
Abstract
As hospitals around the world increasingly face pressure to improve efficiency, “Lean” process improvement has become a popular approach to improving patient flow. In this article, we examine nurses’ perspectives on the implementation of Lean redesigns to the inpatient discharge process. We found that nurses experienced competing demands and tensions related to their time and professional roles and responsibilities as a result of Lean. Four main themes included (a) addressing the needs of individual patients, while still maintaining overall patient flow; (b) meeting discharge efficiency targets while also achieving high patient satisfaction scores; (c) “wasting time” to save time; and (d) the “real” work of providing clinical care versus the “Lean” work of process improvement. Our findings highlight the importance of soliciting hospital nurses’ perspectives when implementing Lean process improvements to improve efficiency and patient flow.
Keywords
Background
Hospitals around the world are facing increasing pressure to improve the quality and efficiency of health care delivery. “Lean thinking,” a quality improvement philosophy and method that originated from the Toyota Production System, is intended to maximize value to customers through elimination of unnecessary steps and wasted time in the manufacturing process (Liker, 2004; Womack & Jones, 1996). The adaptation of Lean methods in health care is an increasingly popular strategy for addressing concerns over the efficiency of patient flow (i.e., movement) through care settings (Beck & Gosik, 2015; Beck, Okerblom, Kumar, Bandyopadhyay, & Scalzi, 2016; Ben-Tovim et al., 2007; D’Andreamatteo, Ianni, Lega, & Sargiacomo, 2015; Graban, 2011; Gray, Harrison, & Hung, 2016; Mazzocato, Savage, Brommels, Aronsson, & Thor, 2010). Improving patient flow is critical if services are to meet the clinical needs of patients.
Some studies on the effects of Lean methods to improve the internal efficiency of Emergency Departments (ED) have shown positive outcomes (Dickson et al., 2008; Holden, 2011; Mazzocato et al., 2012). Most research in this area includes efficiency metrics such as increased patient “throughput” (Holden, 2011) and alleviating “exit block,” which occurs when patients in the ED have been admitted to the hospital but cannot move due to lack of available inpatient beds (Henderson & Boyle, 2014; Pines et al., 2011). Fewer studies, however, have addressed the use of Lean methods as a “system-wide approach” to affect patient flow through the hospital (D’Andreamatteo et al., 2015). Lean thinking and process improvement methods are increasingly being implemented to improve patient flow of the inpatient discharge process (Beck et al., 2016; Henderson & Boyle, 2014; McDermott & Venditti, 2015).
In an integrative literature review of 47 studies in health care, the benefit of Lean principles in improving patient care was clear along with associated challenges and barriers in the implementation process (Magalhães, Erdmann, da Silva, & dos Santos, 2016). However, others have raised concerns about the negative effects of Lean on nursing practice (Saskatchewan Union of Nurses, 2014). Research has identified numerous challenges of adapting process improvement methods designed for industrial manufacturing into the health care sector. These include contextual differences (Harrison et al., 2016; Hung, Gray, Martinez, Schmittdiel, & Harrison, 2017; McDermott & Venditti, 2015; Radnor, Holweg, & Waring, 2012; Young & McClean, 2008) and implications for the social organization of health care (Stanton et al., 2014; Waring & Bishop, 2010). Although there is a growing body of literature focused on the implications of Lean on physicians (Gray, Martinez, & Hung, 2014; Hung, Gray, Martinez, Harrison, & Schmittdiel, 2015; Waring & Bishop, 2010), the sociocultural impact, particularly on nursing practice, is less understood (Joosten, Bongers, & Janssen, 2009; Gough et al., 2014; Rees & Gauld, 2017; White & Waldron, 2014).
There is limited understanding about the impact of Lean-related improvements on nursing. Acute care nurses are on the frontlines of patient care and are critical to successful implementation of quality and process improvement initiatives (Institute of Medicine, 2011; White & Waldron, 2014). The impacts of Lean efficiency initiatives on inpatient nursing, therefore, merit close attention given the growing popularity of Lean thinking in health care. Inpatient nurses play an important role in the discharge process (Foust, 2007; Kripalani, Jackson, Schnipper, & Coleman, 2007); however, little is known about how improving patient flow through Lean methods is perceived by nurses (Connolly et al., 2009; Sanchez-Rubiera, Soto, Cunill-DeSautu, Mestre, & Rodriguez, 2011).
This qualitative research study examines nurses’ perceptions of a Lean process improvement project focused on the inpatient discharge process.
Method
Qualitative Approach
We conducted a focused ethnography study (Roper & Shapira, 2000) to explore nurses’ perspectives on the impact of Lean process improvements in a 241-bed, privately owned, community hospital in Northern California, United States. Ethnographic methods, including participant observation, formal and informal interviewing, are well suited “to describe various perspectives of the participants within an interactive social context” (Roper & Shapira, 2000, p. 12). Our study team consisted of a medical anthropologist, a nurse researcher, a sociologist, a research assistant, and a research scientist with a background in health services research.
Setting
The study site was a 241-bed, privately owned, community hospital in Northern California in the United States. In 2013, in response to increased patient volume, increased ED wait times, and a corresponding decrease in patient satisfaction scores, hospital leadership hired consultants to lead a “Lean transformation” of the ED, followed by redesigns to inter-unit handoffs and inpatient discharge processes. An interdisciplinary “Lean Team” consisting of more than 30 individuals (nurses, nurse managers, nursing administrators, physicians, and representatives from physical and occupational therapy, pharmacy, and radiology) was formed to participate in a week-long “rapid improvement event” (RIE). Using Lean methods such as value stream mapping, the group redesigned the inpatient discharge process and continued process improvement activities during monthly follow-up meetings for 20 months.
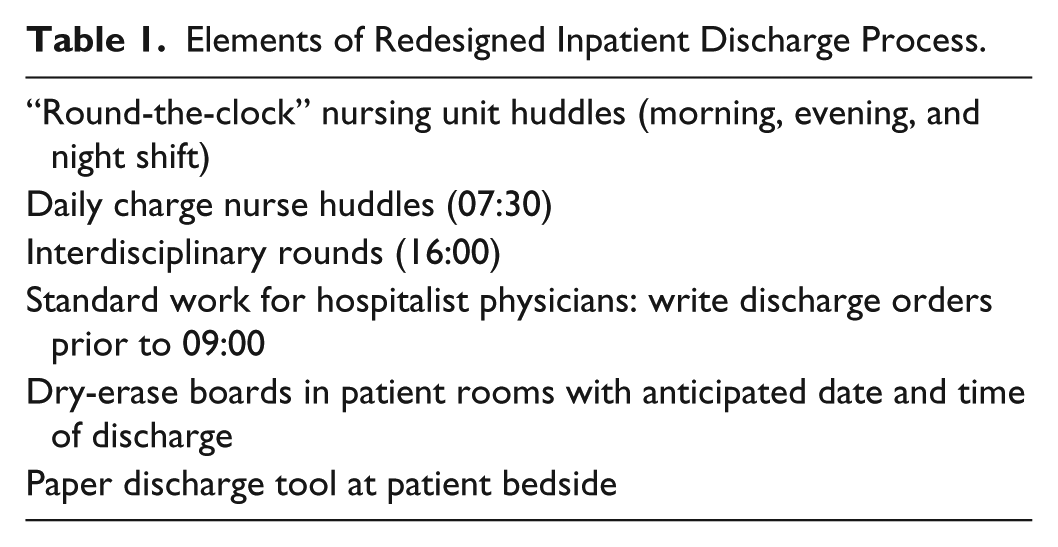
As part of the redesigned discharge process (see Table 1), the Lean Team created a prototype for an interdisciplinary discharge checklist to be incorporated within the electronic health record and interactive in real time. However, unforeseen barriers prevented implementation of the electronic template, and a paper alternative was used.
Elements of Redesigned Inpatient Discharge Process.
Study Sample
Nurses were purposively sampled to include a diverse set of experiences with Lean. We recruited nurses from two groups: (a) members of the Lean Team who participated directly in RIEs, and (b) nurses who were not part of the Lean Team but whose work processes were impacted by Lean. We also designed purposive sampling to include nurses across day, evening, and night shifts from each unit that implemented Lean-related changes to patient flow (medical-surgical [n = 5], intensive care, post-acute care, and ED).
Following ethical approval from the Palo Alto Medical Foundation Institutional Review Board (protocol #2015.051EXP) and hospital leadership, we recruited nurses in person at Lean Team events and via flyers posted on nursing units. Lean Team nurses were allowed to participate in individual interviews during work hours as part of their process improvement duties. Group interviews for non-Lean Team nurses were organized by unit and scheduled outside of work hours. Group interviews with non-Lean Team members were conducted to elicit shared opinions and generate insights about nurses’ perspectives on Lean’s impact on their unit (Stewart, Shamdasani, & Rook, 2007). Participation was voluntary and the anonymity of study participants’ identities was maintained.
Data Collection
We conducted participant observation during RIEs and biweekly follow-up Lean Team process improvement meetings between October 2013 to January 2014. Meetings generally took place in the hospital’s auditorium or conference center with a median length of 2.5 hours (range 1–8 hours). Observations were conducted by Francesca Nicosia, who was introduced to hospital staff as a researcher conducting a qualitative evaluation of the implementation of Lean. F.N. sat in close proximity to the team and recorded the meetings via detailed handwritten notes, which were then transferred into a Microsoft Word document. Because multiple observations occurred over time, it is unlikely the presence of an observer influenced the team’s actions in a substantial way.
After 1 month of observations, we developed the interview guide based on themes identified in observation notes, study aims, and constructs from the Consolidated Framework for Implementation Research, modified for studying Process Redesigns (CFIR-PR; Rojas Smith, Ashok, Dy, Wines, & Teixeira-Poit, 2014; Table 2). CFIR-PR is an implementation science framework intended to account for contextual factors impacting efficiency interventions. We included constructs related to implementation process, measures, and outcomes, including perceived value and unintended consequences. We designed interview guides to elicit the perspective of both Lean “champions” who were involved in RIEs and those who did not actively participate in those events.
Sample Interview Questions.

We conducted individual and group interviews (2–6 participants) between January 2014 and December 2015. Individual interviews were conducted by F.N. with assistance from a second researcher for group interviews. Interviews were continued until thematic saturation was reached. Participants provided written informed consent, and interviews were audio-recorded and transcribed verbatim by a third party. Ongoing consents were not needed. Individual interview participants chose a convenient time and location for the interview. Group interviews were conducted either before or after shifts in the hospital’s conference center away from clinical areas. Refreshments were offered to all participants, and nurses were offered the equivalent of their hourly rate as a monetary incentive. No coercive practices were employed. Two participants declined to audio-record their interviews, in which case we took detailed handwritten notes. During this time, we continued observations of Lean Team meetings (76 hours) and implementation-related activities on nursing units including daily huddles, charge nurse rounds, nurse manager huddles, and auditing activities (27 hours) to provide context and refine interview guides as needed.
Data Analysis
Analysis began at the beginning of the data collection process and continued concurrently and iteratively throughout the study period to inform thematic development. We analyzed field notes and interview transcripts using inductive thematic analysis (Bernard, 2011) and refined through multiple close readings. Rigor was maintained through parallel independent coding to ensure credibility, dependability, and reliability of findings (Thomas, 2006). The lead author (F.N.) first developed analytic themes, and then provided two additional researchers (C.G., M.Y.) with a random sample of 25% of transcripts for independent coding and confirmation of initial themes. The remaining interview transcripts were each analyzed by two coders, using constant comparison throughout the study period, returning to previously coded field notes and transcripts to ensure consistency (Dye, Schatz, Rosenberg, & Coleman, 2000). We used Atlas.ti (Version 7.0.83), a computer-assisted qualitative data analysis software program, to manage observational and interview transcript data and establish an audit trail, which was regularly reviewed by the senior author. We met regularly to discuss findings, reconcile discrepancies, discuss alternative perspectives, and reach consensus on the final coding scheme and analysis.
Results
Nine nurses participated in a one-time individual interview and 15 in group interviews (n = 26). Seven participants were members of the Lean Team (25%); 19 were nonmembers of the Lean Team and had not participated in RIEs (75%; Table 3).
Participant Characteristics.

Group interview.
Individual interview.
Four themes emerged from nurses’ perspectives on Lean process improvements to patient flow and discharge process efficiency: (a) addressing the needs of individual patients, while still maintaining overall patient flow; (b) meeting discharge efficiency targets while also achieving high patient satisfaction scores; (c) “wasting time” to save time; and (d) the “real” work of providing clinical care versus the “Lean” work of process improvement (see Table 4). These themes point to nurses’ perceived tensions between their roles and responsibilities for patient care and as hospital employees.
Themes and Illustrative Quotes.

Note. ED = Emergency Department; RIE = rapid improvement event.
Addressing Individual Patients’ Needs While Maintaining Overall Patient Flow
Interviews revealed that nurses involved in direct patient care experienced tension between attending to individual patients’ needs and increasing patient flow throughout the hospital. They saw the latter as the Lean-based goal to improve organizational efficiency. One nurse explained, You have a patient ready to go home, and then you have a patient who needs your full attention, so where do you go? You feel the pressure because you know that they [the hospital] expect you to discharge the patient before noon. (Nurse, Medical/Surgical Unit)
During process improvement activities, we observed that nurses were often told that Lean would help to “prioritize patient care.” However, the above quote shows that nurses’ responsibility to individual patients at times conflicted with changes to discharge process workflows and maintaining patient flow efficiency through earlier discharge times.
Nurses were also asked their impressions of why the Lean redesign of the discharge process was implemented: One might say that it improves the patient’s experience. One might also say that it is a better utilization of resources to prevent backlogging of patients’ movement through the [hospital]. So you could say both of those things [emphasis in original]. (Nurse, Intensive Care Unit)
This comment reveals how nurses’ perception of Lean did not align with the stated goal of improving the patient experience. Many nurses expressed a negative perception of the rationale to implement Lean to improve patient flow. Representing this view, one nurse simply stated, “It all goes down to money.” Both members of the Lean Team and bedside nurses who did not participate directly in the RIEs considered the redesigned discharge process an impersonal initiative intended to increase efficiency that forced them to “push patients out” to keep beds occupied and improve the hospital’s “bottom line.” A common refrain heard during interviews and observations was, “Lean is mean.” We frequently overheard nurses saying this, particularly when the redesigned discharge process required them to prepare patients for discharge who did not feel ready to leave the hospital. This recurring theme highlighted the tension between dual rationales to increase efficiency—improving both the patient experience and the hospital’s financial performance through increased throughput and resource utilization.
While nurses from both the Lean Team and nonmembers of the Lean Team were critical that earlier target discharge times were forcing patients out prematurely, others explained to us the benefits to patients of being released earlier, such as reduced infection risk, better sleep, and recovering more quickly at home. Some nurses explained how their awareness of research related to earlier discharge times informed their attitudes to Lean redesigns to the discharge process, helping reconcile the tension between prioritizing individual patients’ needs and overall patient flow. However, because of personal experience with individual patients, awareness of evidence demonstrating improved outcomes as a result of earlier discharge did not strongly influence nurses in their acceptance of the redesigned discharge process.
Meeting Discharge Efficiency Targets While Also Achieving High Patient Satisfaction Scores
The imperative of the redesigned process to discharge patients early in the day and open up beds for admitted ED patients created tensions for nurses around meeting the discharge metrics and providing a positive, caring experience to their patients. Nurses consistently reflected on how the redesigned discharge process and push to meet target discharge times impacted their relationships with patients. Nurses frequently expressed concern about their older patients, particularly those who lived alone and expressed anxiety around early discharge times. One nurse summarized the perception that patients felt rushed: The elderly, those are the ones who don’t have a ride mostly, are saying they are being pushed out. (Nurse, Medical/Surgical Unit)
Nurses explained how many older patients do not have family nearby and would worry about who would prepare a meal for them after leaving the hospital. To alleviate this concern, we observed some nurses intentionally delaying the time of discharge so that patients could remain in their room and have lunch prior to leaving the hospital, thus, leaving on a “high note.”
Nurses consistently reflected on how the push to meet target discharge times impacted patient satisfaction: Satisfaction scores are lowered when we’re rushing the patient to get out of here. A lot of [patients] think they should have stayed one more day. We explain to them that they’ll be better off if they recover at home, no interruption in sleep, infection exposure. But still, it feels like they are being pushed out. (Nurse, Medical/Surgical Unit)
This quote further illustrates the tensions nurses faced between meeting target discharge times and ensuring patients had a positive experience that would translate into high patient satisfaction scores, which nurses were concerned would be impacted if patients felt they were discharged too early.
Wasting Time to Save Time
Nurses were asked to describe their experience with the bedside discharge checklist and how they incorporated it into their daily workflow. Nurses were initially excited about implementing an electronic, interdisciplinary checklist. However, nearly all nurses and non-Lean Team Unit Managers expressed frustration that the form created redundancies and additional work: “It’s created extra work having to document things in the medical record and again on this paper. I feel like I’m just wasting time to save time” (Nurse, Medical/Surgical Unit).
Keeping the paper form at the patient bedside was an additional source of frustration for nurses. The form’s location was a barrier for interdisciplinary care team members to actively utilize and update the tool, resulting in nurses disproportionately feeling the burden of extra work.
On the original paper [form], there used to be a part for the physician and the case manager. None of them wanted to do it because they know it’s another waste of their time, so they pass it on to the nurses. (Nurse, Medical/Surgical Unit, Lean Team member)
This quote reflects the opinion of the majority of bedside and charge nurses we spoke with who pointed out that the form was not utilized by all members of the interdisciplinary team, as was originally intended.
“Real” Work of Providing Clinical Care Versus the “Lean” Work of Process Improvement
Nurses’ perception of changes to the discharge process was that the amount of work, namely, the requirements of additional documentation by staff nurses and auditing by Lean Team members, took away time from direct patient care. Nurses distinguished between “real” work of direct patient care and “other” Lean work focused on process improvement activities. One bedside nurse from a medical unit stated, “All this Lean stuff has wasted my time, actually. We’re too focused with the [paper discharge checklist] that it takes away patient care.”
For nurses who participated in RIEs and ongoing Lean Team follow-up meetings, the desire to participate in quality improvement initiatives was often overshadowed by the extra time commitment on top of clinical shifts. One nurse explained the tension between clinical and process improvement work as follows: We need a nursing lead or a team of people who have more dedicated time to do this because we have a lot of good people who were on that group [Lean Team], but they were excused from their regular job to sit in that room [for the RIEs] for that amount of time. And, afterwards, we’re not given extra work time to be really responsible for all of this. None of our other duties went away. (Charge Nurse, Medical/Surgical Unit)
Discussion
Our findings illustrate several of the effects of implementing Lean methods to increase efficiency in the inpatient discharge process. The tensions nurses experienced as a result of Lean redesigns to the discharge process stemmed from a perceived conflict between patients’ individual needs and the need for patient “flow.” This finding adds to our knowledge on the impact of increasing patient throughput on nurses. Connolly et al. (2009) found that nurses reported facing conflicting pressures around keeping patients in the hospital rather than “pushing” them out. This tension in our study was most apparent in nurses’ experiences caring for older patients whose family members were unable to provide transportation home early in the day or for those who had anxiety around returning home alone. This finding further highlights how nurses’ identities as professionals and their duty to advocate for patients may conflict with their responsibilities as employees of a larger organization.
Evidence suggests that efforts to restructure health care delivery using managerial models, particularly those focused on improving efficiency, have had an adverse effect on nursing professionalism by devaluing and deskilling nursing work (Brannon, 1994; Melon, White, & Rankin, 2013; Newman & Lawler, 2009; Rudge, 2015; Urban, 2014; Zeytinoglu et al., 2007). In particular, research on efforts to improve efficiency through scripting and standardization of nurses’ speech in the United States have shown adverse effects on nurses’ professional autonomy, including deskilling and the inability to exercise clinical judgment, a requirement of registered nursing (Pine, 2011). Many nurses in this study expressed how the expectations to meet efficiency metrics overshadowed their ability to exercise judgment in caring for their patients.
Efforts to restructure health care around efficiency, such as New Public Management in the United Kingdom and elsewhere, have resulted in a decline in work satisfaction, motivation, and commitment of nurses in an atmosphere of work intensification (Rees & Gauld, 2017; Selberg, 2013; Stanton et al., 2014; Zeytinoglu et al., 2007). Research on the effects of the Productive Ward initiative in the United Kingdom, which was intended to “release time to care,” has shown mixed results in terms of work engagement, nurses’ sense of professionalism, and ethical responsibility to their patients versus their responsibility to the organization (Gough et al., 2014; White, Wells, & Butterworth, 2014). Our study adds to this literature in the context of Lean process improvements, highlighting the demands placed on nursing labor to meet efficiency targets, often at the expense of providing patient-centered care. As hospitals come under increasing financial and regulatory pressure to deliver more efficient care, it is imperative to do so without contributing to intensified workloads that lead to job dissatisfaction, burnout, and high staff turnover (Stanton et al., 2014). Recognizing that nurses’ professional expectations and their commitment to patient-centered care may conflict with attempts to improve efficiency and productivity will go a long way toward making these efforts more effective and sustainable. However, Mikesell and Bromley (2012) found that some versions of patient-centered care might “obscure substantial and substantive nursing work” and undermine nurses’ professional roles.
This study suggests the distance between the theoretical principles behind Lean process improvement—improving value through reducing waste—and its practical application in health care settings. While the underlying goals of Lean are to eliminate waste and create value for the “customer/patient,” these are often difficult to achieve in real-world settings. “Wasted time” alone is not an accurate measure of inefficiencies, as patient-centered care processes that are valuable to patients most often require time spent at the bedside. When hospitals must contend with both patient satisfaction metrics as well as financial and regulatory pressures to improve efficiency, the secondary focus of improving patient experience is often subsumed under the organizational logics of efficiency and productivity.
The time-intensive nature of Lean process improvement work is a common critique of the adaptation of Lean to health care (Aij, Simons, Widdershoven, & Visse, 2013; Carmen et al., 2014; Hung et al., 2017). In this study, we found that in addition to the increased time burden required to carry out continual process improvement activities, subsequent workflow redesigns of the discharge process created tensions between nurses’ responsibilities toward their “real” work and “Lean” work. To increase the success and sustainability of Lean initiatives, organizations should invest adequate resources such as increased staffing or allowances for overtime to engage in process improvement activities. When these resources are inadequate, nurses’ time and attention are pulled in multiple directions, ultimately undermining the success of quality and process improvement efforts.
The promise of Lean to improve staff engagement has been identified as a challenge in both operations and research literature (Poksinska, 2010). The Lean pillar of “putting people first,” which involves frontline engagement and prioritizing the expertise of those closest to the work when solving problems and redesigning workflows, was not fully embraced in this study setting. The lack of staff nurses on the Lean Team (Table 2) resulted in redesigned processes that were not informed by the experience and expertise of these nurses. Because staff nurses perform the bulk of direct patient care and their work was most affected by the implementation of the redesigned discharge process and the use of the paper discharge tool, being excluded from the Lean Team prevented those on the frontlines of patient care from contributing their expertise to the Lean redesign and continual improvement processes.
This study suggests, as others have argued, that models of quality improvement derived from manufacturing are unsuitable for health care settings (Pine, 2011). However, if health care organizations continue to implement Lean methods, attention should be paid to better integrating clinical and process improvement work. Similar to recent research, we found that nurses conceptually and practically delineated clinical care work and improvement work as separate, competing priorities (White, Butterworth, & Wells, 2017). Participants in this study made it clear that they experienced aspects of the process redesign as creating additional and redundant work that took away from their time providing direct patient care. Because of the time-intensive nature of process improvement work, attention should also be paid to ensuring that efforts to “improve” processes do not create redundant work or additional administrative burdens for nurses.
The barriers to incorporating the discharge tool within the electronic health record contributed to the disintegration of the interdisciplinary intent of the initial RIE. While physicians, case managers, and physical therapists had flexibility in either using or ignoring the discharge tool, staff nurses, because of their position within the hospital’s hierarchy as well as potential concerns around disciplinary action for noncompliance, were required to follow the changes to the discharge process. When redesigning patient flow processes, it is important to be clear about roles and accountabilities, particularly when multiple departments and disciplines are involved. As the concept of “systems thinking” becomes more widespread in efforts to improve the efficiency of complex processes such as patient flow, careful attention must be paid to the inherent challenges of interprofessional and interdepartmental collaborative efforts. Nurses must experience efforts to improve patient flow as enhancing their role as direct care providers and patient advocates, not intensifying workload. Hospital and nursing leadership must be willing to de-implement changes when they do not work as intended. Moreover, efforts must be made to implement Lean and other quality improvement initiatives in a truly democratic fashion so that all nurses’ experiences and voices are valued.
Scholars have identified a positive publication bias for studies of Lean implementation and outcomes, particularly in the United States (Carmen et al., 2014; D’Andreamatteo et al., 2015; Holden, 2011; Mazzocato et al., 2010). In contrast, this study shows how, in some cases, efforts to improve efficiency and hospital-wide patient flow using Lean methods may adversely impact frontline nursing staff, including the creation of tensions between dual responsibilities to patients and the organization. These tensions are important to address, particularly when trying to understand nurses’ engagement with efforts to improve efficiency and patient flow. Further ethnographic research is needed to explore the effects and unintended consequences of Lean on hospital nursing.
Our study has some limitations largely influenced by the qualitative methodology and sample from one privately owned acute care hospital in Northern California, which may limit the generalizability of our findings. Sample selection may have also contributed to potential bias in our results, as nurses who were more positive about Lean may have chosen not to participate. However, the benefits of thematic analysis lend valuable insights that might be transferable to other settings implementing Lean process improvement. We also experienced known challenges of recruiting acute care nurses such as time and workload constraints, logistical challenges around scheduling, and potentially a lack of interest in the research topic or ambivalence about the value and applicability of the research (Broyles, Rodriguez, Price, Bayliss, & Sevick, 2011). To address these barriers, future research could be approached using Participatory Action Research or similar model.
Conclusion
The engagement of nurses is crucial for the success of hospital quality improvement initiatives. We used the voices of nurses to gain insight into the effects of Lean redesigns to streamline patient flow and improve the inpatient discharge process. This study highlights how a Lean-based process redesign effort implemented in a community hospital in the United States created tensions for frontline staff nurses, placing competing demands on their time and professional roles and responsibilities. As the use of Lean methods to improve throughput and patient flow increases in popularity within hospitals in the United States as it has in other parts of the world, more research is needed to understand nurses’ experience of such efforts. Research and practical applications of Lean should focus on ways to improve efficiency while also balancing nurses’ professional autonomy and commitment to delivering patient-centered care in a way that does not create additional burdens for nurses.
Footnotes
Author’s Note
Maayan J. Yakir is also affiliated with Oakland University William Beaumont School of Medicine, Michigan, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research funding was provided by the Gordon and Betty Moore Foundation.