
Abstract
With one of the highest rates of poverty and HIV in the world, Malawi faith-based organizations (FBOs), non-governmental organizations (NGOs), and community-based organizations (CBOs) are expected to provide tangible and emotional support to people living with HIV (PLWH). Using Lin’s social capital theoretical approach, we examine the perspective of PLWH regarding the adequacy of support responses. Forty-six rural Malawi HIV+ adults provided interviews that were recorded digitally, translated, and transcribed by Malawi research assistants. Atlas.ti was used to organize the data and to aid in the analytic process. Participants expressed disappointment in the lack of resources that could be accessed through the FBOs although their expectations may have been unrealistic. Outcomes from accessing and mobilizing the FBO network were negative in terms of stigmatization by FBO leaders and members, whereas outcomes related to CBOs and NGOs were generally positive in terms of empowerment through HIV information and attendance at support groups.
Keywords
Social capital theory has gained currency in the health outcomes research literature related to the recognition that membership in social networks can influence health outcomes. Social capital is generally viewed as a multidimensional concept with origins in both economics and sociology. Social capital attained through membership in community-based organizations (CBOs), such as faith-based organizations (FBOs), non-governmental organizations (NGOs), and CBOs has been examined as a potential moderator of risk-taking behavior and an important source of encouragement to achieve health goals (Campbell et al., 2013; Webel et al., 2012). We examine social capital from a social support and social network perspective whereby people who are embedded in a social network have access to goods and/or money, information, emotional support, and encouragement to engage in healthy behaviors. In particular, we utilize Lin’s (1999) network theory of social capital to examine social capital available to people living with HIV (PLWH) in rural Malawi to determine if the social network’s provision of resources influence mental health and life satisfaction in this vulnerable population.
Social Capital and Network Theory
Lin’s Network Theory of Social Capital, which as Lin (1999) emphasizes is attained from “embedded resources in social networks,” is useful in examining the precursors of social capital, the elements of social capital, and the “returns” from beneficial outcomes related to accessibility and mobilization of the social capital network. Lin notes that social capital has been approached from both an individual perspective and a community orientation; we utilize Lin’s individual perspective to understand how social capital may operate in situations involving Malawi PLWH. We make the assumption, based on our work in Malawi, that the FBOs are a major part of the collective assets and are embedded in the structure of the social system. According to Lin’s (1982) social capital theory, social capital comprises the resources embedded in a social network that are accessed and/or mobilized in purposive actions. He points out that social capital contains three elements: resources embedded in a social network or structure, accessibility by individuals to the resources provided by the social network or structure, and use or mobilization of such social resources by individuals in ways that benefit them (Lin, 1999). Accessibility, as defined by Lin, is the degree to which social resources are available to individuals. Mobilization is the operationalization and the use of social resources in the community by individuals. Figure 1 illustrates the concepts of the network in which we are most interested; these concepts are those elements of the figure that are outlined with bold borders.

Adaptation of Lin’s social capital model (with permission).
We are particularly focused on the concepts of accessibility of the FBO network for FBO members who are living with HIV and the mobilization of the FBO network to provide social resources to PLWH. We posit that the mobilization of the FBO network by PLWH will lead to an improvement in PLWH physical and mental health. The middle section of Lin’s theoretical model illustrates the components of social network processes (accessibility and mobilization) and the far right column reflects the outcomes afforded by social capital including returns (instrumental and expressive returns). The far left block in the model, that is, what we refer to as precursors of social capital, is not examined as the interview data do not provide information on the collective assets or the structural and positional variations. However, because we examined the structure of five different FBOs in other parts of this study, we are aware that the FBOs are lacking financial resources, although as thought leaders in their communities the clergy and imams have considerable opportunity to influence the norms and values of their constituents. The government of Malawi recognizes FBOs as an important community resource, and communities rely on the FBOs for leadership and the provision of instrumental and emotional assistance. Nonetheless, as in many sub-Saharan African countries, the government provides little direct financial assistance to FBOs other than their support of mission-based hospitals. Most of the western Christian FBOs, that in the past supported mission-based hospitals, have withdrawn their financial support (Schmid, Thomas, Olivier, & Cochrane, 2008). Likewise, support to such women’s organizations as the Mothers Union (Anglican), youth organizations, and to the churches themselves has been removed.
Malawi FBOs
Religious organizations are of particular interest in the struggle for HIV prevention and service delivery as they most often provide the only infrastructures reaching rural areas, where the majority of Malawian people live. Approximately 83% of Malawians are Christian, 13% are Muslim, and 4% practice African traditional religions or claim no religious affiliation (The World Factbook: Malawi, 2016). Religious leaders are frequently accorded respect as opinion-leaders in their communities. And whether in urban or rural settings, religious bodies tend to be the custodians of values influencing behaviors—paramount among these are compassion, community service, and care for the whole person. In religious ceremonies, leaders have a public platform from which to challenge destructive prejudices that reinforce stigma, while conveying important information concerning HIV prevention and care.
However, religious groups also have engaged in harmful teaching and practices that promulgate inaccurate information, HIV-related stigma, and other judgmental attitudes and behaviors. Fear of stigmatization and subsequent abandonment and rejection were found to deter subjects from being tested for HIV in a study of rural Malawians (Iroezi et al., 2013; Sliep, Poggenpoel, & Gmeiner, 2001). Theologians and ethicists, many from Africa, have addressed the moral, philosophical, and religious aspects of stigma in an effort to reverse the phenomenon and the accompanying discrimination that is so damaging to PLWH (Morris, Schell, Schell, & Rankin, 2008; W. Rankin, Brennan, Schell, Laviwa, & Rankin, 2005).
Malawians Living With HIV and AIDS
With a population of approximately 17.9 million people in a small landlocked country with few natural resources, there were about 1,063,900 PLWH and 32,600 deaths in 2014 (The World Factbook: Malawi, 2016). Although the prevalence of HIV infection has leveled off to approximately 11%, the Ministry of Health has few resources to deal with this overwhelming level of infection. Therefore, PLWH in Malawi are reliant on family members and local social support resources such as churches and mosques, CBOs, and NGOs.
Purpose and Objectives
The purpose of this article is to present findings from interview data collected from 46 Malawians living with HIV and AIDS, and to describe the perspectives of PLWH and their FBO’s response to the epidemic. Our objective is to use Lin’s framework to organize the data and to explore Malawi FBO, NGO, and CBO provision of social capital to influence PLWH physical and mental health and life satisfaction. The secondary objective is to develop strategies to enhance social capital for PLWH.
Method
Project Partners, Study Participants, and Setting
We present a cross-sectional study that was part of a larger federally funded parent mixed methods project (RO1HD050147) that partnered with and utilized the resources of an international NGO working primarily in Malawi to reduce stigma and enhance HIV prevention and care through churches and mosques. This organization’s long-standing ties to numerous FBOs allowed us to examine five religious groups: three mission-based Christian groups, one indigenous Malawi Pentecostal group, and Muslims who were represented by two Islamic groups. Table 1 demonstrates participants’ pertinent demographic and health data.
Demographic and Health Characteristics of 46 Malawi People Living With HIV.
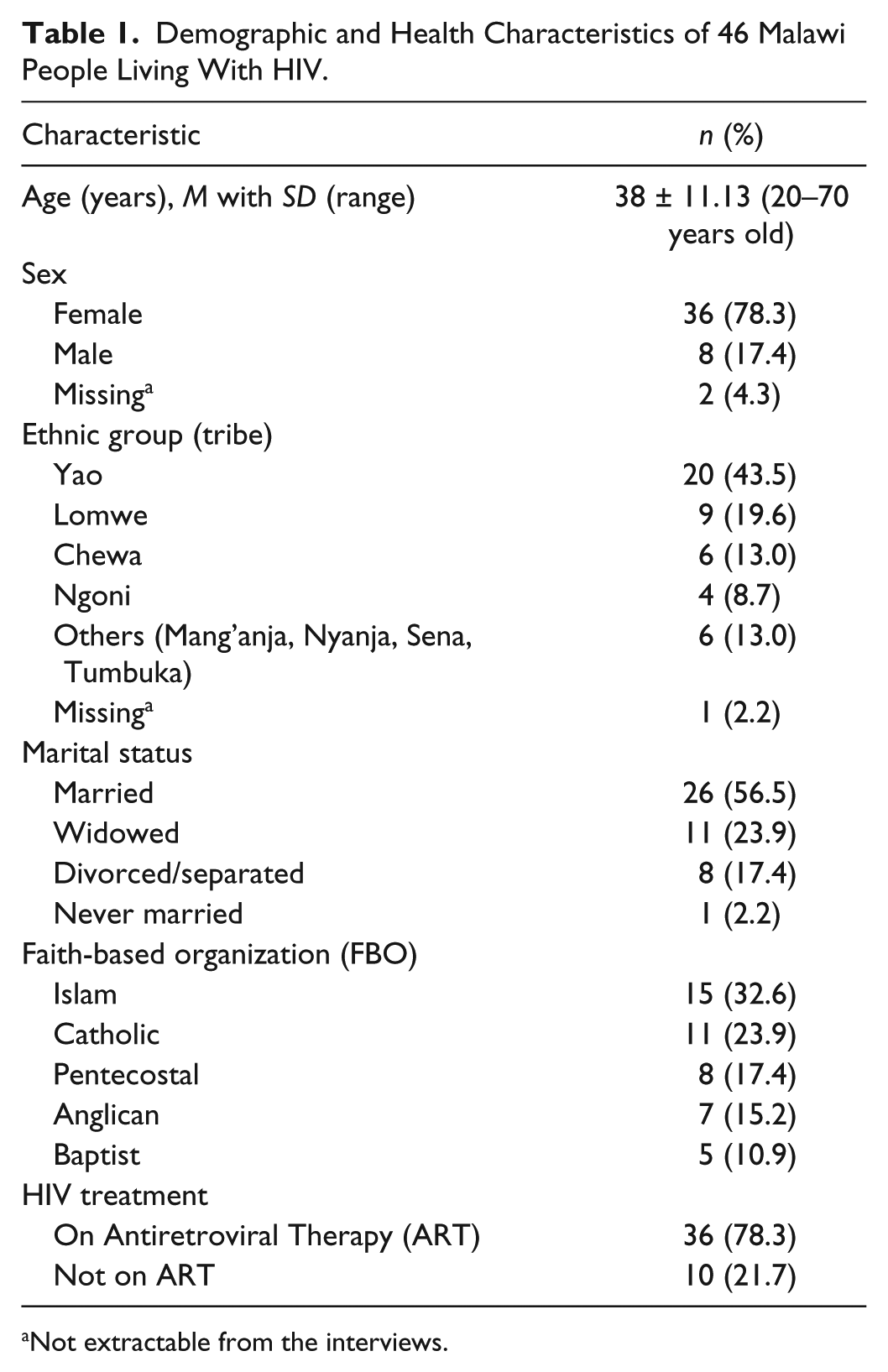
Not extractable from the interviews.
A total of 46 PLWH from various village CBOs were interviewed in settings that were chosen by the leaders of these CBOs. These were usually the sites where their informal support groups met or were convenient to the villagers but also private. As data were collected during the dry season, most villagers were not working in their fields.
Human Subjects Protection
Approval for the study was obtained from both an academic institutional review board and from the Malawi National Health Sciences Research Committee (MNHSRC). Participants were given two bars of soap as appreciation for their participation in the study. Anonymity was protected through the use of numerical codes as identifiers and confidentiality was protected through privacy afforded during interviews. All interview data were stored in locked files and interviews were erased from digital recorders.
Data Collection
We had originally planned to recruit six to 10 PLWH (30-50) from each of FBOs, linking PLWH data with our church/mosque leader and member data. Based on on-going analysis within the parent project, we expected that 30 interviews would probably be sufficient to describe and compare PLWH perspectives across the five FBOs, but we built in the possibility to do more as needed to reach saturation of emerging themes. However, due to issues of stigma, few FBO members had disclosed their status to their church/mosque leaders. Therefore, PLWH were recruited through community-based HIV support groups that were accessed through contacts the NGO had developed with religious organizations and referrals from our Malawi consultants representing each of the five FBOs. These support groups were village based and had members who represented a variety of FBOs, both Christians and Muslims. We contacted the leaders of these support groups, informing them about the study and asking them to refer potential participants who were members of the five FBOs in the study. These leaders instead requested that we show up at a certain time and place and PLWH from their support groups would come to us if they wished to participate in the study. Although we asked for about five to 10 per support group (for an expected sample of 30-40 participants), several groups sent more participants and we felt ethically bound to enroll (and gift) all who came (N = 46), regardless of their FBO affiliation. Upon arrival at the designated location, the project was explained to the PLWH and information sheets in Chichewa, the primary language used in Malawi, were read to the participants. If they remained interested, verbal consent was obtained. Interviewers were Chichewa-speaking Malawians from urban areas not affiliated with the support groups and were trained by the U.S. and Malawi research team members.
The purpose of these interviews was to determine the PLWH viewpoints regarding how their FBOs have responded to the HIV epidemic, including provision of goods and services, emotional support, and advocacy within the religious group. Semi-structured interview guides were used to explore issues related to how PLWH learned their status, where they get assistance (resources), and how their church/mosque has helped them and other members affected by HIV or AIDS. Each interview lasted at least 1 hour, was audio recorded, translated into English, and then transcribed by Malawi research team members. Working together with the U.S. team, the Malawi researchers explained Chichewa terms and local customs with which the U.S. team was unfamiliar.
Data Analysis
Qualitative description was used to reduce, organize, categorize, and thematically analyze the semi-structured interview data. Qualitative description involves a type of analysis that is “low inference” and less interpretive, not requiring a “highly conceptual or abstract rendering of data,” making it useful for researchers who wish to obtain “unadorned” or “minimally theorized” answers to specific questions (Sandelowski, 2000, pp. 335, 337). Atlas.ti, a computer software program that provides for organization and categorization of large bodies of textual data, was used to manage the volume of data and to aid the analytic process. The U.S. research team individually read the transcripts and open coded the data without regard for relative importance of initial codes. This phase of analysis served as data expansion and allowed for an understanding of the breadth of ideas and concepts expressed in the interviews. After initial coding, the U.S. based research team, consisting of the principal investigator (PI), project director, a pharmacist, and two doctoral students, reviewed the data again and developed an analytical strategy that focused on the concept of social capital. A coding scheme reflecting social capital was developed and the data were recoded using this schema. The team met multiple times to discuss coding patterns until saturation of the emerging themes was reached. This iterative process increased the trustworthiness of the analysis.
Qualitative validity was ascertained using “verification [which] refers to the mechanisms used during the process of research to incrementally contribute to ensuring reliability and validity and, thus, the rigor of a study.” (Morse, Barrett, Mayan, Olson, & Spiers, 2002, p. 17). In our study, verification was achieved by such mechanisms as the PI, co-investigator, and project director (PD) directly interacting and interviewing Malawian participants who spoke English, accompanying Malawian research assistants to interviews to observe data gathering techniques and body language, speaking with local Malawian informants who were not participants in the study about the situations of rural PLWH, their roles in rural villages, and assistance they might receive from NGOs and FBOs. We then used these data in an iterative fashion while we examined the transcripts from the interview data.
Results
Although we were originally interested in FBOs as a source of social capital, it became clear that participants also garnered support from NGOs and CBOs. They indicated that they obtain some of the needed resources, such as antiretroviral medications (ARVs) and condoms from governmental agencies (hospitals/health centers), NGOs, and CBOs but struggled to meet basic living requirements. Additionally, some participants revealed that they turned to traditional healers for assistance with their HIV and social situations to remove curses.
In countries like Malawi, FBOs often create needed social capital and structure at the community/village levels through their processes of teaching about God/Allah, visiting the sick, and networking to develop community-/church-/mosque-based projects. However, the data revealed a discrepancy between PLWH’s expectations of accessibility and mobilization of FBO resources and the receipt of assistance or support from their FBOs. This disconnect was partially mediated by the continued problem of stigmatization of HIV positive individuals that impacts disclosure practices and outcomes of mobilizing potential social capital at the community level. The findings are presented using Lin’s network and social capital theory, focusing on accessibility, mobilization, and expressive returns. The first “block” (Lin’s term) that we addressed is referred to as Social Network Processes, and includes accessibility and mobilization.
Accessibility
Lin indicates that accessibility reflects network locations and resources, that is, what resources are available to be mobilized and where these resources reside. It is clear that some of the most important resources for PLWH come from hospitals/health centers and NGOs that supply these health centers. NGOs may arise from local Malawi groups or, more generally, are international organizations such as Population Services International, Save the Children, and Oxfam. International NGOs usually have funding that can be used to provide HIV testing, ARVs, and other material supports. Other organizations such as FBOs and CBOs were mentioned by participants as potential sources of support to PLWH. FBO resources reported as needed by participants were spiritual guidance/counseling and more tangible resources needed to survive that include food; money; assistance with household activities, such as cooking and cultivating land; and taking care of orphans. CBOs in Malawi are those indigenous organizations that arise from individuals or small groups of Malawians and tend to provide such services as support groups, informal household assistance, and other supportive inexpensive help. When we asked PLWH what assistance they needed and where it came from, participants made a clear distinction between assistance from CBOs, NGOs, and FBOs.
CBO/NGO resources
All of the PLWH were recruited through community-based support groups, some which received help from NGOs or Malawi’s National AIDS Commission (NAC) but none of the support groups were explicitly connected to a church or mosque. It was through these community-/village-based support groups that PLWH accessed various resources including knowledge dissemination, emotional support, or “encouragement.” PLWH also access knowledge via the radio and family members. One FBO member explained the resources available through his support group:
I learn about HIV/AIDS from the radio and AIDS Support Group meetings where all of us who are HIV positive go there and share our experiences, not forgetting the hospital where we go to get ARVs. Our group helps other people in our nearby villages; those people who lack counseling, we even take condoms to them so that they can be helped; the condoms are for both males and females, we also take other people for VCT to the hospital so that if they test positive, they can start ARVs.
While some community-based support groups have emerged organically from communities, the most successful have been created or nurtured through support from governmental or international NGO sources, including the National Commission on AIDS (NAC). With outside resources, these CBOs can also provide more tangible resources including fertilizer, food, and mutual assistance in subsistence farming: “Like from NAC, we have received items like fertilizer and some bags of maize, so with these, we did some farming.”
However, CBOs themselves are, at times, plagued by uneven access to resources, particularly when funding for the support groups ends and they are expected to carry on without external inputs. Additionally, Malawi has struggled with corruption at various levels of the political and social system, which has led to inequitable distribution of resources based on who you know rather than need.
FBO resources
FBOs are conveniently situated within the fabric of the community to model appropriate behavior, and visiting the sick is a common practice among most churches and mosques. Additionally, as places of worship, there is potential for community members to seek strength and refuge in times of need, and FBOs can offer supportive environments for PLWH to cope with their illness through semi-formalized FBO structures such as weekly Bible or Qur’anic studies or organized groups that carry out the work of the FBO. For example, women’s groups, such as the Anglican Mothers’ Union, are common throughout Christian and Muslim FBOs as are youth groups. The women’s groups are often the ones charged with devising plans to visit sick FBO members. However, the findings from this study that relate to the accessibility of such FBO resources indicated that there was a discrepancy between PLWH resource expectations and reality. The notion of expectations emerged in response to questions about whether the FBOs offered assistance to PLWH and met their various needs, particularly after disclosure to either the clergy or to congregation. Unrealistic expectations and perceived value of resources emerged as subcategories in our analysis.
Unrealistic expectations
Unrealistic expectations of FBOs were mostly expressed as dissatisfaction with the church or mosque in providing assistance or care, although participants recognized the FBOs may not have been aware of individual needs or HIV status. Because of the stigma associated with HIV/AIDS, most participants had not disclosed their status yet expected to get help: “Oh to say the fact, they [the FBO] have not helped me. I didn’t tell them about my status.” This expectation was predicated upon their assumptions that the FBOs should be aware of their needs without explicit disclosure of status. Lack of communication about their situation but with the expectation of assistance led to dissatisfaction. “I am not satisfied because [the FBOs] don’t help me with anything, maybe I could have told them, maybe they could have helped me, but at this time, I am not satisfied with anything.” However, some of the PLWH recognized that their fellow FBO members were themselves resource limited and therefore appreciated what assistance was offered. “Yes, they [FBO members] help me, especially when I am sick . . . I am very satisfied with the little they give me because I cannot force them to give me more while they have a little themselves.”
Perceived value of resources
The poverty in Malawi is profound and the needs of PLWH are significant. Some participants expressed expectations of assistance from the church to be tangible or financial, while easily accessible assistance, such as knowledge, counseling, and spiritual encouragement, were not necessarily viewed as useful or valuable. Some of the spiritual messages were individually directed toward PLWH members:
There is nothing the church has done to help me apart from the encouragement that my pastor told me that I have not to stop praying to God because HIV/AIDS is an epidemic. They (church leaders) don’t help us but they just encourage us to be faithful to our husbands because nowadays the world is in danger . . .
Visiting of the sick is a norm within Malawi FBO culture and some PLWH indicated that they were visited in their homes by FBO members: “When someone is sick, the church members indeed come and visit us; like now, my wife is down with a headache and they came to visit her.” However, the form of assistance this visit provides is not fully articulated. Other participants indicated that home visiting did not necessarily happen: “There is not any other group which visits the sick in their homes.” Home visits by FBO members provided more spiritual support, in the form of praying for the sick FBO member, than tangible assistance. Therefore, this type of visit was not perceived as meeting the real needs of PLWH as articulated by one participant:
They face problems like hunger, lack of clothing, and some lack farm inputs such as fertilizers and also household belongings. There is also lack of good food as ARVs need good food.
Thus, we noted that while the data demonstrated limited resources available from the FBOs, members expected more and were therefore unhappy with the accessibility of resources from FBOs.
Mobilization
Lin (1999) defined mobilization as the operationalization of social resources in the community by individuals. The data revealed that some resources, such as HIV knowledge/information and encouragement/support, were distributed without any effort on the part of the PLWH, but the mobilization of other potential resources were, at times, difficult to achieve. Three subcategories capture the processes and outcomes of mobilization: encouragement, information, and unmet needs.
Encouragement and information
In Malawi, participants often referred to “being encouraged” when they spoke about messages coming from FBOs and CBOs. These messages included encouragement for partners to be faithful to each other to prevent HIV: “Sometimes when they are preaching they do include [faithfulness] like they say that it is good for a man to have one wife and not have many sexual relationships . . . ”
One of the most important features of mobilization identified in the data was information that was made available to community members by FBOs, NGOs, and CBOs. Many of the informational messages pertained to abstinence and condom use, but the messages were different by source, that is, FBOs were generally negative about condom use while CBOs were positive. Abstinence-only sex education has been attributed to a reduction in HIV infection rates in some parts of Africa, and our findings demonstrated preaching to congregations on this topic consistently emphasized abstinence and condom use has remained taboo. When asked if the FBO provided any information on condom use, one of the participants responded:
All they say is abstinence, abstaining, and abstaining. They do not touch on condoms at all . . . what I know is that they have not touched the topic of condoms explicitly because they feel it is opening up people to bad behavior . . . Condom messages are very silent in church but other organizations talk about those things and that helps people.
Although HIV messages are being disseminated by both FBOs and CBOs, other potential resources are more difficult to mobilize. As noted in accessibility, mobilizing home visits by members is challenging when the PLWH is not disclosed. One member articulated his strategy: “Whenever I am sick, I just tell them it is a headache and they come to pray for me not knowing that I am HIV positive.” However, revealing one’s status and needs does not necessarily mobilize available resources, as one Anglican man described:
Yes, I only told the priest that I have problems of food, clothes, and also I have orphans at my house; I told the priest this when we went to [named church] to commemorate the Bishop’s 10 years in office and I was told that I will be assisted.
However, when asked later what the church had done to help him he stated, “The church has not assisted me in any other way but if you talk of the support group, then they have assisted me.”
Unmet needs
The needs of villagers in Malawi are significant and neither the CBOs, FBOs, nor the NGOs were able to fully meet the needs of PLWH. One CBO had given members of a PLWH support group some farm inputs, which included eggs but what was given was not perceived as sufficient. “We also received money for buying eggs so that we can [have] some business, but it looks like the eggs are not enough; we share 10 eggs for each for the whole month, which is not enough.”
FBOs were likewise perceived as not providing sufficient resources to PLWH members. This was most evident in the area of orphan care. FBOs traditionally played an important role in caring for orphans and could still provide critical resources to members caring for orphans but as one PLWH noted, mobilizing assistance may not be possible. Indeed, there is evidence of a lack of mobilization to care for the orphans resulting from the pandemic; this was reported by a PLWH who stated,
Our church supports the orphans when there is a serious problem . . . but there is no program specially designed for supporting orphans. Some orphans are supported by non-governmental organizations. But as you can see the church does not support these orphans the way they are supposed to; like myself as I have already explained I have 10 children who are orphans but the church does not support me in any way yet all these children need school fees . . .
The next section of the article presents the outcomes from PLWH attempts to garner social resources from their various FBO, NGO, and CBO networks.
Returns From Accessibility to and Mobilization of the Social Network
If individuals are able to access and use the resources within the social network then the investment in social resources is expected to result in returns that benefit the individual. In turn, individuals not only gain from their investment in the social network or social structure but they also benefit the network. However, Malawi PLWH have little to invest in social networks unless they participate in social support groups or role model successful lifestyles to others:
I can also assist other people although I am poor myself, but I try my best to go and visit people who have AIDS . . . It’s not at all satisfying to them because I am also poor, so the assistance that I give them is little because I am also afraid that I can lose more; but still more, I try to help my colleagues.
Nevertheless, this type of investment does provide returns to the social networks. Lin (1999) refers to the outcomes of social network processes as instrumental and expressive returns. We examine the returns in terms of those provided by FBOs and those provided by CBOs.
Instrumental Returns
According to Lin’s (1999) theory of social capital, the activities improving accessibility and mobilization to social capital can yield fruitful returns to both health and instrumental consequences such as wealth, reputation, and power. The instrumental returns are the gaining of added resources that the individual did not possess previously. Our data indicate that there were limited instrumental returns in terms of power, through the empowerment gained by new knowledge and participation in CBO-led support groups. However, there were negative instrumental returns related to the effects of stigma on PLWH reputation.
Power/empowerment
Empowerment skills related to HIV care was a positive return from social capital mobilization. Once PLWH accessed HIV care, one of the immediate returns was improved knowledge about HIV and how to utilize existing health care systems and resources available in communities. The majority of the participants articulated the process of accessing ARVs, the nature of disease progression, and the mechanism of ARV action. This knowledge was relayed to families and friends while encouraging them to get tested for HIV.
I know all the process. What happens is this. For a person to start taking ARVs there are two or three things that happen. First of all you have to be tested for your CD4 count. WHO standardizes the clinical stages. And people like us who are active in HIV/AIDS things we are familiar with the staging of the ARVs.
Engagement with support groups also empowered PLWH to share their HIV burdens with others.
Honestly speaking I did not speak in public or in front of a large group of people, but I did mention it [disclose] to the HIV support group . . . We help each other with ways how to promote our livelihoods as people infected by HIV. We also try to encourage each other against stigma and discrimination . . .
The empowerment of PLWH who attended support groups is an obvious example of the positive instrumental returns related to accessibility and mobilization of the support groups related to HIV. Nonetheless, returns related to reputation were often harmful as the interviews revealed that HIV stigma was still alive in FBOs and delayed disclosure and promoted disengagement from FBO activities.
Because some people are not secretive—when they see you moving around in the village, they tell some people that “have you seen that person, he is HIV positive.” So I don’t reveal my status to other people [in the mosque] but only my relatives. They say we cannot be employed by some people or other organizations because we are HIV sick.
Damage to reputation/stigma
PLWH are often discouraged to disclose their status due to fear of being ridiculed, discriminated against, and isolated. This is a critical dilemma that often hinders access to resources and is at times reflective of the messages coming out of the FBOs. If the FBOs are preaching that HIV/AIDS is caused by unfaithfulness and promiscuity, as was reported in this study, then disclosure becomes a direct admission of sinning. “You know here in Africa sexual behaviors are paramount to spreading AIDS so most messages pertain to that idea that sex is bringing AIDS and premarital sex or extramarital sex for example is being very sinful.”
Additionally, some PLWH have been indirectly singled out and isolated in an attempt to provide them with counseling, an approach that further fuels the discrimination and stigma. “People are afraid to tell their fellow members because they cannot keep a secret . . . so we meet the pastor in secret because he prays for us.”
Congregations have been reported to contribute to this discrimination via rumormongering, which further creates social tension and compromises any social cohesiveness that could otherwise promote socially supportive interpersonal processes:
. . . But other people just don’t take good care of the people who have AIDS, they just discriminate against them. When you have revealed that you have AIDS and you have started getting ill, they neglect you, saying you are sick from AIDS . . .
Another participant said, “Even if I revealed, I would have been insulted and discriminated against by my fellow church members.” Expressive returns are the second type of outcome to which Lin refers. Data from the interviews support the accessibility and mobilization of social resources to enhance physical health.
Expressive Returns
Expressive returns, as explained by Lin, are those returns from accessing and mobilizing social resources that protect existing resources and are usually related to denser networks with reciprocal relations such as those that might be found in a group of PLWH with shared interests and resources (Lin, 1999). Our interviews revealed that expressive returns were primarily related to physical health and to a lesser extent mental health. The positive outcomes were improved health secondary to HIV treatment and more engagement in social networks related to HIV. However, the data are clear that these positive outcomes accrued as a result of NGO and CBO accessibility and mobilization with no evidence of FBO provision of expressive returns.
Physical health
Improved physical health for PLWH was a direct return of accessing and mobilizing health care resources from NGOs. Seventy-eight percent of the participants reported that they were on HIV treatment at the time of the interview. Despite barriers to accessing the treatment such as lack of transportation and nutrition, the participants were confident about their health status as they received the treatment. Considering that the majority of the participants were female, regaining health status was particularly important because they were able to contribute to their families, particularly to their children’s care and be more independent. Also, regaining physical health was fundamental to the process of building their social capital. “I believe in it (HIV treatment) because the way I was suffering; I was chronically ill but when I started taking these medicines, I am able to work, farm and I believe that they are good medications.” Another participant said, “But ever since I knew the problem and started taking ARVs, I am not ashamed. I do tell my friends that I am taking ARVs and that my health is improving every passing moment.”
The physical health returns reported by participants as being mobilized from FBOs were minimal and were primarily oriented toward prevention. These messages were related to abstention from sexual activity or occasionally the use of condoms. Thus, most participants did not connect the FBOs to improvement in their physical health.
Mental health
Physical health led to better health outcomes, including better mental health. For example, the narratives revealed how the changes in health “I feel better,” “have more energy,” “I’m good now,” contributed to improved mental health. Not only did higher energy levels experienced by PLWH but also changes in appearance contributed to reduced stigma associated with HIV. Although the narratives did not specifically identify depression or anxiety, which are prevalent among PLWH in many settings (Rivero-Méndez, Portillo, Solis-Baez, Wantland, & Holzemer, 2009), discrimination against people with HIV was widespread in the communities. Therefore, not looking ill encouraged the participants to be more active and engage with others in their communities.
After a while I said I should tell people at church about my status because the way I look people cannot think I am HIV positive, so I thought I can be an example how this disease is like. You see (I) am one of the deacons at church so I thought I should lead the way so that more people are free to talk about these kinds of things . . . Actually my goal was for more people to go and be tested.
There was no direct benefit from disclosing HIV status. However, the deacon who was willing to disclose his status in church was able to role model the benefits of testing and treatment and thus was able to invest in the social network available to him through his FBO membership.
Discussion
There is a clear discrepancy between the expectations that PLWH have toward the FBOs as supportive social structures, and the resources offered by these religious entities within their financial and denominational capacity. As shown by our findings, this discrepancy is attributed to the poor communication of needs from PLWH, and the stigma and discrimination associated with disclosure, which in turn hinders accessibility and mobilization of social capital. Additionally, the individuals who are brave enough to disclose have experienced both disappointment and loss of trust in their FBO leaders and members.
Although some FBOs may have good intentions toward assisting these individuals, most preventive and supportive HIV/AIDS work, such as condom use promotion, is contrary to doctrinal values. As a result, the ambiguous messages and other practical efforts to meet these PLWH expectations were not reported as successful. Our study findings indicated that many of the FBO efforts to meet the needs of infected individuals were inconsistent, discriminatory, and consequentially led to withdrawal of PLWH from FBOs as a reliable source of social capital. Hence, our findings suggest that FBOs may not be sufficiently equipped to deliver such HIV/AIDS preventive messages nor a social structure that can operate independently to provide necessary goods and services to PLWH.
Research on social capital has emphasized the importance of creating networks in the delivery of services (Burt, 1984). Therefore, to avoid these patchy and sporadic interventional attempts, formal alliances and collaborative efforts are needed among FBOs, NGOs, and CBOs in designing and delivering comprehensive social services aligned and congruent with the needs of this population (Schmid et al., 2008). Recommendations are in order for the religious entities committed to supporting PLWH to target their interventions to the needs of this population and for HIV organizations and other stakeholders to create partnerships that enhance social capital and the wellbeing of PLWH. This is especially true for the mission and mainline Christian FBOs that have withdrawn most of their financial support; this support is crucial to FBO response to the pandemic. Until religious leaders, policy makers, and other stakeholder invest in enriching and strengthening the resources embedded in the communities, this vulnerable group cannot thrive.
In rural Malawi villages, there are few opportunities for PLWH to enhance their wealth, power, or reputation, that is, the usual instrumental returns from social capital. However, the development of PLWH engagement with CBOs and NGOs and the leadership opportunities within them were a significant source of social capital for the PLWH. Instrumental returns such as empowerment from membership in NGOs and CBOs was a tangible return accrued by PLWH who were empowered to advocate for testing and treatment in their CBOs, NGOs, and very occasionally within the FBOs. Such development of leadership particularly at the CBO and FBO level is important to the future development of Malawi and its people and an important strategy for CBOs and NGOs to employ.
The FBO assault to reputation, an important instrumental return, through discrimination and stigmatization of PLWH indicates that many religious organizations are not providing for the needs of their members and in some cases are causing psychological harm. Whether it is possible for FBOs to become less judgmental and more accepting of PLWH is unclear. The “winds of openness” in Malawi have changed attitudes on the part of many FBO leaders, especially in the urban areas (S. H. Rankin et al., 2011). However, villagers are slower to change and their FBO leadership is less educated and open to new ways to interpret religious literature and beliefs. These findings are consistent with previous studies as well. We have found in past studies that FBOs offered little support to PLWH and also reinforced gender-based stigma toward women (S. H. Rankin, Lindgren, Rankin, & Ng’Oma, 2005). Additionally, in our quantitative analysis of data from this study, we found that religious leaders’ stigmatizing attitude negatively affected HIV prevention and care behavior (Lindgren et al., 2013; S. H. Rankin, Lindgren, Kools, & Schell, 2008).
Expressive returns from mobilization of social networks such as NGOs, CBOs, and FBOs in the areas of physical and mental health were consistent with previous studies, in which PLWH who disclosed their HIV status and engaged in CBOs tended to demonstrate better physical and mental health status including less stigmatization from disclosure (Gregson et al., 2011; Sivaram et al., 2009). Well-informed PLWH utilized resources from hospitals, CBOs, NGOs, and occasionally FBOs and thus became healthier in appearance, which improved their position in their communities as they were able to work and care for their families. This improved physical status and ability to function well within their roles may have led to better mental health although this is not addressed specifically in our data.
Limitations
The pervasiveness of HIV stigma in Malawi leading to the lack of disclosure of HIV status to FBO leaders and/or members forced us to change our PLWH recruitment plan. Being unable to recruit PLWH from the churches/mosques in the parent study, we sought assistance from existing community-based HIV support groups that included members from a variety of religious organizations in Malawi. We interviewed all PLWH that came to participate in the study regardless of religious affiliation, potentially limiting our ability to compare across FBOs. However, just as in the parent study, we found no substantive difference in the perspectives of PLWH on available and accessible resources and outcomes of social capital. All of the PLWH in the study had experience with accessing resources from NGOs and CBOs, so their perspectives and expectations could be different from PLWH living in areas without HIV support groups. As with all qualitative research, this study is context specific; participants came from districts with high HIV prevalence and the experience of PLWH living in regions with low prevalence might be different.
Conclusion
Although FBOs provide important social leadership networks in resource-limited rural communities in Malawi (Lindgren et al., 2013), we were disappointed to find the minimal contribution of FBOs to PLWH empowerment, reputation, and physical and mental health, all outcomes of social capital. We believe that it is worth investing in FBOs as potentially they have the ability to improve the lives of PLWH. Indeed, FBOs could be more effective if they cooperated with NGOs and CBOs so that a more integrated approach to HIV could be attained. Organizational strategies are apparent at the national level in Malawi with such organizations as the Malawi AIDS Interfaith Alliance and various organizations that oversee the CBOs and NGOs; collaboration among these entities could enhance the work of the FBOs. Individuals and organizations involved in global health initiatives, coming from the perspective of enhancing individual- and community-level social capital, could be the facilitators of such a collaboration but resources need to be brought to bear to make this a reality. The promise of FBO involvement in both preventing and caring for those with HIV is in their unique ability to promote HIV prevention, testing, and treatment without stigma; to encourage sexual behavior that lessens the possibility of infection; and to provide spiritual and tangible support. Health and development professionals need to foster FBO involvement in health programs, providing education and support to FBO leaders and members, to achieve this promise.
Footnotes
Acknowledgements
The authors wish to express their gratitude to the following Malawi members of the research team for their thoughtful guidance and generous assistance in completing the research: Alice Bvumbwe, Andrew Mguntha, Joel Phiri, Sheikh Mussah Ayami. The project would not have been successful without them.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received a R01 (R01 HD050147) from the National Institute of Child Health and Development (NICHD). The fourth author received a Research Supplement to Promote Diversity in Health-Related Research, also from NICHD.