
Abstract
The purpose of this study was to describe and explain the process by which homeless veterans manage their chronic health problems. In the United States, over 550,000 people experience homelessness on any given night. Of these, over 11% are veterans of the military, many whom suffer from at least one chronic disease. Study participants included male homeless veterans with at least one chronic health problem recruited at a Veterans Affairs emergency department, a homeless shelter, and a soup kitchen. Semi-structured interviews with 32 veterans from the Vietnam/post-Vietnam era were audio-recorded, verified, and coded resulting in a theory entitled “pursuing the mission,” which describes and explains four ways (deferring, exploring, embarking, embracing) they manage their chronic health problems. The findings from this study provide insight from individuals living this experience and will help guide the future delivery of health care to homeless veterans.
In the United States, over half a million people are homeless on any given night (U.S. Department of Housing and Urban Development [HUD], 2015). Homelessness is associated with poorer health status due to the difficulty in maintaining health while attempting to satisfy the basic human needs such as food, shelter, and safety. Homeless individuals suffer from higher rates of communicable and noncommunicable diseases, higher mortality rates, and multiple comorbidities (Schanzer, Dominguez, Shrout, & Caton, 2007). They often overuse emergency services, underuse primary care services, and require longer lengths of stay as inpatients compared with the general population (Kushel, Vittinghoff, & Haas, 2001). Veterans of military service are overrepresented in the homeless population, accounting for 11% (or 48,000) of homeless adults (436,000) (HUD, 2015). Rates of homelessness have remained consistently higher in the veteran population, with male veterans 50% more likely to be homeless than male nonveterans (Fargo et al., 2012). Veterans have an increased risk of compromised health status because of their greater representation among this vulnerable population.
Homeless veterans suffer from higher rates of chronic disease and comorbidities than their nonveteran counterparts (Goldstein, Luther, Jacoby, & Haas, 2008) with over half suffering from at least one chronic health condition (Fargo et al., 2012). Physical and mental disorders experienced by homeless veterans are heterogeneous and do not necessarily fit any defined health framework. Their complex pattern of health contains components of both chronic medical and chronic psychiatric health problems. Common medical problems experienced by homeless veterans include diabetes, hypertension, cancer, chronic obstructive pulmonary disease, and heart disease (Goldstein, Luther, Haas, Appelt, & Gordon, 2010). Common psychiatric problems include depression, bipolar disorder, posttraumatic stress disorder (PTSD), schizophrenia, and substance abuse disorders (Goldstein et al., 2010). Other illnesses such as ulcers, frostbite, and malnutrition can be attributed to the general aspects of homelessness and exposure to the elements. Given the large number of homeless veterans, there is a significant challenge to health-care professionals, and the general public health domain to address the multidimensional and complex health needs of this population.
Barriers to optimal health care among homeless populations are widely documented. Lack of affordable health care (Tsai & Rosenheck, 2014), service fragmentation among health-care institutions and providers, and transportation all create obstacles to care (Blue-Howells, McGuire, & Nakashima, 2008). Other barriers exist for veterans including a complicated health-care eligibility process within the veterans affairs (VA) system. This often causes great difficulty for veterans to navigate (Blue-Howells et al., 2008) and, therefore, seen as a stressor rather than a benefit. In addition, a common misconception is that all health care at the VA is free for veterans but this is not necessarily true. Services may still require copays and be billable depending on a veteran’s eligibility status (i.e., military service) and insurance. Veterans may also be eligible for service-connected health benefits based on injuries that occurred during their active military service (Weber & Clark, 2016). Finally, veteran’s own perceptions of their health can influence their ability to access care. Utilizing health-care services can be perceived as a weakness, which is sharply contrasted with their military way of life in which they are perceived as strong (Gilliss, 2010).
In the United States, the cost burden of chronic disease is 78% of total health spending (Bodenheimer, Chen, & Bennett, 2009). This number is expected to increase over the next 10 years due to the aging population and a rise in modifiable risk factors such as obesity. In addition, there is a stronger correlation seen between those who fall below the federal poverty level and chronic disease compared with the general population (Bodenheimer et al., 2009). All of these factors result in an increased burden and financial strain on the U.S. health-care system. Therefore, it is likely that veterans who are homeless and suffering from chronic disease are at a higher risk of developing more chronic illnesses as they age, thus requiring more health-care services.
In 2009, President Obama, along with the former VA Secretary Eric Shinseki, set a goal of ending chronic and veteran homelessness by focusing on six areas including education and outreach, treatment, prevention, housing and supportive services, employment and benefits, and community partnerships (U.S. Interagency Council on Homelessness, 2010). This comprehensive plan further highlights the need to address national homelessness among the veteran population and make positive contributions to reduce this phenomenon. These combined factors create multiple questions about the lives and experiences of homeless veterans living with chronic diseases and contribute to the foundation for this study. The goal of this grounded theory study was to develop a theory to describe and explain how veterans who are homeless manage their chronic health problems. The research question was as follows:
Method
Grounded theory methods were used to answer the research question in this study (Glaser & Strauss, 1967). Glaser and Strauss successfully merged their philosophical traditions of positivism and pragmatism with influence from Herbert Blumer’s (1969) theoretical concept of symbolic interactionism to develop theory that is “grounded” in the research data and able to explain real-world phenomenon (Glaser & Strauss, 1967). The population of veterans in this study shares the same fundamental problem of being homeless, while also suffering from some chronic disease. This is a “real world” phenomenon as described by Glaser and Strauss (1967) that can be explained by data generated through the grounded theory process. The focus of this inquiry was to determine how homeless veterans resolve the problem of disease management through a social or psychological process. Homeless male veterans with at least one diagnosed chronic health problem were recruited. Men make up 91% of the homeless veteran population whereas females make up 9% (HUD, 2015). Homeless female veterans were excluded from the study because of their low representation and, therefore, low accessibility rate. In addition, female veterans’ experiences managing chronic disease could be substantially different from men because of gender-related factors influencing health-seeking behaviors and sex-specific medical conditions.
Recruitment
Institutional Review Board and VA Research and Development Committee approval was obtained. Detailed study announcements were posted at three locations in one large Midwestern city including a VA medical center emergency department, an emergency shelter, and a soup kitchen. In addition, the principal investigator made visits to the soup kitchen during meal times and to the shelter during bimonthly veteran-specific meetings for face-to-face recruitment. All potential participants were screened for inclusion and exclusion criteria, provided with detailed information about the study, and any questions or concerns were answered. Written informed consent and demographic information were obtained prior to interviews.
Sample
Purposive sampling at the three locations was initially used to recruit homeless male veterans. This sampling method is consistent with grounded theory method and allowed the principal investigator to deliberately select participants who met the inclusion criteria of being a homeless male veteran with at least one chronic disease. Participants were recruited over a 6-month period and ended as saturation occurred and no new information was discovered (Glaser & Strauss, 1967). The systematic collection of data, sampling, and analysis occurred simultaneously and then theoretical sampling was used to collect further information from remaining participants to enrich the developing theory. Using comparative analysis, the initial participant demographics and interviews showed that many recruited veterans were from the Vietnam/post-Vietnam era (1961–1975) and thus their experiences with chronic disease and homelessness were different than veterans from the current war in Iraq and Afghanistan (n = 2). Therefore, the principal investigator and research team determined that the remaining veterans recruited should only be from the Vietnam/post-Vietnam era (n = 32).
Data Collection
All interviews were conducted by the principal investigator and occurred in a private room at each location. The principal investigator is an experienced emergency department nurse who has worked extensively with veterans and the homeless for the past 10 years. Participants were interviewed one time and encouraged to tell their stories and experiences about managing their chronic health problems while also being homeless. The interview began with open-ended questions (“You have indicated that you have had a health problem for a long time without having a stable home. I am interested in understanding how you manage this”) and more specific questions (“Tell me about a specific time when you needed treatment for your chronic health problem”) were asked as the theory began to emerge from the data. This type of interview process follows the strategies of grounded theory development. Interviews averaged 40 minutes in length, were audio-recorded, and field notes were taken during each interview reflecting on the environment, the participant’s behavior, and the context of each interview. Each participant received a US$35 gift card to a large chain grocery store for compensation of their time.
Data Analysis
Interviews were audio-taped, transcribed, and verified by the principal investigator. All data were stored behind the protected VA firewall and were de-identified to ensure privacy and confidentiality. The qualitative software MAXQDA (2015) was used to assist with data analysis. Data were analyzed by the principal investigator, a team of two experts in qualitative research, and one undergraduate honors nursing student who is in the U.S. military. Substantive coding, including line-by-line coding and selective coding, was initially used (Glaser, 1978). Line-by-line coding was completed by the principal investigator and one member of the research team on the first four transcripts. Words, phrases, and sentences were carefully examined and then compared between other transcripts for similarities and differences resulting in the development of 16 initial categories. Selective coding was then used to analyze the remaining transcripts and place all data in the defined categories. During selective coding, the team collapsed codes and expanded codes as the theory began to emerge and a higher level of coding, theoretical coding, was then initiated. Theoretical coding allowed for increased abstraction of the data set resulting in the development of the emerging theory. Comparative analysis was used throughout the process, allowing the principal investigator and the research team to ask multiple questions of the data and thereby determine the trajectory of the data set.
During the processes of coding and comparative analysis, the core concept of “pursuing the mission” was identified by the research team to metaphorically describe homeless veterans’ efforts to manage their chronic health problems. The term “mission” is a widely used military term associated with performing a specific military task or duty and the action to be taken (Department of Defense, 2016). As theoretical coding was being conducted, the concept of pursuing the mission was broadened by the principal investigator and the research team to link identified theoretical constructs from the data regarding care management back to the main core concept. The transcripts were re-examined for evidence of various ways or actions that veterans use to pursue their mission of health-care management resulting in the final modifications of the theory.
Multiple methods were used to enhance rigor of the study findings. Trustworthiness or validity of the study was ensured through the use of a research team. Intersubjective agreement among the team members ensured the credibility of the findings along with the use of direct quotes from participants (Denzin & Lincoln, 2011). Transferability was ensured by providing an adequate description of the sample, and dependability of the data was fulfilled by verification of the audiotapes by the principal investigator against the transcripts. In addition, confirmability was ensured in this grounded theory study by the creation of an “audit trail” including field notes taken during interviews and written memos that described the theoretical decisions and ideas that came from the data (Denzin & Lincoln, 2011).
Results
The final sample included 32 homeless male veterans with at least one diagnosed chronic health problem. All participants who agreed to participate signed the informed consent and were interviewed. Much of the sample was African American (n = 23; 72%) while the remaining participants (n = 9; 28%) identified as Caucasian. Veterans from four military branches made up the sample including the air force (n = 4), army (n = 18), marines (n = 5), and the navy (n = 5). Years of military service varied with a range from 33 days to 20 years (M = 5 years). The number of episodes of homelessness among the participants ranged from one to eight (M = 3 episodes). Most of the participants lived in a shelter or short-term rehabilitation center (n = 28) while the remainder were staying in their car, on the streets, or in abandoned buildings (n = 4). The most common chronic diagnoses found among the sample include chronic pain (n = 17), depression/anxiety (n = 13), hypertension (n = 15), substance abuse (n = 20), and PTSD (n = 11). In addition, 75% (n = 24) of the study participants indicated the use of the VA health-care system and over half the veterans interviewed (n = 19) reported having a primary care provider either within the VA system or the community.
The way homeless veterans manage their chronic health problems depends on the manner in which they approach their health, the resources they have access to, how they choose to utilize those resources, and how they drew on their military experiences for support. Participants described how their time in the military affected their civilian or postmilitary life and particularly how they approached management of their health. Therefore, the core concept of “pursuing the mission” was used to metaphorically describe and explain the four different ways homeless veterans manage their chronic health problems as found in the data (Figure 1). The “mission” is the task or duty and the action that needs to be taken to manage their chronic health problems. Participants address that mission through four different ways or actions, which include deferring the mission, exploring the mission, embarking on the mission, and embracing the mission.
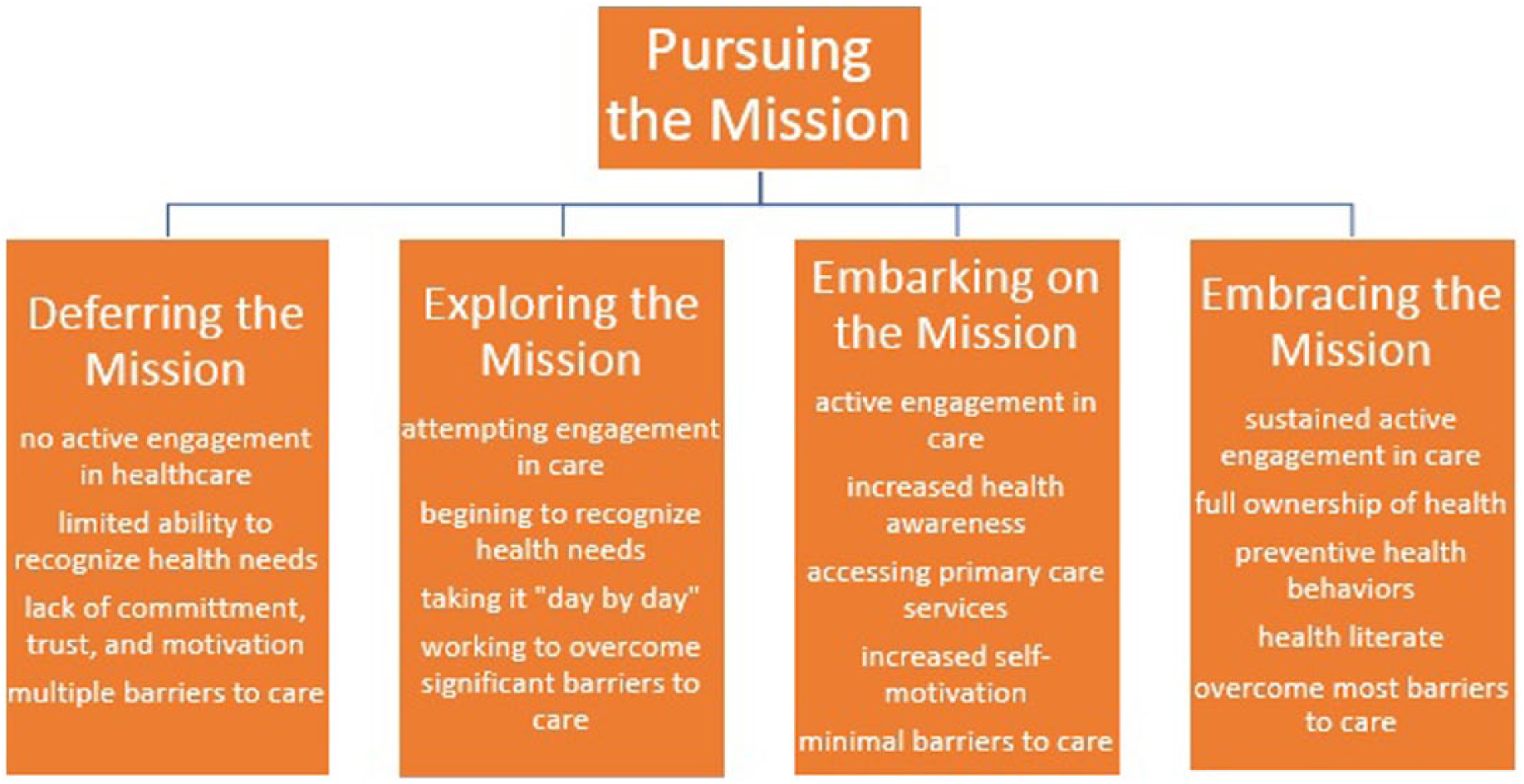
Theory of “pursuing the mission” with defined characteristics.
Participants “deferring” are not managing their chronic health problems. They do not actively engage in health-care services to treat their chronic issues. Therefore, they are deferring their mission or the act of managing their chronic health problems. Participants “exploring” are beginning to explore and learn how to manage their chronic health problems. They have taken the initial steps to seek health-care services and participate in their care. Participants “embarking” are accepting and adjusting to the management of their chronic health problems. They are committed to the process of achieving care management but shifting their actions as needed to fit with their life circumstances and barriers they face. Finally, participants “embracing” are successfully managing their chronic health problems and have embraced the “mission.” They have committed to the process, they are actively engaged in services, and their chronic health problems are successfully being managed with positive health outcomes.
Deferring the Mission
Veterans who were “deferring the mission” (n = 4 participants) are defined as those not managing their chronic health problems. They have not taken the steps to actively engage in the process of obtaining positive health outcomes and often have a limited ability to recognize the need for health services. They also experience multiple barriers that cause deferment of the health mission. These include logistical barriers such as unemployment and lack of transportation, but also personal barriers such as lack of trust in the system, mental health issues, and/or substance abuse. One participant described transportation barriers affecting his ability to access the hospital to get his medications: It’s very difficult, because once I lost my job, it affected me as far as having bus fare to get back and forth, because my feet are bad too and sometimes I would have to walk. . .that really affects me, because I have to walk all the way to get my meds. (Participant A)
Veterans described lack of trust in health-care providers and agencies as a reason they defer management of their health problems. They provided descriptions of being treated negatively at times by staff and health-care professionals because of their life situation. One negative experience can prevent any future attempts at accessing health care. One participant described attempting to go to a health clinic and the manner in which he was treated: It was frustrating. People were unprofessional, disrespectful. They had no idea what they were doing. They were under-trained and underpaid and it showed and I see these type of things, plain as day, but if you somehow show them that you see that, then they get defensive and then you really got a problem. (Participant B)
Another participant described how the general condition of being homeless affects your mental and physical health, increasing the deferment of the mission: You can’t stay as clean as you use to when you’re homeless, you’re stressed out, you don’t know exactly who you can turn to or where you can get your medicine, it’s difficult when you’re homeless, I get depressed sometimes and then I procrastinate, you’re out there, you know and your mind could be on some other stuff, you really would like to take care of the situation right then and there, but it’s hard because you’re trying to get yourself together, get a job and everything, get housing, so it’s more than one thing to think about. It’s not the same as being in a structured environment and when you’re in a structured environment, you got more assets that can help you. (Participant C)
One participant described a continuous cycle of attempting to maintain sobriety and hold down employment but then falling back into addictive behaviors with negative results: I gotta get my medicine and everything first, right now I’m can’t go to work like this, dizzy, lightheaded spells and then it got worse and actually last week it’s gotten worse. . . I do have a bad marijuana addiction because I got stressed out and I turn to drugs. (Participant D)
In addition, there can be a lack of commitment and motivation to managing their health problems, which results in no active engagement in the health-care system, no use of primary care services, or any health services at all. Veterans who are deferring the mission often speak of feeling depressed, hopeless, taken advantage of, and have low self-worth. “Some people took advantage of me because I suffer from mental illness. They took advantage of me and took my money. They tried to swindle me, I lose in the end.” Homeless veterans may defer the management of their chronic health problems for multiple reasons. All participants in this category were unable to begin consistent active engagement in their health care. They described personal and logistical barriers that obstruct their ability to manage their diagnosed chronic diseases and pursue positive health outcomes.
Exploring the Mission
Homeless veterans categorized as “exploring the mission” (n = 12 participants) are defined as those who are just beginning to discover and become aware of their health mission. These participants describe initial attempts at active engagement in the health-care system. Frequently, these individuals are aware of their health problems and try to deal with them as best as they can on a day-to-day basis. They are slowly taking the needed steps to successfully manage their chronic health problems while still facing significant barriers. One participant who recently entered a substance abuse treatment facility for homeless veterans described his initial thoughts about his health progress and his plans for moving forward. “Right now, I’m taking everything day by day. My goal is to end the homelessness, stop my alcoholism and to live a productive life.”
Unfortunately, it can be difficult for these veterans to stay on a healthy track because they are just beginning the mission. Many described experiencing turning points in their life where they knew that they could not keep up with the unhealthy lifestyle they were living. A participant described his feelings of loneliness and desperation and how that helped to turn his life around and served as a motivator to seek treatment for alcohol abuse: The desperation that I was in my last three year run, the feeling of hopeless that I was in, is a feeling that I never want to feel again. I don’t want to feel that no more, you know just a feeling that I felt. This last episode of homelessness was rough. (Participant E)
Participants who were “exploring the mission” also describe becoming more self-aware in regard to their health. They are more aware of the need to take care of their health problems and often attempt to seek care. One participant described realizing the need for management of his health problems and how that influenced his ability to take control of his life: While I was in the streets homeless, I was really concerned with myself, with my health problems. I do have depression, so I would drink to deal with the depression. . . and I did not worry about my health problems, my high blood pressure or anything, I would just not worry about it, whatever happens, happens. Since I’ve been in rehab it has become a concern. I’m not drinking anymore and I’ve been dealing with my depression. I am concerned about my health now. (Participant F)
Veterans who are exploring their health mission may not be actively engaged in primary care services, but they are beginning to seek treatment for their health problems and gain a better understanding of their health and the system.
Embarking on the Mission
Homeless veterans who are “embarking on the mission” (n = 13 participants) of chronic health management are defined as adapting and adjusting to the management of their chronic health problems. They have made the decision to engage in the health-care process and learn about the steps needed to maintain their health such as navigating the health-care system. Typically, they have established primary care services; however, they may not always make appointments or follow-up when appropriate. In addition, these participants are learning to trust the system, have more self-motivation in regard to their health, and are frequently future oriented. One participant described how he managed his medication schedule while being homeless and moving often: What I would do is get my medications for blood pressure, depression, and anxiety. I would get a three-month supply of medications, so that would hold me over and when that ran out, the VA would give me another three-month supply. (Participant G)
Other participants in this category described the importance of establishing a routine to help manage their lives and health. They also recognized the interrelated nature of their health and homeless status. When they are consistent with their medications and any special type of treatment needed (i.e., wound care), then they are able to concentrate on finding housing and food. However, if their health began to spiral out of control then they were less able to focus on the basic necessities. One participant described what it is like to be homeless and dealing with health issues even with access to health services and how quickly things can change: I miss a lot of doctor’s appointments. When you’re homeless you don’t really have consistent situation, it’s hard to organize your life, so sometimes I do miss doctor’s appointments, which is bad. . . I’m just trying to organize things and sometimes you can have an appointment on such and such a day and then I think where I live and what my appointment is and how problematic it’s gonna be to get there, so it might be easier where I’m at now but someday I might be living somewhere else and I go through this cycle so long, even if I’m in a place where I feel like I’m secure, you always prepare for the worst. (Participant H)
Veterans who are embarking on the mission still constantly face barriers to health and housing, but they are also optimistic about their future and tend to think about continuing to flourish in their own personal lives and stay on a positive track. One participant described what it was like living in the shelter system and constantly being exposed to illegal substances but that it was no longer a problem for him: I sit outside sometimes and guys go back and forth, back and forth, smoking weed, then heroin and drinking, but I don’t do any of that, I haven’t for 6-1/2 years. I’m proud of my clean time and I don’t want to lose it, I just want to continue to grow. (Participant I)
Finally, these participants have a better understanding of their life situation. They know what they need to do to manage their health and what routine works for them. One veteran was able to vividly describe what he needed the most to manage his health problems: Stability is one of the key building blocks of good health and stable health and if you have joy and happiness in your life, health wise you have a tendency to be more healthy than someone who is living on the street, worrying about somebody taking their stuff or being killed on a 24-hour basis, and you sleep in your own bed, you are behind a secure area, and special people with PTSD tend to relax. (Participant J)
Those participants who are embarking on the mission of chronic disease management tend to have a more positive outlook on their health and lives because of the constructive choices they have made regarding their health. They are becoming more aware of their health needs and actively contribute to the health process to meet those needs.
Embracing the Mission
Homeless veterans who are “embracing the mission” (n = 5 participants) are defined as those successfully managing their chronic health problems in their daily life. They are committed to their health and have integrated their health needs into their normal routine. These participants practice preventive behaviors, are more health literate, have taken full ownership of their health situation, and are willing to commit to what is necessary to maintain their health. They are more health literate because they understand how to manage their diseases and what signs and symptoms to be concerned about. One HIV positive participant, described his complicated medication routine and how he adapted to managing his medications while being homeless: Two of my anti-retroviral medications I have to take with food and if I’m not at a place where food is available, in other words, I take it on a daily basis I just have to wait until mealtime or go to a soup kitchen that is available that is accessible and take it after that, I could never take it on an empty stomach because it’s upsetting. (Participant K)
This participant understood the side effects of his medications and the importance of taking it with food. He was able to adapt his health routine while being homeless and still manage his HIV. Participants that embrace the mission continue to face barriers as all homeless veterans do. However, they are able to see past those barriers and understand the whole picture of their health. One participant had recent back surgery and was staying at a shelter. He ambulated with the assistance of a walker. He described the circumstances he faced just to get to an appointment from the shelter: Well it was hard, trying to get back and forth to the hospital, you leave here at 7:30am, they don’t pick you up until 3:30 or 4:00pm, so you got the whole day up there. . .then I had to go to UC, so I had to walk from the VA to UC, see the doctor over there and then walk back to the VA to catch the ride. . .that was a hard day that day because I walked and I could barely walk anyway, but I made it and just dealt with it. (Participant L)
These participants remain committed to their health and tend to stay positive and hopeful rather than focusing on the negative aspects. One participant with significant chronic health problems described how he maintains a healthy outlook on life despite being homeless: Don’t let the situation get you down, if you start letting stress and that get to you that’s gonna cause you more problems and you just take it a day at a time and whatever is bothering you, do the best you can with it and if this is going on, maybe they can do something else, but the more you try to help yourself, the better off you’re gonna be. (Participant M)
By “embracing the mission,” these homeless veterans have moved on from blaming others for their situation, have taken full ownership of their health problems, and frequently described experiences of hope and joy in their lives.
Additional Findings
An additional and unique finding from this study is that the sample of participants were from the Vietnam/post-Vietnam era. This characteristic was not part of the inclusion criteria, but merely a result of the target population from which recruitment took place at the three sites. The Vietnam/post-Vietnam War era was socially and contextually different than any later military war era (i.e., Gulf War, Iraq/Afghanistan). These veterans tend to suffer disproportionately having significantly worse physical and mental health compared with other veterans (Villa, Harada, Washington, & Damron-Rodriquez, 2002). Therefore, a veteran’s service during this era may have played a significant role in the defining factors of each individual participant’s homelessness status.
Discussion
Outcomes from this study indicate there are four ways in which Vietnam/post-Vietnam male veterans who are homeless manage their chronic health problems. These four ways (i.e., deferring, exploring, embarking, and embracing) provide researchers, health-care providers, and stakeholders with new knowledge that can be used to produce more effective interventions to treat the many chronic health problems that veterans who are homeless endure. Previously published literature is often lacking in theory-based interventions that can result in patient-centered outcomes. Instead, focus is placed on identifying medically based interventions that will affect homeless veterans as a group (O’Toole et al., 2013). This stance utilizes a broad “one size fits all” approach and does not consider that members of this vulnerable population may manage their health in different ways. Narratives describing experiences of deferring the mission were very different than narratives of veterans who described embracing the management of chronic health problems. Not all veterans who are homeless are able to embrace the mission of managing their chronic health problems and may not be ready to actively engage in the health-care process. These findings provide insight into the individualized experiences of homeless veterans with chronic health problems, which can help contribute to developing future patient-centered approaches that provide the best possible health outcomes for this population.
Moreover, findings from this study corroborate results found in previous research on barriers related to health care that homeless veterans face (Blue-Howells et al., 2008; Goldstein et al., 2010; Weber, Lee, & Martsolf, 2017). Study participants frequently identified transportation issues and service fragmentation in the health care system as major concerns. Although, as depicted in the study findings, those obstacles can play a major or a minor role in a veterans’ life, depending on the way homeless veterans manage their health problems. Barriers were discussed by participants who managed each of the four ways, but were often more prevalent in the deferring and exploring category (i.e., transportation, access to primary care services). Those participants embarking upon and embracing management of their chronic health problems often took ownership of their health problems and did not provide justifications for not seeking health services or missed appointments. In addition, those participants who accessed the VA health-care system (n = 24, 75%) often described more health- and social-related resources to help better manage their chronic diseases and obtain permanent housing.
To reduce barriers to receiving health care for this vulnerable population recommendations include the co-location of services and utilizing community outreach programs to enhance connections and support. The co-locating of services allows for patients to receive medical care, mental health care, and social services all in one location at potentially the same time (Blue-Howells et al., 2008). This reduces the need for multiple visits, at potentially multiple locations, and with multiple providers where they would have to explain their personal situation to numerous individuals (Blue-Howells et al., 2008; O’Toole, Johnson, Redihan, Borgia, & Rose, 2015). In addition, outreach programs that connect with patients in the community and increase health care visibility have the potential to bridge gaps in care management (Zucker, Choi, & Gallagher, 2012). Veterans deferring the mission of health care management may be able to move to exploring the mission of health care as barriers are reduced and they can begin to explore and learn how to manage their health. With the aid of supportive services significant barriers can be reduced and even overcome.
It is also important to look at the potential role that “masculinity” and male role norms play when homeless veterans work to manage their chronic health problems. Men are more often socialized toward achievement and independence (Liu, Stinson, Hernandez, Shepard, & Haag, 2009) while remaining stoic, controlled, and self-sufficient (Mahalik et al., 2003). Conforming to these male gender norms may have influenced the way (deferring, exploring, embarking, and embracing) veteran participants manage their chronic health problems. A homeless veteran may delay (defer) seeking treatment for their chronic health problems because of society norms that indicate men should be independent and self-sufficient. Research has also shown that men are less likely than women to seek help, particularly for mental health conditions (Addis & Mahalik, 2003; Galdas, Cheater, & Marshall, 2005). Over half of the study participants reported being diagnosed with a mental health issue (anxiety/depression, PTSD, substance abuse). Therefore, study participants may have underreported mental health issues or felt they could be controlled on their own and not needed to seek help. It is difficult to determine how significant the role masculine norms played in this study as men of varying age, social status, and ethnicity may react differently (Galdas et al., 2005). Further exploration of this phenomenon is needed, thus future research with homeless veterans attempting to manage their health problems should include exploring the role of gender norms in this process.
Implications for Nursing
From a historical perspective, the profession of nursing has long strived to provide a more holistic approach to patient care that considers the “whole” person, which involves optimizing all aspects of their health including physical, mental, social, and spiritual care (Thornton, 2008). This approach that focuses on the “whole” of an individual is compatible with the needs of veterans experiencing homelessness while attempting to manage chronic disease per study findings. Qualitative inquiry, such as grounded theory utilized in this study, provides a unique view of the individuals own experiences when attempting to explain the social world of homeless veterans managing chronic disease and to develop an explanatory theory to explain this phenomenon (Morse & Field, 1995). Other qualitative research methods have highlighted the need for holistic, individualized care with homeless populations (Mabhala, Yohannes, & Griffith, 2017; Watson, Crawley, & Kane, 2016; Weinrich et al., 2016) and the need to focus on their health but also social conditions to improve quality of life outcomes.
Limitations
A limitation of this study was self-disclosed veteran status. Participants were not asked to provide official identification or documentation of military status. However, due to the specific nature of the topic and the initial demographic information collected, it would be challenging for an individual to falsify any claims related to military enrollment and experience. Another limitation of this study is that participants were interviewed at one point in time. Homeless populations are historically nomadic and often cycle in and out of homelessness as evidenced by the multiple episodes described by the study sample. This study was able to only capture a single snapshot of the described experiences of homeless veterans living with a chronic health problem.
Conclusion
Chronic disease management among the homeless Vietnam/post-Vietnam veteran population is a complex phenomenon that was captured in this study with the central concept of pursuing the mission. To be most effective, chronic disease-based interventions with veterans who are homeless should focus on the four specific ways that they attempt to manage their health rather than one general approach. All participants in this study were able to describe in their interview one of the four different ways that they utilize to manage their health. This study helped to gain a better understanding of the health needs of a population that has honorably worked to serve and protect their country. Finally, study findings can confirm the need for continued work to improve the health and quality of life among this vulnerable population and ultimately contribute to the goal of ending veteran homelessness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Jillian Weber PhD, RN, CNL disclosed receipt of the following financial support for the research, authorship, and publication of this article: The Department of Veterans Affairs VISN 10 through a Patient-Centered Research Initiative Program Grant (RIP).