
Abstract
Spiritual care is important in nursing practice, and spiritual well-being and spiritual care are associated with better health. Military veterans, a unique patient population, want spiritual care to cope with chronic conditions. It is unclear whether spiritual care is provided in veteran health care in the United States. This study used a qualitative descriptive method, guided by the Spiritual Care in Nursing Practice (SCNiP) theory, to describe spiritual care in nursing practice and facilitators/barriers in veteran health care. Individual interviews were conducted with 39 registered nurses (RNs) at a U.S. veteran health system. Findings were consistent with the SCNiP theory but revealed additional categorical attributes and processes as it applied to veteran health care. Facilitators that promoted spiritual care include nurse professionalism, collegial support, and available spiritual resources. Barriers included lack of time, task-oriented culture, unclear knowledge of accessing resources, and unclear organization policy in providing spiritual care. Findings further refined the theory.
Spirituality is defined as a dimension of self that searches for meaning and purpose in life, transcends time and space, and is the source of connections within oneself, between individuals, and to a higher power (Burkhart & Hogan, 2008; Burkhart & Schmidt, 2012; Herdman & Kamitsuru, 2014). Spirituality is a universal dimension of being human, which differs from religiosity, in that religion is a set of faith beliefs and practices associated with a faith tradition. Many individuals live out their spirituality through faith traditions, but many search for meaning and purpose in life outside of religion (Herdman & Kamitsuru, 2014). Systematic reviews indicate the importance of spirituality in promoting physical, psychological, and social dimensions of health (Goncalves, Lucchetti, Menezes, & Vallada, 2017; Lewinson, McSherry, & Kevern, 2015).
Spiritual care is a purposeful process of helping others to promote their spirituality, particularly to cope in stressful times (Burkhart & Hogan, 2008; Steinhauser et al., 2017). For centuries, nurses have recognized the importance of spirituality in promoting health by integrating spiritual care in nursing practice (Calabria & Macrae, 1994). Spiritual care continues to be recognized as important in modern nursing practice and education (American Association of Colleges of Nursing, 2009; American Nurses Association, 2010, 2015).
Many nursing curricula lack spiritual care education, and nurse educators frequently describe feeling unsure how to teach the timing and content of spiritual care (Wu, Tseng, & Liao, 2016). Consequently, practicing nurses describe low self-efficacy in how to integrate spiritual care into nursing practice (Balboni et al., 2017). In addition, professional standards do not provide guidance in how to provide spiritual care or collaborate with chaplains. As a result, while registered nurses (RNs) have a professional obligation to provide spiritual care, it is unclear how spiritual care is provided or should be provided (Balboni et al., 2017). Nursing theory and research can help provide guidance to integrate spiritual care in practice.
Nursing care is provided within a health system; therefore, spiritual care integration must not only adapt to patient spiritual needs but also be compatible with health system mission and organizational culture (Burkhart, Solari-Twadell, & Haas, 2008). A patient population with unique needs and culture are military veterans (Steinhauser et al., 2017).
Veterans want spiritual care from their health care providers and seek out spiritual practices to cope with mental health disorders, life-changing situations, and chronic disease (Bonner et al., 2013; Jones, Simpson, Briggs, & Dorsett, 2016; Zhang, 2017). Research has shown that spiritual practices (e.g., daily spiritual experiences, forgiveness, and religious practices) among veterans have significantly and positively affected symptoms related to posttraumatic stress disorder (PTSD), suicide, depression, anger/aggression, anxiety, and quality of life (Smith-MacDonald, Norris, Raffin-Bouchal, & Sinclair, 2017) and can facilitate individual and family adjustment to chronic disease (Jones et al., 2016). It is important to address military veterans’ spiritual well-being, particularly during times of crisis (e.g., poor diagnosis or prognosis).
Military veterans engage in their own spiritual practices to cope with stressful times and memories of military experiences (Smith-MacDonald et al., 2017). These practices can lead to positive coping (e.g., finding meaning in situations, hope for the future) or negative coping (e.g., feelings of guilt or punishment for past behaviors). In a systematic review of research related to veteran spirituality, Smith-MacDonald et al. (2017) found that although positive spiritual coping was associated with better health indicators, negative spiritual coping had a stronger relationship with poor health indicators. This indicates that veterans engage in and value spiritual practices, but not necessarily in a healthy way. Nurses are in a unique position to facilitate positive spiritual coping during times of crisis.
Research indicates that veterans may welcome spiritual care, but little research exists to guide how spiritual care is provided. Chaplains are experts in providing spiritual care, and the U.S. Department of Veterans Affairs (VA, 2016) policy specifies that only chaplains can conduct a spiritual assessment and provide spiritual counseling. However, the chaplain is not always available, and this policy lacks clarity, suggesting siloed care excluding all other providers from addressing veterans’ spiritual needs.
The health care professional available 24/7 is the RN. In general, RNs recognize spirituality and spiritual care as an important aspect of health and health care, and providing spiritual care is a professional expectation. At the same time, VA RNs are experiencing low work satisfaction (U.S. Office of Personnel Management, 2017). This problem may be mitigated in part by facilitating nurses to deliver spiritual care to their patients. Nurses who care for patients with complex conditions have cited environments that support the provision of spiritual care as fulfilling and what keeps them engaged in nursing (Burkhart & Hogan, 2008). Transforming an organizational culture by improving holistic care has the potential to improve both RN and veteran satisfaction. However, coordinated research is needed to develop guidelines to promote spiritual care in an evidence-based way (Smith-MacDonald et al., 2017). At this point, it is unclear how spiritual care is provided spiritual care in VA health care. The aim of this study was to describe spiritual care in nursing practice and reveal organizational facilitators and barriers in providing spiritual care in a VA health care system.
Design
The qualitative descriptive method (Sandelowski, 2010, 2012) was used to describe spiritual care in nursing practice and organizational facilitators and barriers in providing spiritual care in VA health care, guided by the Burkhart and Hogan Spiritual care in Nursing Practice (SCiNP) middle-range theory (Burkhart & Hogan, 2008; Burkhart & Hogan, 2017; Burkhart, Schmidt, & Hogan, 2011). Consistent with the method, initial analysis was guided by theory, and the data-guided modifications of categories as new subcategories, properties, or processes were discovered. The study was approved by the VA health system’s Institutional Review Board and Research and Development Committee.
Sample
A convenience sample of RNs who worked at a large midwestern VA health system was invited to participate in a two-phase study including a spiritual care simulation with a standardized patient, followed by a one-on-one qualitative interview to explore spiritual care in VA nursing practice (Desmond, Burkhart, Horsley, Gerc, & Bretschneider, 2018). Qualitative interviews were conducted in summer 2016. Inclusion criteria was working >0.5 FTE (full-time equivalent) as an RN and caring for veterans with chronic conditions, as patients with chronic conditions have high spiritual needs (Smith-MacDonald et al., 2017). Recruitment included a broadcast email inviting all staff RNs employed at a midwestern VA (inpatient and outpatient) to participate in the study, followed by presentations at staff meetings without managers present. Those interested in participating contacted the research team, with one participant declining at the time of the interview after the simulation. Consent was obtained in a two-step process: once over the phone prior to scheduling the simulation and the second immediately prior to the simulation. The sample was recruited within 1 month.
Participants’ (n = 39) mean age was 53 years (SD = 8.8), were mostly female (92.5%), and highly educated (55% bachelors, 25% masters). Most were Caucasian (53%), followed by Asian (32%), Hispanic (13%), and African American (2%). Participants’ work units were inpatient (30%), surgery (22%), outpatient (33%), and outpatient mental health (15%) settings.
Procedure
Participants initially engaged in a spiritual care simulation with a standardized patient. The simulation is reported elsewhere (Desmond et al., 2018). Immediately following the simulation, the participants met individually with a qualitative researcher for an interview, lasting 30 to 60 minutes. Interview questions provided an opportunity to reflect on the spiritual care simulation experience, describe spiritual care in VA health care, and identify organizational facilitators and barriers in providing spiritual care (Table 1). Interviews were audiotaped, transcribed, and analyzed using descriptive coding guided by the SCiNP theory with an inductive–deductive approach to discover facilitators and barriers in providing spiritual care using constant comparison methods (Glaser & Strauss, 1967; Saldana, 2016; Sandelowski, 2010; Sandelowski, 2012). Consistent with the qualitative descriptive method (Sandelowski, 2010, 2012), coding was initially guided by the categories in the SCiNP theory, but data-guided modifications of categories as new properties were discovered, particularly as applied to VA health care. Two qualitative researchers analyzed the data individually and compared the results to maximize fidelity and credibility until 100% of the codes were agreed upon by both coders, using constant comparison methods until saturation was reached. Findings were then brought to the research team (an expert in spirituality and VA nursing education) to finalize the categories. Data-guided emerging modifications to the SCiNP categories, subcategories, and properties as revealed in VA health care were discovered.
Interview Questions.
Results
The definition of spiritual care in VA nursing practice that emerged from the data was consistent with the existing definition outlined in the SCiNP theory (Burkhart & Hogan, 2008): a purposeful process of the nurse recognizing a patient cue in the moment, making a decision to engage or not engage in spiritual care, and providing spiritual interventions. Providing spiritual care affects the nurse as an emotional response followed by reflection, leading to a spiritual memory that affects the nurse’s spiritual well-being. Nurse participants recognized Cues from the Veteran Patients indicating a spiritual need in the moment of care, followed by the nurses’ Decision to Engage or Decision Not to Engage in Spiritual Encounter, depending on organizational facilitators and barriers. Figure 1 identifies those organizational facilitators that promoted the decision to engage and barriers that discouraged the decision to engage the veteran patient. If the nurse chose to engage the patient, she or he provided Spiritual Care Interventions that included being with the patient holistically, determining spiritual need, and performing actions to address the spiritual need. Organizational resources support the provision of spiritual interventions, but barriers exist in accessing those resources and collaborating with chaplains. Nurse participant responses primarily developed the first part of the theory that describes the nurse–patient spiritual encounter, but responses also identified strategies to promote spiritual care that relate to the RN Search for Meaning in Encounter category. Those strategies included providing opportunities for nurse reflection through retreats and creating physical space for reflection.
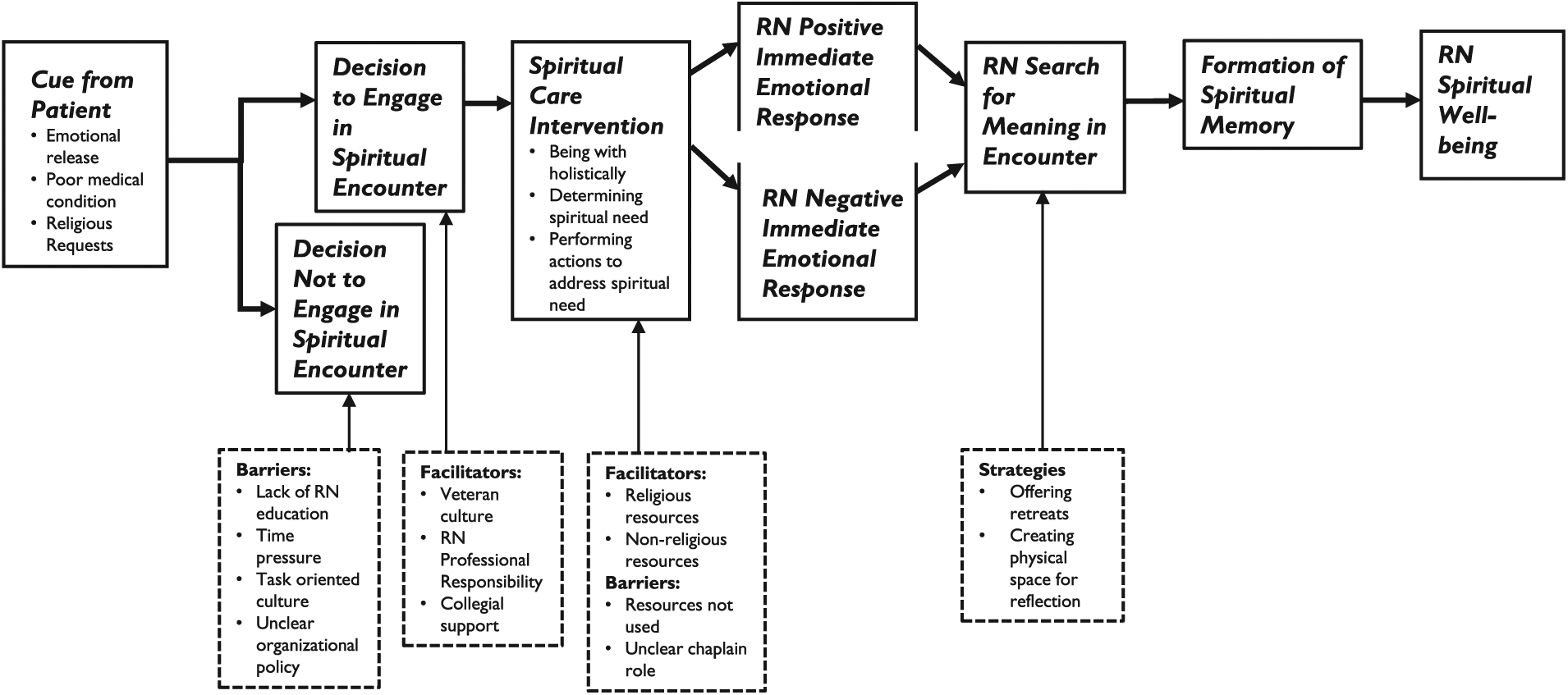
Spiritual care in nursing practice theory applied to veteran health care.
Cue From the Veteran Patient
Participants indicated that nurses enter veteran patient encounters with an awareness of veteran’s unique spiritual needs due to their military experiences, including violence, moral injury, and struggling with PTSD: “So many of our veterans have been exposed to such trauma and atrocities and abuse.” “They’ve seen something that is horrific, and I feel like they’ve had moral injury.” Participants agreed that cues for spiritual needs include an emotional release, responses to a poor medical condition, and religious words or a request for assistance with faith practices.
Emotional release
Participants recognized a potential spiritual need as a verbal or nonverbal emotional release, which includes anxiety and agitation: “They could be so anxious when they keep on calling the call button.” Many veterans express fearfulness and may cry: “He kind of opened up about his fears and then he was crying” or through a burst of anger, “just escalate and can be rather abusive and that’s really more of a form of spiritual distress.” Participants also recognized a nonverbal cue for a potential spiritual need as a blank stare: “There’s no soul. You look in their eyes and there’s nothing. It’s like blank.”
Poor medical condition
Situational cues can indicate a spiritual need. These include a poor prognosis, diagnosis, or medical complications: “starting to have more medical complications. That usually does trigger more of the spiritual issues.”
Religious requests
Participants also learned of a spiritual need when the veteran requested prayer or assistance with engaging in faith rituals (e.g., Islamic prayer rituals). The admission documentation facilitated this cue by including a question about religious/spiritual needs and offering a chaplain referral. Participants also recognized a spiritual need when veterans used religious references: “I thought that my God wouldn’t do this to me. How could He be so cruel?”
Decision to Engage/Not Engage
After recognizing a cue indicating a spiritual need, participants described organizational facilitators and barriers that created a decisional tension that affected the nurse participant’s choice in engaging or not engaging in addressing the spiritual need. If the nurse decides to not engage the patient, the process stops and spiritual interventions are not provided.
Facilitators that promote decision to engage
Organizational facilitators that encourage RNs to engage the veteran in spiritual care are veteran culture, RN professional responsibility, and collegial support.
Veteran culture
Being a veteran is a meaningful identity that connotes patriotism, pride, and camaraderie. “They [veterans] need to know that what they did mattered, that they didn’t do it just for a paycheck. I mean, their whole life, that’s their persona.” Participants agreed that the veteran culture is different than the civilian sector and requires a meaningful recognition and attention to that culture as part of nursing care: “Veterans are very proud of their service. It’s a different feeling here . . . very patriotic and symbolic. In a way, it’s spiritual.” Veterans’ spiritual needs “are different than the rest of the population” and need to be addressed.
RN professional responsibility
Participants consistently recognized that incorporating spiritual care is their “responsibility as a nurse.” “It’s my profession.” “This is what nursing is all about.” The nursing professional ideal includes the importance of integrating spirituality into practice. “That’s why a lot of us went into nursing is to make that connection with people.” “So, there’s like a spirituality that’s more than human, and you try to get into that and to help people.” Participants consistently recognized spiritual care as a professional responsibility.
Collegial support
When participants engage in spiritual care, their nurse colleagues would “not be upset,” “nobody will object to this,” and “managers would support taking time for this type of care.” Participants also recognized that other professionals collaborate as a team that incorporates veteran spiritual issues: “We have a collaborative team . . . the psychologist is on board, the license clinical social worker’s on board, the physician, the pharmacist, the nurse, PT [physical therapist]—whatever element is needed, we have it in place.” Participants also indicated that nurse colleagues also care for each other’s spiritual well-being: “We support each other, and we could talk to each other.” Nurses also provide guidance in helping each other to provide spiritual care: “I think we are just expected to turn to our peers and receive supervision from our peers.” Participants agreed that colleagues allow spiritual care to occur, and RNs support each other spiritually.
Barriers that discourage decision to engage
Organizational barriers that discourage RNs to engage the veteran in spiritual care are lack of time, a task-oriented culture, lack of education in providing spiritual care, and unclear organizational policy in providing spiritual care.
Lack of RN education
VA nurses did not receive training to provide spiritual care in the health care institution, and many indicated little to no spiritual care education in nursing school: “I don’t know if we were ever trained to address spiritual needs in nursing” and “you are not taught it. It’s not in the educational tool here.” Nurses who were comfortable with providing spiritual care were self-taught: “It just self-development from my own—reading the books, listening to the things” or through experience, “I think I’ve had sufficient training and life experiences to do that.” Participants agreed that they did not receive formal training in providing spiritual care.
Time pressures
Many perceive a lack of time to provide spiritual care due to workload: “If they have four or five patients, some nurses won’t take the time to sit down and talk to their patient because they’re so overwhelmed.” High patient acuity also limits the time for spiritual care: “There are patients, maybe five or six—some of them are very sick. I definitely say the time matters.” Nurses feel a time pressure to address other patient’s needs: “You don’t feel comfortable spending more time with him, because the other patients are all waiting.” Participants consistently cited actual time and the perception that spiritual care requires too much time as barriers.
Task-oriented culture
Many VA nurses support a “task-oriented” culture as more important than providing holistic care: “Some of them are very driven at vitals . . . but then you miss the whole person during all that stuff.” The focus is more related to physical needs, and spiritual needs are not considered: “I think we focus mostly on the physical aspect of patients’ care. I don’t think we focus on spiritual care.”
Unclear organizational policy
Participants consistently stated that spiritual care is not discussed within the organization or considered part of the care process: “It’s not talked about,” “It’s something that’s not really pushed here,” and “never see the nursing ever, doctors ever, I have never seen them even discussing to the point.” Participants also questioned whether providing spiritual care was consistent with organizational policy: “I don’t want to upset anyone or break the rules,” and “You cannot talk spirituality. You cannot do that.” Participants found that the organizational policy was either silent or participants perceived that spiritual care was disallowed.
Spiritual Interventions
If nurses choose to engage the patient, participants described a process of providing spiritual interventions that included using oneself therapeutically by being with the patient holistically, determining the veteran spiritual need, and performing actions to address those needs. There are also facilitators and barriers to affect spiritual interventions.
Being with the patient holistically
The process of providing spiritual interventions was described as a “holistic experience” and addresses “the spirituality of the inner, the life source of a person.” This approach includes “Just being present is taking care of the spiritual.” This process is intentional to build a relationship: “Taking the extra time and develop a trust relationship with them.” Participants agreed that all humans are connected and being with a patient holistically includes connecting therapeutically: “Connecting with the person, I think that’s fundamentally what spirituality is, is getting out of myself and being with another person.” Once the connection is established, participants agreed that the initial process includes communicating concern, care, and respect: “Showed them the love and the care.” Spiritual interventions begin with a therapeutic holistic connection between patient and nurse to convey care, concern, and respect that helps develop a trusting relationship.
Determining spiritual need through active listening and probing
Nurses actively engage in listening to patient concerns: “Listen to the cares of the patient,” “Listen carefully to what the patient says,” and “He needed somebody to listen to him, and I was able to provide him with that.” Listening also includes determining the patient’s spiritual needs: “Identify and be able to discuss with a patient how that affects them.” This probing includes determining “Where they get their strength from and their peace from,” while also respecting “Whatever their beliefs are, to be in tune with them.” This includes “What kind of religion they have.” Participants agreed that once a holistic connection is made, the nurse identifies the veteran spiritual need by actively listening and probing to determine that need.
Performing actions to address the spiritual need
Participants identified actions that address veteran spiritual needs. These include promoting hope, encouraging self-reflection, facilitating spiritual practices, promoting support from others, and initiating referrals to other providers or the chaplain.
Promoting hope through self-reflection
Participant nurses assist the patients to reframe their situations in a hopeful way: “I tried to give him some hope, and I think that was spiritual in a sense—giving him something to hang onto,” “To have a positive assurance for everything in their lives,” and “Positive support, attitude, positive thinking.” Nurses encourage patients to find hope and peace through reflection: “Just taking time out and reflecting is more spiritual.” Reflection helps find “The peace you make with yourself and whatever else is out there.”
Facilitate spiritual practices
Veterans frequently identify religious or nonreligious spiritual practices that help them cope. Participants agreed that nurses encourage patients to find strength in their faith beliefs, when appropriate: I think just trying to figure out where someone is at with their relationship with God and their faith and how much that that gives them comfort and how much it gives them strength and courage and encouraging them to utilize their spirituality.
When asked, nurses integrate prayer: “We kind of prayed silently.” Participants also indicated that veterans find meaning through art, music, and nature. Therefore, nurses “Encourage them [veterans] to look at creativity, music, nature—trying to help the person, again, look outside of themselves.” Nurses also use “the TV channel they have with the nature and the music . . . I think beauty does help.”
Encourage support from others
Nurses provide spiritual interventions by encouraging connection with others as a source of strength. They provide that connection themselves by “Reassuring them that we never walk alone” and “I’m on your team and I want you to get better.” Nurses also recognize that veterans “find spirituality in their relationship whether it be with their dog or with their neighbor” or “how they get their support from their family member.” Participants also identified faith communities or community social groups as a source of spiritual support: “Getting them in the community if they are in the community—maybe there’s a Bible study somewhere that they are not aware of, or even someone’s home—searching out, getting resources in the community.”
Initiate referral to other professionals
When patients are in spiritual distress, some nurses offer to call the chaplain, particularly if the veteran indicates a religious need: “I would just call the chaplain . . . it’s more religion-directed.” If the patient does not have a faith belief system, they initiate referrals to the social worker: “I was focused more on social services.” Participants agreed that they would “look for a pastor, a volunteer, somebody who can spend a block of time.”
Facilitators in providing spiritual interventions
Organizational facilitators in providing spiritual interventions included the availability of religious and nonreligious resources.
Religious resources
Participants consistently identified organizational facilitators that support religious and spiritual interventions. Religious resources include “a chapel, there is Mass every day” and veterans “can watch it [religious services] on TV.” Participants also knew of chaplain services, “the chaplain did say in a meeting one day, that ‘We are available for everyone.’ I think that the systems are here in place.” Chaplains regularly visit certain units. On those units, participants agreed that veterans “really enjoy conversation with the chaplains. I think it’s very helpful for them.” Participants felt that the organization had professional resources to help address veteran religious and spiritual issues.
Nonreligious resources
Nonreligious resources exist to address spiritual needs, particularly when the veteran refused a chaplain visit: “Some people they may say, ‘No, I don’t want to see . . .’ So, then we have another resource like social worker, they can talk or a psychologist available—they can talk, but not from the chaplain side.” There are also programs to engage veteran volunteers to meet with veteran patients. Recognizing the importance of the veteran culture, the organization has a peer volunteer program to help address patients’ spiritual needs: “Volunteers that come in and do one-to-one to sit with dying patients, that’s an excellent program.” Participants identified motivational interviewing and healing touch initiatives as forms of spiritual care, as well as yoga, acupuncture, mindfulness meditation, sleep hygiene, wellness workshops, and stress management.
Barriers in providing spiritual interventions
Organizational barriers in providing spiritual interventions related to lack of knowledge and use of spiritual care resources and collaboration with pastoral care chaplain services.
Spiritual care resources not used
Although many participants recognized organizational resources that support spiritual care, many other participants were unsure how to access those resources: “There’s a lot of opportunities and a lot of services offered to the veterans and a lot of times we don’t have complete knowledge of everything there is offered to them.” Participants also cited that nurses do not access those services: “We have a lot of [spiritual] resources. I don’t know that we always utilize those resources that well” and “We don’t talk about that in our team meetings or we don’t talk about those [spiritual] resources.”
Unclear chaplain role
Participants were unsure of the chaplain role. Although participants agreed that chaplains are a potential resource, they viewed the chaplain as only a religious resource. Chaplains are “the Sunday people, they make rounds.” Participants perceived that the chaplain role is to pray with the patient: “They come around and they give the Host and they say a prayer and that’s it.” Participants also recognized chaplain services in limited situations, “only in the dying process and the palliative care if the family requested it.”
Chaplains are an external resource and were not often contacted: “I don’t have a ton of experience with chaplains.” Participants did not understand chaplain services, believing that chaplains were associated with specific religious denominations: “I don’t know how, if the chaplain is open to all beliefs?” There was discomfort in contacting chaplains, as chaplains do not engage with the health care team: “If they were more present I guess, talk to us—get to know us . . . I don’t even know their names. It just feels a little weird.” Participants agreed that chaplains are underutilized.
Recommended Organizational Strategies for Spiritual Care
Participants agreed that spiritual care should be made a priority, and VA initiatives to promote spiritual care should focus on nursing education and promoting access to current spiritual care resources. Spiritual care needed to be integrated in care systematically and participants recommended establishing a committee to develop guidelines and clarify policy and procedure to integrate spiritual care into workflow. Participants also recommended providing opportunities for nurse reflection, including retreats: “nurses need some spiritual healing too . . . some kind of retreat would be good for nurses.” Participants also recommended creating physical space for reflection, “a generic quiet serenity room, and family or staff could utilize it.” These latter two recommendations are consistent with the RN Search for Meaning in Encounter category in the theory (Figure 1).
Strengths and Limitations
Participants’ rapid response to recruitment, within 1 month, and their willingness to engage in a 2-hour study supports the notion that RNs in the VA find the topic of spiritual care to be important. An additional strength was the large sample size and the breadth of the clinical experience, including in both inpatient and outpatient sites. Another strength of the study is that all participants experienced the same spiritual care simulation prior to the qualitative interview, thereby providing a common comparison with their own practice. The simulation included patient cues and spiritual interventions derived from the literature and were psychometrically validated for the simulation study to promote conceptual clarity (Desmond et al., 2018). A limitation is that participants who came forward may value spiritual care and may not represent the entire VA RN population. The sample also represented nurses with higher education (25% masters) than typical RNs at the VA, which may have affected the results. Also, participants were recruited from one Veterans Integrated Service Network (VISN), which may not be consistent with other VISNs. However, findings from this study can guide quantitative research to determine generalizability. Additional research is also needed to further develop organizational initiatives to promote spiritual care.
Discussion
Participants agreed that spiritual care in VA health care is a purposeful process of recognizing a patient cue, choosing whether to engage the patient and provide spiritual interventions in the moment of need. However, study findings provided a more specific application of the theory categories to the veteran population, integrating military experiences and the VA organizational culture. It is also interesting to note that participants recommended organizational strategies to promote nurse reflection post spiritual encounter, which is consistent with the SCiNP theory, in that spiritual care does not end with the nurse–patient spiritual encounter, but continues to affect the nurse. More research is needed to further develop these organizational strategies. The original theory also associates the post spiritual encounter process (RN Positive/Negative Immediate Emotional Response, RN Search for Meaning in Encounter, Formation of Spiritual Memory, RN Spiritual Well-being) with the Decision to Engage in Spiritual Encounter in that choosing to engage the patient is affected by nurse’s spiritual well-being. This relationship is unclear in this study, and more research is needed to further develop these categories and clarify this relationship.
This study revealed additional categorical attributes and processes of spiritual care, beyond what was identified in the SCiNP theory, as it applies to veteran care. Similar to the SCiNP theory, patient cues of spiritual need included a verbal and/or nonverbal emotional release, a direct request for religious resources, and the situational cue of a poor diagnosis or prognosis. However, participants agreed that this population has a greater spiritual need due to past traumatic military experiences, which is consistent with the literature (Smith-MacDonald et al., 2017). Also, similar to the theory, the decision to engage the patient is influenced by lack of time and collegial support. Findings suggest that there are many additional organizational barriers to providing spiritual care. Organizational policy and a task-oriented culture are barriers that can lead to a decision to not engage in spiritual interventions. It is interesting to note that participants did not indicate spiritual exhaustion as a barrier. However, spiritual exhaustion presupposes that nurses consistently provide spiritual care, which may not be the case. More research is needed to clarify how much spiritual care is provided by nurses in the VA.
The initial grounded theory research (Burkhart & Hogan, 2008) with RNs indicated that the nurse engages in three types of spiritual interventions: promoting connections with self, others, and/or a higher power. This study further developed the SCiNP theory, discovering a three-step process of providing spiritual interventions that begins with being present and connecting with the patient holistically to build a trusting relationship. The nurse then listens and further probes to determine the spiritual need and then provides an appropriate spiritual intervention. This three-step process is consistent with spiritual intervention research (Kostovich, 2012; Mamier & Taylor, 2015; Vincensi & Burkhart, 2016).
Although VA health care has resources to help provide spiritual care, several barriers exist that inhibit spiritual care. VA health care lacks chaplain integration into the health care team. Although VA policy indicates that chaplains are responsible for spiritual care, that role is separate from other health care team members and has led to a siloed approach in providing spiritual care. Also, nurses, who are present at the moment of need, lack the formal education in addressing spiritual needs and lack the knowledge of available spiritual resources. Although available, many spiritual care resources are unknown, unused, and not integrated into health care processes. Opportunities exist to create an integrated strategy to address veteran spiritual needs among the health care team. For example, nurses currently provide compassionate, holistic care and can identify spiritual needs in the moment. When educational programs and resources are in place, nurses can further assess the need and access resources to address the need. This can include referral or collaboration with the chaplain. When organizational policies are clear and the nurse and chaplain roles are more clearly defined, spiritual care processes can be integrated into workflow, and handoffs to chaplains can be smooth. When developing initiatives designed to improve veteran care, it is also important to explore veteran perspectives of spiritual need and interventions (e.g., focus groups) to ensure spiritual care initiatives meet patient needs and are acceptable to the patient. The VA is currently piloting a Whole Health initiative to foster continuous healing relationships between veterans and providers that integrate physical, mental, emotional, spiritual, and environmental dimensions of health into health care (U.S. Department of Veterans Affairs, Office of Patient Centered Care and Cultural Transformation, 2018). Creating and implementing educational programs and a clear process in providing spiritual care that are consistent with RN professional standards and meet veteran needs has the potential to improve whole person veteran care.
Conclusion
Each health care institution has its own organizational culture. Although the VA is a national health care system, no one VISN is representative of all VISNs. However, to effect change in improving care requires a deeper exploration at the institutional level. Health systems can use qualitative descriptive research to reveal institution-specific care processes, population-specific needs, and facilitators and barriers to promote quality care. Specifically, this study described SCiNP in VA health care and identified opportunities to improve spiritual care for veterans at the moment of need, improve interprofessional collaboration with chaplains, and clarify organizational policies and procedures to better meet veteran whole person health.
Footnotes
Acknowledgements
Thank you to Bella Etingen, PhD, Research Health Scientist, Center of Innovation for Complex Chronic Healthcare, Hines VA Hospital for reviewing and editing the initial manuscript draft.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study, “Research to Support an Organizational Culture of Spiritual Care in VA Patient Care,” ONS 101, was funded by the Department of Veteran Affairs, Office of Nursing Services.