
Abstract
In this study, we examined the sociocultural factors underlying infant feeding practices. We conducted four focus groups with 19 Latina mothers of children 0 to 2 years of age enrolled in Early Head Start programs in the United States over a 1-year period. We found these mothers considered both science- and family-based feeding recommendations. However, advice from family was often inconsistent with science- and nutrition-based recommended feeding practices. In the interest of showing respect and preserving harmonious relationships, some mothers accepted family advice instead of recommended practices while others employed strategies to follow recommended practices without offending. Nutrition educators need to consider the intersection of macro, organizational, and community factors with micro-level processes in shaping the implementation of recommended feeding practices within family systems. Nutrition interventions for Latino families should capitalize on Latina mothers’ strategies for navigating multiple information sources while preserving cultural values and family relationships.
Keywords
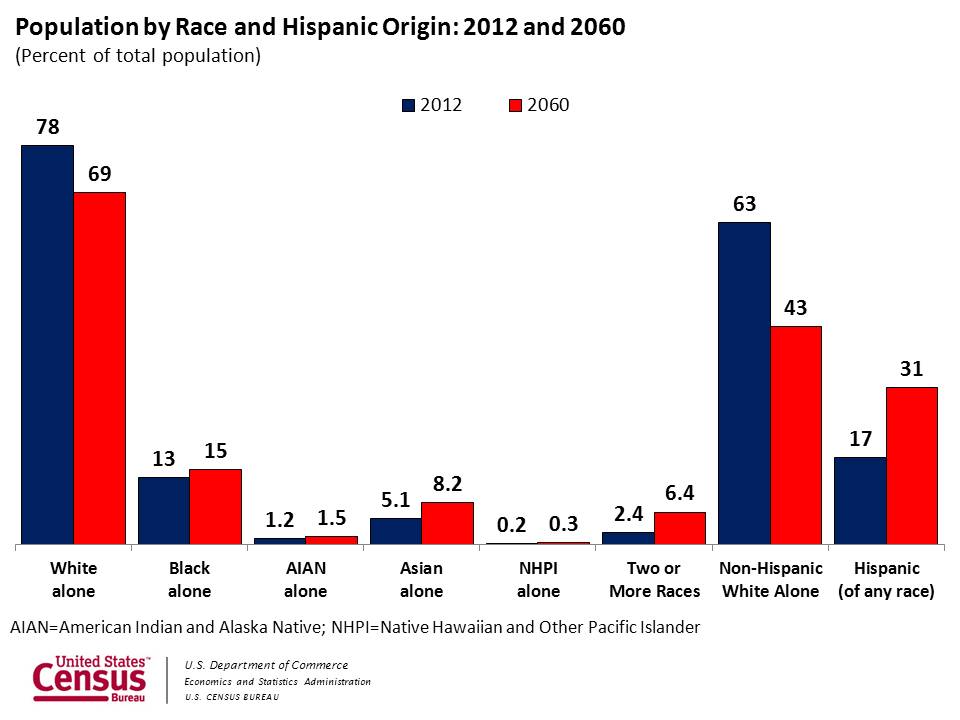
Latino children are a fast growing, disproportionately obese segment of the U.S. population. An estimated 21.2% of Latino children and adolescents are obese compared with 14% of White non-Latinos (Ogden, Carroll, Kit, & Flegal, 2014; de la Torre, et al., 2013). Obese children are at elevated risk for diabetes, cardiovascular disease, and other serious chronic illnesses (Juonala et al., 2011; Pulgaron & Delamater, 2014). As it is projected that by 2030 nearly one in three U.S. children will be Latino (U.S. Census Bureau, 2014b), and as obesity increases morbidity and mortality, health care costs, and health disparities (Dobbs et al., 2014; Ebbeling, Pawlak, & Ludwig, 2002; Finkelstein, Trogdon, Cohen, & Dietz, 2009), there is a need to address this public health concern.
Desirable changes resulting from obesity interventions in late childhood and adolescence (e.g., increased physical activity, consumption of nutrient dense foods) have proven difficult to sustain over time (Alexander, Grant, Pedrino, & Lyons, 2014). Interventions in infancy and toddlerhood, especially within family contexts, may mitigate excessive weight gain in childhood and reduce risk for morbidity and mortality across the life span (Altman & Wilfley, 2015; Sharifi et al., 2014; Shirley et al., 2015). Researchers and practitioners have developed interventions to reduce early childhood obesity risk among children 2 years of age and younger (Ciampa et al., 2010).
Arikpo, Edet, Chibuzor, Odey, and Caldwell’s (2018) systematic review highlighted a number of these randomized controlled trials of educational early childhood infant feeding interventions aimed to curb early childhood obesity risk, including the Early Childhood Obesity Prevention Program, and the Infant Feeding and Activity and Nutrition Trail (Infant Extend). However, based on their analysis of these and complementary feeding interventions, they found limited evidence that such interventions improve feeding practices and insufficient evidence to demonstrate positive intervention effects on growth outcomes. This body of research suggests additional work is needed to improve the effects of educational interventions on infant feeding practices and child growth outcomes. One way to do this is by considering the social and cultural factors driving infant feeding practices (Lumeng, Taveras, Birch, & Yanovski, 2015).
Research shows that Latino parents’ feeding practices often deviate from recommended guidelines. For example, although scientific guidelines recommend exclusive breastfeeding for the child’s first 6 months (World Health Organization, 2001), some Latina mothers report formula feeding or combination feeding (giving breast milk and formula simultaneously) within the first few months (Bunik et al., 2006; Flores, Anchondo, Huang, Villanos, & Finch, 2016; Higgins, 2000). Guidelines also recommend solid food introduction after 6 months, but some Latino parents introduce solid foods earlier (Kuo, Inkelas, Slusser, Maidenberg, & Halfon, 2011).
Finally, guidelines for infants and toddlers determine food quantity (e.g., how much they should eat) together with awareness of satiety cues. Latina mothers are more likely than White or Black parents to encourage their infants to finish a bottle, whether or not the child shows signs of satiety (Perrin et al., 2014). Such feeding practices are associated with childhood obesity risk and are targets of obesity prevention efforts (Huh, Rifas-Shiman, Taveras, Oken, & Gillman, 2011; Koletzko et al., 2009; Lumeng et al., 2015).
To date, only a handful of obesity prevention interventions target children 2 years of age and younger. These interventions largely promote healthy dietary behaviors and physical activity and consider child dietary health outcomes and parents’ nutrition knowledge and attitudes (Ciampa et al., 2010; Sanders et al., 2014). They do not consider culture, family dynamics, or the meaning of foods. Infant feeding is a complex practice shaped by multiple factors (e.g., conflicting advice from family, friends, and health care professionals; stigma; and social norms; Guell, Whittle, Ong, & Laksham, 2018). Furthermore, low-income families may obtain nutrition education through government-sponsored child and maternal health programs, which focus primarily on promoting nutrition and infant growth, not preventing obesity, and which emphasize the biological aspects of nutrition with little attention to culture and the social context of feeding. As a result, even when knowledgeable about nutrition, parents may engage in nonrecommended feeding practices (Crocetti, Dudas, & Krugman, 2004).
Theoretical Framework
We draw on the Family Ecological Model (FEM), which situates infant feeding and child health within multiple social systems of influence. We use this model to contextualize individual-level infant feeding, growth, and obesity within a social ecological context. The FEM provides structure to examine how factors embedded within social systems of influence (macrosystem, community, organizational factors) intersect with the family social and emotional context and parenting behaviors and practices to shape child health outcomes. For example, mandates of public assistance and health information sources at the macrosystem, community factors involving access to healthy foods and availability of community programs and services, and provision of childhood education programs and parent work demands at the organizational-level intersect with the family context to shape child health outcomes (Davison, Jurkowski, & Lawson, 2013). We use this structure to highlight the multiple factors across systems that shape ideas about child health and infant feeding, access to nutrition education, and the application of nutrition education into Latino family systems.
We know that social and cultural factors influence Latino child socialization and health outcomes (Calzada, Huang, Anicama, Fernandez, & Brotman, 2012; Counihan, 2009). Acculturation, a key variable associated with many health outcomes (Lara, Gamboa, Kahramanian, Morales, & Hayes Bautista, 2005), shows that less acculturated Latinos exhibit more nonresponsive infant feeding practices, meaning that caregivers may not respond appropriately to infants’ verbal and non-verbal feeding needs and signals (Dancel et al., 2015; Evans et al., 2011; Sussner, Lindsay, & Peterson, 2009). As others noted, understanding variation in infant behaviors within a sociocultural context can inform the identification of risk groups and the tailoring of interventions to them (Lumeng et al., 2015).
By considering the sociocultural context, we also consider the meaning of feeding activities. In contrast with prior research, we conceptualize feeding as a social and biological activity. Nutrition education was built on a biological model and focuses on nutrient intake and energy expenditure. We acknowledge that feeding also provides an opportunity for people to fulfill social roles, transmits culture via consumption of culture-specific foods, and teaches such behavioral norms as how to show respect (Padilla, 2006).
Furthermore, we consider how sociocultural factors shape the translation of nutrition education into practice. Despite existing knowledge that infant feeding practices are embedded within sociocultural contexts (Chaidez, Townsend, & Kaiser, 2011; Higgins, 2000), there has been little attention to understanding how these factors shape the translation of nutrition education to practice in the home (Schafer, Williams, Digney, Hare, & Ashida, 2016). Thus, this article fills existing gaps in the scientific literature by qualitatively describing Latina mothers’ infant feeding practices and identifying social and cultural factors (e.g., knowledge, values) driving these practices.
Method
Setting
This interdisciplinary research brought together investigators with disciplinary training in anthropology, pediatrics, psychology, psychiatry, and sociology, as well as engaged local community partners in Riverside and San Bernardino counties’ Early Head Start (EHS) programs.
Our study used principles of community-based participatory research (CBPR) and involved a collaborative approach combining the strengths of diverse partners and emphasizing equality in the research partnership (Minkler & Wallerstein, 2008). The research is a partnership between the University of California, Riverside School of Medicine’s Center for Healthy Communities and EHS programs in Riverside and San Bernardino Counties. The research focused on the context of food and feeding in low-income Latino families and sought to generate ideas for the development of early childhood obesity prevention programming grounded in mothers’ experiences. The University of California, Riverside Institutional Review Board (IRB) approved all procedures prior to the start of the research.
From fall 2015 to spring 2016, we conducted four focus groups with Latina mothers enrolled in one of two federally funded EHS programs in Inland Southern California. Located east of Los Angeles, Inland Southern California refers to the Riverside-San Bernardino-Ontario region (The Community Foundation, 2015a, 2015b; U.S. Census Bureau, 2014a, 2014b, 2014c). Riverside County is home to more than 1.1 million Latinos, of whom a third are foreign-born (U.S. Census Bureau, 2010). San Bernardino County is home to more than 500,000 Latinos most of whom are foreign-born (The Community Foundation, 2015a, 2015b). In both counties, the majority of Latinos are of Mexican origin with a smaller percentage from Puerto Rico, El Salvador, and Guatemala (U.S. Census Bureau, 2000). Children from low-income Latino families in these counties have some of the highest rates of obesity in the nation (The Community Foundation, 2015b; U.S. Census Bureau, n.d.).
Riverside County EHS has eight sites and enrolls >350 children annually. Three quarters of these are Latino, and more than a third of these families report Spanish as their primary language. San Bernardino County EHS has 15 sites and annually enrolls ~600 children. Half of these are Latino and nearly a quarter of the families report Spanish as their primary language. Programs in both of these counties provide home- or site-based education and support services to low-income pregnant women and mothers of children ages 0 to 3 years. Mothers receive child development and nutrition education and work with a registered dietician if their children experience weight problems.
The nutrition education program follows curricula (i.e., My Healthy Plate and Color-Me-Healthy) that align with the United States Department of Agriculture’s healthy eating practice campaign (see https://www.choosemyplate.gov/), the cornerstone of government-sponsored nutrition programs for low-income parents and children (see https://wicworks.fns.usda.gov/nutrition-education). These curricula encourage healthy eating practices through education on portion control, food diversity, and nutrition content. Classes also include information on parental roles and responsibilities for food preparation and family mealtime.
Participant Recruitment
Participants had to be 18 years or older, self-identify as Latina, and have at least one child 2 years of age or younger enrolled in either a Riverside or San Bernardino EHS program. Following the recruitment approach of other investigators who have successfully engaged EHS and Head Start (HS) families in research (Nepper & Chai, 2017), the study team met with EHS nurses and community assistants to discuss study objectives, outline eligibility criteria, and brainstorm recruitment strategies. EHS nurses and community assistants, who meet weekly with EHS enrolled families, recruited mothers for the study during regular program visits and later contacted them with the day, time, and location of the focus group. If mothers requested, EHS staff provided transportation to the focus group.
Focus Groups
We conducted four focus groups, two in English and two in Spanish. For nonprobability samples, 80% of themes can be identified within two to three focus groups and 90% within three to six focus groups (Guest, Namey, & McKenna, 2017). Data collection and analysis were simultaneous activities. At the end of each focus group, the co-facilitators held a debriefing session to discuss emerging themes, key points documented through note taking, and general observations. We wrote up a summary of this information, which we then used to compare and contrast initial findings across focus groups.
Once the audio recordings were transcribed, we began a more in-depth analysis of the data (described below). We followed Saunders et al.’s (2018) recommendation to operationalize data saturation in relation to the primary research questions and theoretical and analytic framework. We asked the following question: Does the data provide sufficient information to meet the aims of the research? We reached data saturation, meaning new data were redundant and participant responses were similar (Guest, Bunce, & Johnson, 2006), for our primary research question (i.e., What are the social and cultural factors driving child feeding practices in Latino family contexts?), within four focus groups.
Participants were grouped by primary language (English or Spanish dominant). The first English focus group included eight mothers and the second included two mothers. The first Spanish focus group included six mothers and the second included three mothers. The focus groups were held at the EHS offices in a private room and lasted 60 to 90 minutes. Drs. Cheney and Nieri, who speak Spanish, co-facilitated the focus groups.
Prior to the start of the focus group discussion, participants were provided with their own copy of an information sheet that outlined the research, its goals, participant payment, risks and benefits to participation in the study, and the contact information of the investigative team and the university IRB. The facilitators read over this form and provided an opportunity for participants to ask questions. Once facilitators responded to all questions and participants provided verbal consent to their participation and to being audio-recorded, the facilitators began the focus group. Interviews were audio-recorded and transcribed by bilingual student assistants. Participants received a US$25 Target gift card to thank them for their participation. We recognize that gifts or cash payments to research participants is controversial, as it may undermine independent choice, exacerbate social inequalities, and exploit vulnerable populations (London, Borasky, & Bhan, 2012). However, given university policy, we were unable to offer other forms of payment to research participants such as child care.
Based on conversations with EHS community partners, qualitative team members drafted a semistructured interview guide with open-ended questions to elicit information on caregiving practices for ages 0 to 2 years, challenges related to the child’s eating and sleeping patterns for ages 0 to 2 years, strategies to address the challenges, and family and community perceptions of infant growth. For instance, we first asked participants to “Tell us about the first two years of a baby’s life” and used probes to understand commonly involved caretakers (e.g., fathers, grandmothers, babysitters) and their role. We then asked participants to identify and discuss common challenges encountered during the first 6 months of life, probing to elicit specific data on infant feeding (e.g., breastfeeding, formula feeding, solid foods, concerns about infants eating too much or too little), as well as where parents commonly obtain information and knowledge on addressing these issues. Near the end of the group interview, we asked participants to discuss how family and community members think about weight gain during the first 2 years of life using the following question: “Is too much or not enough weight gain during the first two years a concern in your community or family?”
Through our initial analyses, we noted that the women had obtained scientific knowledge on infant feeding from EHS nutrition educators and health care professionals. Consequently, we added an additional question to the interview guide to examine women’s knowledge of scientifically recommended infant feeding practices. In the second English and Spanish focus groups, facilitators listed common feeding practices considered to be obesogenic and not scientifically recommended (i.e., solid food introduction prior to 6 months, formula in lieu of breast milk, serving sweetened beverages, and the use of thickeners) and asked participants to share their thoughts on these practices and describe their use for children aged 0 to 2 years.
Data Analysis
Because this study was exploratory, we used an inductive approach involving line-by-line reading of textual data to identify emergent themes (Ryan & Bernard, 2003). All original transcripts were imported into MAXQDA, a qualitative data analysis software program, and data were coded and analyzed (Verbi Software, 2016). Cheney, who has expertise in qualitative research, led codebook development and analysis.
Following an inductive approach, team members used open coding (line-by-line reading of the text) to identify emergent themes (Corbin & Strauss, 2008). Four team members, including an anthropologist, a medical sociologist, a pediatrician, and a psychologist, read the transcripts line by line, identified emerging themes, and met to discuss a draft codebook. Cheney then drafted the initial codebook, including code definition and exemplar quotes, and presented it to the team (MacQueen, McLellan, Kay, & Milstein, 1998). Once the initial codebook was developed, we independently applied the codes to text segments and met to discuss agreement of code application. This was iterative and the codebook was revised several times.
Throughout the process, the team met regularly to discuss the coding schema and its application to the textual data. Once we reached agreement on the coding schema, Cheney engaged in in vivo coding (i.e., tagging text with codes) and applied the coding schema to all transcripts. Nieri reviewed the application of the coding schema to a selection of tagged text and discrepancies were discussed. Finally, axial coding (i.e., constant comparison) was used to examine the relationships between themes and compare and contrast themes within and across transcripts. Once we identified the main findings, we scheduled meetings with community partners (coauthors in this article) to elicit feedback and insight on the interpretation of the findings and their potential implication for future research.
Results
Participant Characteristics
Nineteen women participated in the research. All women self-identified as Latina, were between ages 18 and 40 years, and participated in either the Riverside or San Bernardino EHS program. Eleven spoke English and eight spoke Spanish as their primary language. Most were of Mexican descent and lived in extended family households (e.g., with in-laws or members of their family of origin). All women had at least one child under the age of 2 years and had anywhere from one to seven children. The central themes that were generated from the analysis are described below.
The presentation of our findings map onto the FEM. We first discuss macrosystem and microsystem interactions, focusing on the intersection of federal nutrition education policy for low-income families, dominant scientific nutrition discourses, and family food knowledge and practices. We then discuss the family social and emotional context, shaped by social disparity and chronic stress. Last, we highlight the intersection of these factors with parenting practices—in this case, infant feeding and child health outcomes.
Macrosystem and Microsystem Intersections
Health information resources and mandates linked with public assistance through the EHS program that entail the delivery of nutrition education to parents enrolled in EHS at the macrosystem intersected with family food knowledge and practices.
Scientific recommendations
Latina mothers described their knowledge of scientifically recommended feeding practices. Many received feeding advice from health practitioners (e.g., pediatricians, nurses, or lactation consultants) and incorporated it into their feeding practices. Health care professionals advised them to feed infants and toddlers nutritious foods and snacks.
A mother of a toddler said, “[The doctor] would say, ‘Don’t give [participant’s daughter] junk food. Try to give her nutritious snacks that are healthier. That will keep her full.’” Her doctor also encouraged her to provide her daughter with protein. Another mother explained how her doctor advised her to breastfeed or provide formula and not to feed infants water: “The doctors told me that it’s not good to give water to babies when they are really young.”
Nutrition education
Through formal nutrition classes, Latina mothers received education on portion control (i.e., feeding an amount of food that meets the need for sustenance based on the child’s age/size), food diversity, nutrient intake (e.g., calories, equal portions of different colors of foods, proteins), and healthy food consumption (e.g., nonprocessed foods). Participants were especially knowledgeable about portion control, as exemplified by one mother’s comment: “We also have nutrition classes, and they teach us how much a portion is.”
Participants also discussed using a “control plate” to measure portions and meal plan. A mother who used a control plate explained, I gave him [her toddler] some shredded chicken. I put a little bit of barbeque sauce on it—it had a portion [size] as well. Then, I put a little bit of light snack popcorn. And, when there’s none [left], I put some pretzels on it, and he will eat the whole thing. And, also add an apple . . .
As this quote evidences, mothers put into practice their knowledge of portion control, food and nutrient diversity (e.g., portions of different colors), and healthy food, rather than street or fast food, consumption. For instance, referring to her nutrition education class, this mother shared, “They taught us that everything has calories even if its fruit . . . I taught my kids that the colors of fruit tell you which fruit is healthier.”
Family Social and Emotional Context
Within the social and emotional context of the family, the social meanings of food and feeding and beliefs about child body size and health shaped child health outcomes and risk for early childhood obesity. As participants explained, they grew up in family contexts shaped by a history of social disparity (poverty, low income, racial/ethnic minority) and chronic stress, specifically around food insecurity. The advice and beliefs of other caregivers, the symbolic meaning of food and feeding, and infant body ideals greatly influenced infant feeding practices.
Trusted caregivers’ advice and beliefs
The mothers identified other caregivers (e.g., family members and babysitters) on whom they often relied for caregiving assistance and from whom they frequently received feeding advice. These people, typically elder women, were generally respected for their childrearing experience and viewed as having valuable expertise. Their advice to mothers and their own feeding practices, when the child was in their care, reflected beliefs that were not always consistent with scientific recommendations or with mothers’ own preferred feeding practices as shaped by government-sponsored nutrition education programs.
For example, mothers discussed generational differences in beliefs and practices associated with portion size. Some caregivers, especially children’s grandmothers, reportedly expect children to eat adult portions and encourage excess eating. The mother of a toddler explained, “In our culture we are used to eating a lot. First comes soup, and then comes rice, then whatever. We eat a lot.” A mother in another focus group shared, “My mom and my grandma used to serve us as adults. To my kids they would serve a plate just like this: full! Like full!” As participants explained, older generations’ perceptions of food and feeding were tied to food insecurity. Because older family members, especially grandmothers, did not want children to suffer as they did, they encourage an abundant consumption of food.
Food as a form of love
Mothers discussed how the meaning of food as a form of love influenced their feeding practices. Reflecting on generational feeding practices in her own family, one mother commented, “I have noticed that generations—my mom, my grandma and me—always offer food as a form of love. And before, if you would not eat it, it would be disrespectful.”
Mothers wanted their children to eat the food prepared for them and expressed concern about children not eating their food. A mother of a toddler said, “If he does not eat what I give him right now, I would have to substitute this food for something that he likes.” Referring to when her son was an infant, she explained, “If I do this right now when he is a baby, it means that later on, he is just going to tell me he does not want to eat any food and he wants something else.”
Perceptions of infants as too thin
According to the focus group participants, solid food introduction prior to the recommended 6 months of age is a common practice in Latino families. The women’s own mothers or grandmothers encouraged them to introduce solid foods prior to the child’s 6-month birthday. Perceptions of children as too thin was a reason for early solid food introduction. A mother of an infant girl explained, “When she [participant’s mother] was a neighbor with us, already she would make her [participant’s daughter] an oatmeal—something to eat with milk.” A mother of three described a similar scenario: Many times it is the traditions you bring as a family . . . they [participant’s mother and mother-in-law] would tell me, “Feed them!” At two months they already wanted to give them [infant children] cereal or banana or something solid. But they weren’t really thin.
It was generally accepted that early introduction of solid food was a common practice among older generations. For example, a participant whose mother began to feed her infant son solid food around 4 to 5 months, said, “My mom’s more traditional; so she would give him rice and beans. Smash it, and give him rice, beans, and squash because they’re soft.”
Sugar as soothing
Another practice discussed across the focus groups was feeding infants sweetened beverages, such as sweetened tea or sugary milk. Some mothers and mothers-in-law, for instance, encouraged the women to give their infant sweetened hot beverages so they would fall asleep. A participant recalled a common scenario in her family: “My mom says, ‘Give them a glass of warm milk with sugar,’ which is a glass of milk that you put sugar in. You sweeten it, so they will drink it.” Another participant described a similar interaction in which both her mother and mother-in-law would say to her, “Give her [infant child] tea.” Family members also encouraged mothers to give their infants sweetened pureed food. A participant explained, My mother would tell me, “Cook rice, boil it. Give the rice water in a bottle to the baby.” Because it has all the vitamins from the rice. If my child didn’t like rice cereal, we would make her papilla (pureed vegetables) . . . My mom would say, “Put a little bit of honey in it so that she feels the taste because it doesn’t taste like anything.”
Mothers’ infant feeding practices and child health outcomes
As the above information highlights, beliefs about infant body ideals (e.g., chubby babies as healthy) influenced infant feeding practices and contributed to early solid food introduction and feeding of sugary drinks and foods. Although mothers in our study were knowledgeable about nutrition, they were unable to consistently apply this knowledge to infant feeding due to the influence of other caregivers. We found that values within Latino families shaped the application of nutrition education to infant feeding practices.
Most participants lived in homes with extended families characterized by a diversity of beliefs about feeding (as described above). The importance of family in Latino culture (familismo) and the high value placed on treating elders with respect (respeto), personal relationships (personalismo), and agreeableness (simpatía) leads mothers to place high value on maintaining harmonious social relationships within the home. The women identified various strategies for navigating the diversity of information on feeding practices (scientific guidelines and advice from trusted others) to preserve social relations. Sometimes mothers adopted practices, or pretended to adopt practices, recommended by their mothers, grandmothers, or other family elders even when they conflicted with recommended guidelines. Other times they educated these trusted others about the scientific feeding guidelines.
Some mothers simply deferred to the elders when they received feeding advice. One mother said, “And the seniority thing. You are kind of like, ‘Okay.’” Preserving positive rapport with family was important. For others, this meant they deferred to their mother’s or mothers-in-law’s advice during face-to-face communication but later enacted a feeding practice consistent with their own perspective. A mother of an infant illustrated this strategy well: “My other aunt says, ‘Give him some peppermint tea [te de herbabuenas].’ But I said to her, ‘Peppermint tea?’ I didn’t give him any. But I said to her, ‘Yeah. I’ll give it to him.’” Another mother used the same strategy: My mother always says, “This baby’s mouth is dry. Give her water.” I say to her, “No, mom!” And she says to me, “Why not? Mix some water with the milk.” So, I tell her, Ok.’ But, I don’t give her water.
Another strategy was to educate the family elders. A participant whose mother and mother-in-law told her to feed her infant daughter sugary tea protected her children’s health by not allowing them to feed her infant sugary beverages. She said, “It is difficult at times to tell the family, ‘No.’ But we are thinking of the well-being of our children. Because our [family] roots are very strong. But families have to learn new ways too.”
Discussion
By drawing on the FEM, we brought forth the macro-level, organization, and community-level factors that intersect the family social and emotional context to shape infant feeding, growth, and early childhood obesity risk. In our study, we found that low-income Latinas’ feeding practices were influenced by several social and cultural factors embedded within family systems, including the mother’s knowledge of recommended scientific feeding practices and the advice and beliefs of trusted other caregivers. Feeding practices also held meaning for mothers. Echoing other scholars’ findings, mothers in our study showed love through food and feeding their infants, who were perceived to reciprocate love by eating their mother’s food (Cheney, 2013; Counihan, 2004, 2009) Furthermore, feeding was a social activity and not the sole responsibility of the mother. Other family members, most commonly the women’s own mothers and mothers-in-law, were very involved in feeding children.
In Western societies, nutrition programs and research tend to focus on the mother–child dyad and overlook the role of other family members, especially senior women or grandmothers in the household. In her review of the literature across 60 cultural contexts and 35 different countries in Africa, Asia, and Latin American, Aubel (2012) found senior women or grandmothers often assumed roles as advisers to young mothers and caregivers of infants and imparted their knowledge on maternal and child nutrition practices throughout the family and community. We found this to be the case in our research. Mothers and mothers-in-law (the grandmothers) were involved in infant feeding and their advice was well respected because of their experiential knowledge, wisdom, and the value of respect for authority within Latino culture. Our work and others demonstrate the need for nutrition programs to expand beyond the mother–child dyad and include grandmothers and other senior women in nutrition education and childhood obesity prevention.
In addition, our findings further substantiate Matvienko-Sikar et al.’s (2018) qualitative evidence synthesis of infant feeding across 25 studies in which they identified guidelines and advice from multiple and overlapping sources (family/friends, health care professionals, official recommendations, the Internet) as a common theme shaping parents’ infant feeding knowledge and practices in diverse cultural and social contexts. In our study, we found that mothers are situated in a context in which there are diverse ideas about feeding, such that mothers have to navigate information about feeding from multiple sources. Many of these mothers lived in extended, intergenerational families where immediate and extended family members born outside the United States (e.g., in Mexico) helped care for the children.
These elders had not received the nutrition education that the mothers had received and often recommended feeding practices inconsistent with scientific guidelines such as early solid food introduction and feeding sweetened beverages. These infant feeding practices are common among Mexican mothers (Gonzalez-Cossio, Rivera-Dommarco, Moreno-Macias, Monterrubio, & Sepulveda, 2006). This may reflect, as others found, limited cooking skills to prepare more healthy foods as well as limited access to healthy options among low-income Latino families (Clark, Bunk, & Johnson, 2010).
Mothers who were cognizant of recommended guidelines had to develop feeding management strategies. Some mothers were more successful than others at implementing scientifically recommended practices in the face of conflicting advice from trusted others. The nutrition education that the women received did not appear to have taught them how to manage the diversity of feeding information they were likely to encounter in the home while successfully putting into practice recommended feeding practices.
Our findings also reinforce previous studies showing that infant body size concerns influence feeding practices in Latino families. Several studies note the contribution of family beliefs that thin babies are unhealthy and chubby babies are healthy to nonrecommended feeding practices (Bunik et al., 2006; Higgins, 2000). In our study, elder caregivers’ concerns that infants were too thin resulted in early solid food introduction, overfeeding, and feeding sweetened puree, all of which contradict recommended guidelines. However, even though the trusted others held beliefs supporting these practices, the mothers themselves rarely viewed their infants as unhealthily thin. This finding suggests the existence of generational differences in infant body size ideals and the meaning of infant growth, wherein younger generations may not view thinner or nonchubby babies as unhealthy.
This research offers rich insight into the sociocultural context of infant feeding among low-income Latinas; however, several limitations should be considered when interpreting the findings. We used a convenience sample and recruited low-income Latina mothers enrolled in a government-sponsored program providing nutrition education. Their experiences may not reflect those of women not enrolled in a similar program. In addition, most women in the study raised their children in intergenerational families; their experiences may not reflect those of Latinas living in nuclear family households. We also did not include the women’s mothers or other caregivers in the research, which limits understanding of generational differences in feeding practices and their meanings, as well as beliefs around chubby babies as healthy. Future research should be conducted with more diverse samples.
We also found evidence of humoral belief systems in women’s discussions about hot–cold food classifications (Barker, Guerra, Gonzalez-Vargas, & Hoeft, 2017). Prior ethnographic work among Puerto Ricans in New York City in the 1970s showed that hot–cold categories of food informed mother’s decisions to feed their infants hot tea and mannitol (a sugary substance) to facilitate feeding transitions from hot to cold foods (Harwood, 1971). Foods classified as hot within hot–cold theories of disease and illness, a health belief model common among Latinos in the United States and Latin America, are thought to strengthen the body and prevent illness (Baer, Weller, de Alba Garcia, & Rocha, 2008). In our work, hot–cold explanatory models of disease may have influenced infant feeding practices including the feeding of sweetened tea, sugary milk, and introduction of sweetened puree—all of which were used to make children fuller or satisfy what caregivers perceived as infant desires to consume food other than milk. Additional research is needed to explore the meaning of hot–cold foods and their relation to sugar, teas, and solid foods.
Implications
Our findings can guide the development or modification of culturally grounded interventions by identifying modifiable, unhealthy practices and unrecognized strengths that could be promoted in interventions. There are only a handful of interventions intended to reduce obesity risk among children below the age of 2 years, all of which focus on the nutritional and dietary aspects of feeding (Arikpo et al., 2018; Ciampa et al., 2010). Our findings show that feeding is a social activity, involving more than mother and child, in Latino families. However, early childhood nutrition or obesity-related interventions target mothers or parents and rarely include other caregivers (Sanders et al., 2014). Consequently, such interventions are not well-tailored to the needs of parents in multigenerational households, such as the predominantly Mexican-origin families of the women in our study, where many family members partake in childrearing.
Latinos of Mexican origin have voiced the need for inclusion of other family members in childhood obesity interventions and to draw on the cultural strengths of Latino families (Kaiser et al., 2015). Because Latina mothers are not typically a child’s sole caregiver, we suggest that trusted others who also participate in feeding the child be included in intervention efforts. Familismo, specifically the value placed on devotion and loyalty to the family, and women’s role as nurturers of the family should also be considered strengths and incorporated into future intervention efforts.
As we found in our study, Latina mothers may experience pressure from family, especially their own mothers and mothers-in-law, to use nonrecommended feeding practices. The women in our study used several strategies to navigate multiple sources of feeding information in culturally appropriate ways to maintain harmonious relationships. These strategies included the following: (a) deferring to respected family members’ advice during interpersonal interactions but enacting the feeding practice they felt best for their child, (b) becoming a voice for children and advocating for them, and (c) educating family members on healthy feeding practices. Communication strategies that attend to Latino values of familismo, respeto, simpatia, and personalismo are needed to help women navigate feeding advice and practices that may put their child at risk for early childhood obesity. Effective communication strategies should align with core Latino values including the desire to maintain harmonious social relationships and be included in obesity prevention interventions for Latino families.
The findings have implications for public health nurses in the United States, as well as nurses in a global context. Nutrition education programs were developed in the 1940s, at a time when its participants were primarily Euro-American (United States Department of Agriculture, 2016). EHS nutrition education, like most nutrition education, prioritizes nuclear family dynamics and identifies parents as primary caregivers (e.g., Perrin et al., 2014). Program material tends to focus on parent–child interactions (e.g., How can I give my child . . .?), which may not resonate with the experiences of parents in households where other caregivers are involved in feeding. This is certainly the case for the EHS population. Over time, this population has become more ethnically diverse and now includes a significant number of children of immigrant parents, including children of Latino immigrants (Golden, n.d.).
To improve the health and well-being of the EHS population, public health nurses need to consider the demographic changes of the EHS population, the involvement of extended family members and other caregivers in child health and well-being, and linked cultural values. As our work illustrates, Latino families may have single or multiple generations and one or more cultures in the home. Latina mothers in our study lived in multigenerational households with family (e.g., mothers or mothers-in-law) who had immigrated to the United States. Within these family contexts, mothers valued the involvement of multiple caregivers in child feeding and were considerate of differences in infant feeding and perceptions of child health. Despite the involvement of multiple caregivers in infant feeding, only mothers receive the program’s nutrition education. As we found, nutrition education, by continuing to focus on single caregivers, does not address the diversity of families in government programs such as EHS (Broyles, Brennan, Burke, Kozo, & Taras, 2011; Passel & Cohn, 2008).
The findings also have implications for international nursing. Across the globe, public health nurses are involved in the education of diverse families, including immigrant parents, on nutrition and feeding practices. However, nurses may not be prepared or aware of cultural differences in infant feeding attitudes and practices, or of the value assigned to specific feeding practices. For instance, in their study on counseling immigrant parents on child feeding in Oslo, Norway, Holmberg Fagerlung, Petterson, Terragni, and Glavin (2016) found public health nurses rarely considered family dynamics and food culture in their counseling approach. In such instances, nurses may draw from their understanding of the food meanings and feeding practices of the dominant culture (e.g., Magnusson, Kjellgren, & Winkvist, 2012), which could create communication barriers and potentially reduce the impact of nutrition education and obesity prevention on child health outcomes.
Conclusion
Latina mothers in this sample were knowledgeable about recommended feeding practices that align with the United States Department of Agriculture’s healthy eating practice campaign (see https://www.choosemyplate.gov/), the cornerstone of government-sponsored nutrition programs for low-income mothers and children (see https://wicworks.fns.usda.gov/nutrition-education). However, they were not always able to successfully put this knowledge into practice in their family contexts. By understanding the sociocultural factors, including knowledge, beliefs, and food meanings that shape Latina mother’s feeding practices, we can develop a shared framework and language for Latina women and nutrition educators to effectively communicate. Such an approach would ideally improve mothers’ knowledge and skills and engage others involved in infant feeding so families can more successfully follow recommended infant feeding practices and work toward optimizing their child’s nutrition and health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by a University of California UC MEXUS Faculty Small Grant.
{kind=link}