
Abstract
We examined the meaning of living with HIV/AIDS among women in Lebanon. Ten women living with HIV/AIDS (WLWHA) described their experiences via semistructured in-depth interviews. They navigated a process of HIV diagnosis acceptance that incorporated six overlapping elements: receiving the news, accessing care, starting treatment, navigating disclosure decisions, negotiating stigma, and maintaining stability. Through these elements, we provide a framework for understanding three major themes that were constructed during data analysis: Stand by my side: Decisions of disclosure; Being “sick” and feeling “normal”: Interacting with self, others, and society; and Living day by day: focusing on the present. We contribute to the existing literature by providing a theoretical framework for understanding the process of diagnosis and sero-status acceptance among WLWHA. This was the first study of its kind to examine the meaning of living with HIV/AIDS among women in a Middle Eastern country.
Keywords
Although HIV/AIDS prevalence rates are relatively low in the Middle East and North Africa (MENA) compared with other regions, the known rates in MENA are likely underestimated because of the lack of coverage or presence of surveillance (Jenkins & Robalino, 2003). An estimated 75,000 adults and children were newly infected with HIV in 2009 (Joint United Nations Programme on HIV/AIDS [UNAIDS], 2010) and 31,000 new infections reported in 2012 (UNAIDS, 2013). There has been a relative paucity of data available on HIV/AIDS in MENA compared with other regions of the world (McFarland et al., 2010). Denial that HIV/AIDS exists and is a problem in MENA persists in some countries (Abu-Raddad, Akala, et al., 2010). Although UNAIDS (2010) estimates that 460,000 individuals are currently living with HIV in MENA, the exact number of women living with HIV/AIDS (WLWHA) in the region is unknown. While other regions have successfully achieved declines in the incidence of HIV, the MENA region is one of the only regions globally still witnessing an increase in new infections (UNAIDS, 2013). In fact, reports provided by nongovernmental agencies and the National AIDS Program reveal a staggering 134% increase in the prevalence of HIV in the region (UNAIDS, 2013).
It is well established that women are physiologically at greater risk and susceptibility to HIV than men through penile-vaginal sex because of the cell receptors in the cervix (Quinn & Overbaugh, 2005). Moreover, women are also socially more vulnerable to HIV transmission. This is particularly the case in cultural contexts characterized by gender norms that promote men’s autonomy and women’s economic dependence on men (Harvey & Bird, 2004; Kim, Pronyk, Barnett, & Watts, 2008). These social and cultural factors can influence women in both developed and developing countries, but in regions characterized by poverty and a lack of equal rights for women, the risk of HIV infection is greatly intensified (Pronyk et al., 2008). UNAIDS (2006) has estimated that in most countries in MENA, women represent less than 25% of people living with HIV/AIDS (PLWHA); however, the overrepresentation among men has been shifting as the prevalence among women increases (Abu-Raddad, Hilmi, et al., 2010; Obermeyer, 2006).
To date, research efforts have largely overlooked Lebanon where the current HIV prevalence is 0.1% (UNAIDS, 2014) with an estimated total prevalence of 3,750 (Shaheen, 2014). Within a culturally and religiously conservative society, frank discussions about the sexual transmission of HIV are difficult (King-Irani, 1996). Although rates of infection are uncertain because of a lack of sufficient surveillance (Jenkins & Robalino, 2003; Obermeyer, 2006), recent statistics from the National AIDS Program in Lebanon suggest that 90% of infection was transmitted via sexual contact (National AIDS Program, 2013). The ratio of HIV-infected men to women in 1990 was 6:1; by 1998, the ratio had changed dramatically to 3.6:1 (Kalaajieh, 2000). While infections among women are underreported, the majority of women found to be infected between 1984 and 1998 were married (81.7%) and were presumed to be infected by their husbands (Kalaajieh, 2000; UNAIDS, 2013). Health care providers in Lebanon do not currently initiate testing of pregnant women, in part, because of the stigma that characterizes WLWHA (UNAIDS, 2013).
Without optimal adherence to drug regimens, PLWHA can develop resistance to one or more antiretroviral medications (ARVs; Levy, 2007). Adherence is ideal globally, but barriers to adherence are context- and culture-specific (Murray et al., 2009). Although ARVs have been free for Lebanese citizens since 1998, transportation challenges as well as disruptions in supply because of political conflicts can impede individual access (J. Mokhbat, personal communication, July 9, 2006). When introduced into the region, ARVs improved the quality of life of PLWHA and decreased mortality rates (Abu-Raddad, Akala, et al., 2010). Ensuring access to ARVs for all PLWHA in need of treatment, however, continues to be a problem in MENA (Abu-Raddad, Akala, et al., 2010).
Cultures characterized by women’s subordination to men make it difficult for women to access treatment when infected with HIV (Ehrhardt, Sawires, McGovern, Peacock, & Weston, 2009). In MENA, as in many regions of the world, women’s insufficient funds or lack of control over household earnings may limit their ability to access and maintain ARV medications (Remien et al., 2009). Prior to approximately 2008, typically men and married women who were testing positive for HIV in Lebanon (J. Mokhbat, personal communication, December 10, 2008). However, anecdotal evidence from the physician who treats many of the country’s HIV/AIDS patients indicated an increase in the number of unmarried women testing positive for HIV in Lebanon (J. Mokhbat, personal communication, December 10, 2008). Unmarried women face myriad obstacles when trying to access sexual health treatment and services, including testing for sexually transmitted infections. In MENA, married women who test positive for HIV are often compelled to remain married because of social and economic constraints and may be blamed for the infection by their husband’s family (Remien et al., 2009). Similarly, unmarried WLWHA in the region are expected to experience guilt about their sexual “misbehavior” (Remien et al., 2009). In the cultural context of defining sexual activity within the confines of marriage, both married and unmarried WLWHA have a unique set of experiences and perceptions that had not yet been comprehensively examined in Lebanon prior to the present study.
Previous quantitative research has measured associations between finding meaning in life following a positive HIV test and behavior that affects health and quality of life (Audet, Wagner, & Wallston, 2015; Buscher et al., 2013; Valle & Levy, 2008). Importantly, in one study, participants who found meaning in response to an HIV-related stressor had less rapid declines in CD4 T cell levels and lower rates of AIDS-related mortality (Bower, Kemeny, Taylor, & Fahey, 1998). Previous qualitative inquiry indicates that the construction of meaning following diagnosis affects self-perception, which in turn affects individuals’ adaptation (Fife, 2005). Specifically, construction of meaning can occur vis-à-vis the normalization of illness, the integration of HIV into personal identity, and the recognition of positive effects of HIV (Alexias, Savvakis, & Stratopoulou, 2016). What it means to live with HIV/AIDS has been described differently by women living in different contexts. For example, among WLWHA in San Francisco, participants described the meaning of testing positive as an epiphany (that clarified the meaning of life), a confirmation (that corroborated their suspicions of being HIV-positive), or a calamity (that caused deep distress, loss, and affliction; Stevens & Doerr, 1997). In Finland, WLWHA explained the meaning of living with HIV/AIDS as experiencing a shift of focus from planning for the future to living in the “here and now” (Kylmä, Vehviläinen-Julkunen, & Lähdevirta, 2001). The experience of living with HIV/AIDS is context-specific and to be understood must be examined in individual countries and/or regions (Doyal, 2009).
Although the lived experiences of WLWHA in Lebanon had not yet been examined, a recent study measured the quality of life of PLWHA in Lebanon (Abboud, Noureddine, Huijer, DeJong, & Mokhbat, 2010). The authors found that among 41 PLWHA surveyed, a lower perception of stigma was associated with higher quality of life. The factors most strongly associated with quality of life among PLWHA included social relationships, mental health, and medical care. The authors found no differences between women and men in regard to reports of stigma and symptoms; however, women reported better quality of life in the social functioning domain. Although they cautioned against drawing strong conclusions about gender differences because of the small proportion of women in the sample (22%), the authors suggested that women may have relied on socializing as a coping strategy more than men.
The purpose of the present study was to understand how women 1 living with HIV/AIDS in Lebanon view their sero-status and the ways in which women created meaning in their lives following their diagnosis. We sought to develop a framework that facilitates understanding of the process by which women created meaning in their lives during and after learning of their sero-positivity. This study was the first to examine what it means for women to live with HIV/AIDS in Lebanon.
Method
Data Collection and Analysis
Ten WLWHA participated in in-depth semistructured interviews in 2009 and 2010. Participating WLWHA comprised a convenience sample recruited by an HIV/AIDS specialist in Lebanon. At the time of data collection, there were an estimated 30 to 40 WLWHA who were in care in Lebanon. Of 18 WLWHA approached, 10 agreed to participate in the study described. Interviews with WLWHA took place in a private room and when possible, were scheduled for participant convenience to coincide with their regular appointments. Following the oral informed consent process, interviews with WLWHA were digitally audio-recorded given the participant’s consent (N = 2); if the participant was not comfortable being recorded, the interviewer typed notes verbatim during the interview (N = 8). Interviews were in Arabic or English and lasted from 60 to 120 minutes; interviews that took place in Arabic were translated in real-time into English by a local certified translator. Following basic demographic information intake, interviews followed the structure of an interview guide that included open-ended questions about the following general areas: life before and after testing positive, being tested for HIV, experiences with disclosure, changes in everyday life, and how the future looked. For the purposes of triangulation, 10 men living with HIV/AIDS and 10 community HIV stakeholders were interviewed; however, because of space constraints, the focus of this article is on the WLWHA.
Constructivist Grounded Theory (Charmaz, 2006) and Symbolic Interactionism (Charon, 2004) guided data collection and analysis. Transcripts were analyzed through the use of Atlas.ti and according to the constant comparative method to identify salient themes both within and across transcripts (Glaser & Strauss, 1967). Atlas.ti was used for data management and organization of codes and themes; relationships between themes were mapped out by hand. Commonalities and differences within and among participants’ experiences were identified and then organized according to theme. Qualitative analysis through the use of questioning the data, analyzing a word, phrase, or sentence, and further analyzing through comparisons (Strauss & Corbin, 1998) facilitated the process of identifying the most important ideas and themes both according to existing concepts of health and to the participants’ voices and experiences. Although coding was conducted by only one researcher (R.K.), scientific rigor was achieved through the use of the above methods of inquiry in addition to reviewing the findings of the study with two participants who confirmed that the data, framework, and themes accurately represented their lived experiences. Quotations in this article were selected for their representation of themes and concepts within the interviews. The Institutional Review Boards at the participating universities reviewed and approved the study prior to initiation of the data collection process.
Sample Description
The study sample was comprised of both unmarried and married WLWHA who were both Muslim and Christian. Although ultimate control over which WLWHA enrolled in the study was impossible, maximum variation (Lincoln & Guba, 1985) was still a sampling goal. Convenience sampling was used as the most pragmatic method with “hard to reach” populations (Abrams, 2010). Because Grounded Theory is the guiding methodology for the study, the exact sample size was not predetermined (Sandelowski, 1995). The number of WLWHA interviewed was 10; although it is difficult to determine whether saturation was achieved, a sample size of 10 is appropriate, given the local HIV prevalence and stigmatizing environment. Reportedly there were approximately 30 to 40 known WLWHA currently in care living in Lebanon during data collection (J. Mokhbat, personal communication, July 12, 2009 and October 22, 2010).
Findings
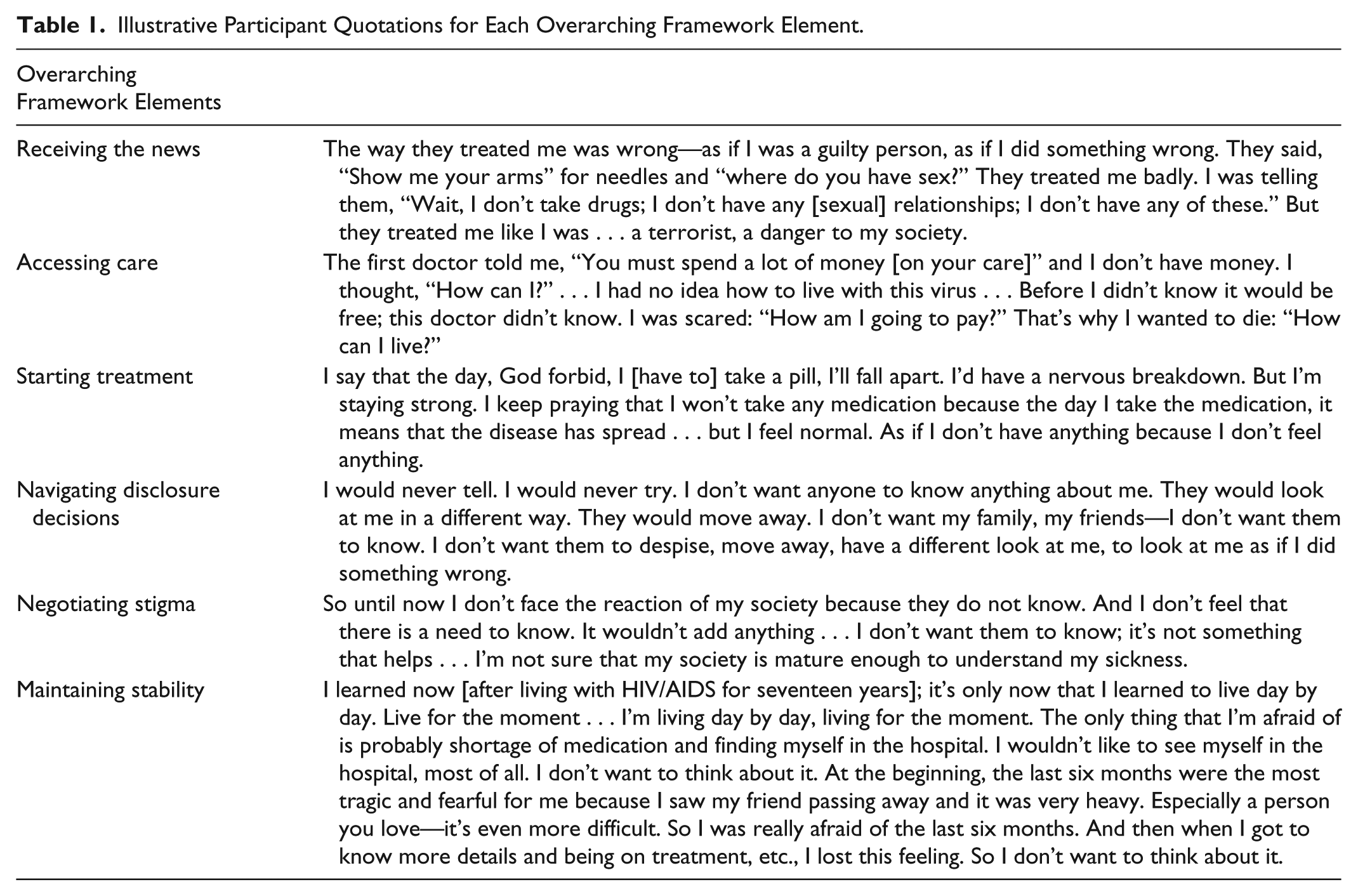
The meaning of living with HIV/AIDS for WLWHA in Lebanon can be described as the process of learning how to accept and live with the diagnosis. Women described testing positive for HIV as a major life-changing event and recognized the need to accept their HIV status. They went through a process of making meaning in their lives either because of or despite their sero-status. WLWHA in Lebanon began a process of accepting their diagnosis from the moment they learned about their HIV test results. The process is one that unfolds over time and is influenced by a confluence of factors that mitigate or exacerbate the impact of having a chronic illness and a culturally highly stigmatized condition. A combination of natural disease progression and contextual factors mark and define the acceptance process among WLWHA in Lebanon. Beginning with the manner that each woman intersected with the health care system when she tested positive for HIV to the way that she has evolved to think about and navigate her own future, learning how to live with HIV/AIDS is a process comprising the following elements: receiving the news, accessing care, starting treatment, navigating disclosure decisions, negotiating stigma, and maintaining stability. These elements represent nonsequential and nontemporal events that occur in a woman’s life following a positive HIV test. The elements are the major events that WLWHA confront and are often overlapping and continuous. Not all women in the sample had experienced each element, but the majority had or was aware that she would. For example, some women had yet to start on ARV treatment, but they had accessed care. Some women had not yet been able to find stability in their lives. Overall, however, these elements provide an overarching framework to view, describe, and explain women’s experiences of living with HIV/AIDS in Lebanese culture. Table 1 provides illustrative quotations of participants’ lived experiences relevant to each of the following overarching framework elements.
Illustrative Participant Quotations for Each Overarching Framework Element.
Overarching Framework Elements
Receiving the news
The experience of testing positive for HIV was an extremely difficult and pivotal time for women. None of the women were tested at a Voluntary Counseling and Testing (VCT) center where staff members are trained by Lebanon’s National AIDS Program, and recognized by the Ministry of Health to provide pre- and post-test counseling. As such, general health care staff members gave the women their results; these providers were unlikely to be trained about the importance of how to give HIV-positive test results in a way that decreases the negative impact of the news on the newly diagnosed person. Likewise, health care staff members who are unfamiliar with the HIV/AIDS-related services, treatment modalities, and resources in Lebanon are less equipped to provide referral, treatment, and service information at this critical stage. In two cases, women’s test results were communicated indirectly to them through a relative. Two women in the sample were tested for HIV outside of Lebanon and were deported back to Lebanon as a result. One of these women did not receive her results until she had landed in Lebanon. The other woman was required to remain at a hospital within MENA after she had tested positive and while undergoing confirmatory tests. She was then told to leave the country within 48 hours; she left her job, her bank account, and all her belongings and was unable to return as her passport was stamped barring reentry. Women who were tested in Lebanon had a variety of experiences when receiving their test results.
Accessing care
Women described having little knowledge of HIV/AIDS prior to testing positive. Perhaps because they did not test for HIV at VCT centers where the referral system is formalized, they had diverse experiences with receiving referrals for and accessing HIV/AIDS care. One participant was fortunate enough to be tested at a laboratory that was familiar with one of the few HIV specialists who treats patients in Lebanon, and as such, they provided her with referral information. In a very different scenario, the testing physician informed a participant that she should go to the HIV specialist but that the care and treatment were very expensive; the physician failed to inform her that the Lebanese Ministry of Health provides the medication free of charge and that resources exist to assist with the cost of the necessary CD4 and viral load blood tests. Women relied on interactions with their HIV specialists for gaining information and learning how to live with the diagnosis. Some of the women were initially very anxious and worried about every change they noticed in their bodies and they recalled contacting their specialist on a regular basis to ask about “every little thing.”
Starting treatment
WLWHA often viewed being told that they needed to start taking medication for HIV as horrible news that was almost as bad as testing positive for HIV. Coming to an awareness of the need to begin ARV treatment represented a key element and a major turning point in the process of acceptance. This, participants explained, is because taking medication can be one of the few daily reminders of being “sick” regardless of the presence or absence of symptoms. If clinical recommendations had not yet indicated the need to start taking medication, women anticipated this day with dread and anxiety. For example, women worried about having a “nervous breakdown” because starting medication means to them that the body is not strong enough to fight the virus on its own. Contrary to the popular stereotype that Lebanon is a “pill-popping” country, in part because of easy access to medications through pharmacies, most WLWHA felt a heavy burden because of the need to take ARV medication.
Navigating disclosure decisions
Because of the life-changing implications of receiving a positive HIV test, newly diagnosed individuals must navigate the decision-making process about whether, how, when, and to whom to disclose their status. The process of making decisions regarding disclosure constitutes major events in the lives of WLWHA as they accept their diagnosis and the changes that HIV brings to their lives. This element, unlike those previously described, involved decisions that included other individuals outside the more private dyad of the woman and her physician. All of the women interviewed believed that public disclosure would lead to negative social appraisal, regardless of how they had become infected. They described varying degrees of discomfort about societal views of PLWHA and particularly of WLWHA, from hoping for change and acceptance to feeling undisturbed by societal views because others are unaware of their status. Some women explained that before testing positive, they had very little or incorrect information about HIV and transmission and that because of this lack of prior knowledge, they understood the fear and rejection they expected or experienced from others.
Negotiating stigma
Women began to encounter HIV/AIDS-related stigma from the moment they received their positive test result. Stigma not only affected disclosure decision-making but it also affected women’s overall process of diagnosis acceptance. Whether women had minimal information about HIV prior to testing positive or felt that they had some level of understanding, they knew from the beginning that their status carried stigma. Women referred to the general public as not accepting and anticipated that if others knew about their status, they would experience fear, rejection, repulsion, and withdrawal by others. When a diagnosis is stigmatized, women must overcome the disease-related stigma to gain support from others. Only one of the women had accessed formal HIV-related psychosocial services at the time of the interview.
Maintaining stability
Women’s quest to achieve a sense of stability in their lives was an important component of the larger process of acceptance. Once they began to take the right medication, if clinically appropriate, and had adjusted to the side effects, most women preferred not to think about their status. They were obliged to think about their diagnosis during regular check-ups and some viewed taking daily medication as a constant reminder of the presence of HIV in their lives. Once the women obtained stability in managing their status in terms of treatment and care, they tended to focus on other things in their lives and described this as “getting on with life” or “moving on.” The amount of time that had passed since diagnosis did not act as a blanket barometer for how well women accepted and learned to live with their diagnosis. For example, one woman had tested positive a year and a half prior to the interview, had accepted her status, and was functioning fairly well. On the other hand, another participant had tested positive 16 years prior but expressed continued difficulty accepting her sero-status when interviewed. Other women described an acceptance process that typically took 1 to 2 years and included stages such as shock, denial, depression, acceptance, and moving on. Women expressed their ability to accept and move on by describing their focus on the present and living “day by day.”
Women moved through these six elements in the process of accepting their sero-status and creating meaning in their lives either because of or despite their diagnosis. Women’s experiences with receiving the news, accessing care, and starting treatment all influenced the women’s ability to accept the impact of HIV/AIDS on their lives. Likewise, navigating disclosure decisions, negotiating stigma, and maintaining stability are essential parts of the process of acceptance. Women’s navigation of the six aforementioned overarching framework elements is best understood through an examination of three main themes that emerged and were constructed during data analysis. The following three main themes further explain women’s processes of acceptance and creation of meaning: Stand by my side: Decisions of disclosure; Being “sick” and feeling “normal”: Interacting with the self, others, and society; and Living day by day: Focusing on the present. While all six of the overarching framework elements are key to understanding the process and experience of women in Lebanon following a positive HIV test, these three main themes were most central to women’s lived experiences. The three major themes are linked to the last four overarching elements and represent the way in which women perceive their lives within the context of their sero-status.
Main Themes
The first major theme, “Stand by my side: decisions of disclosure” is linked to the navigation of disclosure decisions. The second major theme, “Being ‘sick’ and feeling ‘normal’: interacting with self, others, and society” is linked to negotiating stigma with the self, from others, and from the general public as well as to starting treatment. The third major theme, “Living day by day: focusing on the present” is linked to the process of acceptance when women strive for maintaining stability and reflects the way in which women made new meanings in their everyday lives.
Stand by my side: Decisions of disclosure
WLWHA in Lebanon faced a complex set of decisions involved in disclosure throughout their acceptance process. The need to have someone stand by their side was a major motivating factor that influenced decisions. Although women disclosed or considered disclosing their status immediately on receiving their test results, decisions about disclosure continued during multiple elements of acceptance and disease progression by weighing relevant factors, anticipating the impact of the decision, and experiencing disclosure or nondisclosure and the resulting consequences. As they weighed the factors and anticipated the other person’s reaction, women hoped for positive consequences that would bolster their support and protect the health of others.
Weighing relevant factors
As an integral part of the decision-making process, women considered important factors about to whom and how they might disclose. One important factor was a sense of obligation to disclose based on the perception of safety or fairness. Some felt the need to disclose to family members for whom they cooked, as one woman explained, “My godson knows, of course, he’s living with me. He’s eating from my cooking, so it’s only right; it’s fair.” One young participant revealed her reasoning for disclosure to her cousin to whom she was very close, “She used to come and sleep over a lot. Sometimes she uses my toothbrush, my everything. It was a combination of things [that led me to disclose to her]. I needed to wake her up: Life is not as clean as we think.” Women also cited the perception of a medical necessity as a relevant factor in deciding about disclosure. Women discussed the need for someone to know their status in the event of a medical emergency and viewed this as a relevant factor in the internal process of decision. Another important factor relevant for women was the anticipation of acceptance from the individual. One woman noted waiting to disclose to her daughter until she was old and mature enough to receive and accept the news.
The need for emotional support was the most important factor in influencing women’s decisions to disclose. A common phrase that was repeated throughout women’s narratives was women expressing their need for someone to “stand by my side.” WLWHA expressed the need for someone to be there for them for emotional support and for someone who would not judge them. One participant had been diagnosed 15 years prior to revealing her status to her sister and nieces and explained that a change in her health catalyzed her disclosure decision. Other relevant factors that women weighed included concerns about reactions from others. Women were worried that people would avoid them and not want to speak to them. They were also concerned about causing fear toward them and their children and about coming to their homes and eating with them. Women worried about others viewing them differently if they disclosed their HIV status.
Anticipating disclosure impact
During the decision-making process, women considered the impact that disclosure might have on them, on the other person, and on their lives. This step included imagining and anticipating the individual’s reaction and preparing for the disclosure experience as well as the resulting actual reaction of the individual. WLWHA anticipated the specific impact of these decisions on both themselves and the person receiving the information. They also incorporated their past experiences with and assumptions about HIV/AIDS into their anticipation of the disclosure impact.
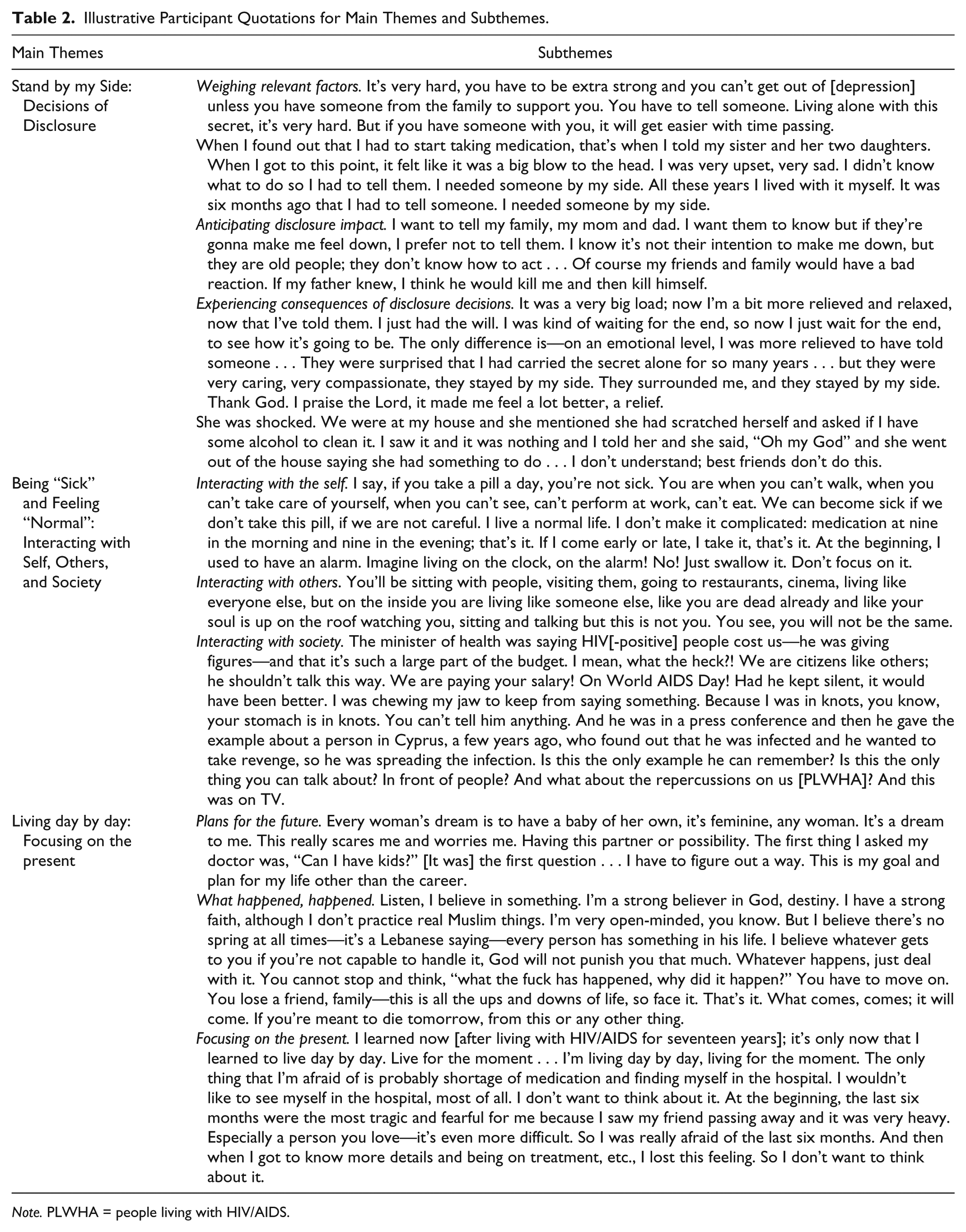
Some women expressed conflicting emotions when explaining their desire to disclose compared with the anticipated impact of the information. Many participants decided against disclosing because of a negative anticipated experience resulting from disclosure. One participant, who was unmarried at the time of the interview, described some particularly extreme and negative reactions she anticipated if she were to disclose her sero-status to her family: “Of course my friends and family would have a bad reaction. If my father knew, I think he would kill me and then kill himself” (see Table 2). The fear of the impact a disclosure would have on the family illustrates the immense pressure that WLWHA experience. On the other hand, some women prioritized the potential support they might gain from their loved ones and decided to disclose to their families despite the possibility of negative impact. Each woman delineated the potential anticipated impact that disclosure could result in during this step in her decision-making process.
Illustrative Participant Quotations for Main Themes and Subthemes.
Note. PLWHA = people living with HIV/AIDS.
Experiencing consequences of disclosure decisions
Women experienced a broad range of responses to and consequences of their disclosure decisions, which affected their relationships with others and in turn their social, emotional, and logistical support. Some women gained the support they were seeking that motivated them to disclose, while others were met with negative responses and painful rejection. Women’s experiences with disclosure to one person also affected subsequent disclosure decision-making processes.
Some WLWHA described positive reactions of others when they disclosed their sero-status. One participant described her mother’s care and concern for her and the added effort her mother made to show her that she was not afraid: “It was the nicest thing ever . . . My mom woke me up. She made me this healthy food. She ate with me from my plate for me not to feel rejected.” Another woman found comfort and relief after disclosing to multiple friends and described them as “really very positive.” Another participant had become infected with HIV while working abroad as a domestic worker, an undesirable job for Lebanese women. She explained that she had been infected by HIV when her employer raped her. Because of these layers of stigma, she had not disclosed her sero-status to anyone for 15 years. The participant described her experience as unburdening herself when she decided to disclose her HIV status to her family.
Other women in the sample experienced negative reactions following disclosure. They explained that their news was met with fear, a lack of understanding, and judgment. People’s fear, many women explained, was because of a lack of information about the modes of transmission of HIV. The women interviewed decided both for and against disclosure at different times. Nondisclosure allowed many WLWHA to feel at ease because most people around them did not know their status, while others felt the weight of the burden of maintaining the secret as a means of preserving their own and their family’s privacy. As women move through the process of accepting their sero-status, they face the emotional and logistical need for someone to stand by them. Thus, women weigh the factors, anticipate the impact, and experience the consequences of their disclosure decisions.
Being “sick” and feeling “normal”: Interacting with self, others, and society
As women navigated the process of accepting their diagnosis and learning how to live with HIV/AIDS, they experienced many changes in their lives based on perceptions of HIV/AIDS from within themselves, from others, and from society. Regardless of women’s levels of knowledge prior to testing positive for HIV, they were aware of the publically negative view of PLWHA that became personally relevant on receiving the diagnosis. As women contended with negative societal and personal messages about PLWHA, leading a “normal” life became essential for their ability to manage their overall health and well-being. Natural disease progression, knowledge about HIV/AIDS, as well as other factors in the environment affected women’s perceptions of their health. The perception of themselves as being “sick” or feeling “normal” emerged as a central theme in the overall process of living with HIV/AIDS. Their interactions with the self, others, and society demonstrate the ways in which women navigated the stigma associated with their HIV status.
Interacting with the self
After being diagnosed with a chronic condition, women face a multitude of changes in their everyday lives. In addition, when that condition is highly stigmatized, women face the possibility of changes in their self-perceptions. Women in the study tended to experience a range of emotions and thoughts about why they contracted HIV and whether there was someone to blame for the infection. Women’s experiences largely did not include the internalization of stigma, or the acceptance of HIV stigma as legitimate and applicable to themselves (Steward et al., 2008). Rather, their construction of meaning about their infection narrated a story of self-preservation and self-acceptance. Women dealt with anger, blame, and confusion, and were confronted with the stigma associated with being diagnosed with a highly stigmatized condition within a highly stigmatizing environment. Despite the local societal expectation for unmarried women to feel more stigmatized than married women as well as the assumption that WLWHA had engaged in sex work, WLWHA worked to resist the internalization of stigmatizing messages. One participant explained how she did this: “I live a normal life. I don’t make it complicated: medication at nine in the morning and nine in the evening; that’s it” (see Table 2).
Interacting with others
In addition to the direct immediate reactions that women faced from individuals to whom they disclosed their HIV status, they also navigated other ongoing interactions over time with people who were both aware and unaware of their status. Overall, women balanced the internal knowledge about their status with both the external views of PLWHA and the assumption that they were not HIV-positive; many WLWHA shared the common experience of feeling as if they are living a double life. This tension was described: “I always feel uncomfortable; I have this fear. I mean, I do live a normal life, as if I didn’t even have the virus. That’s because nobody knows at all.” Women balanced the worry about their status being discovered with their ability to live a “normal” life. Their concerns about ongoing social interactions focused on relationships with family members, potential intimate partners, neighbors, and health care professionals and service providers.
Interacting with society
Women’s perceptions of being “sick” and feeling “normal” were also affected at the societal level. Messages about PLWHA came from Lebanese society, as defined by the women as being made up of individuals and groups beyond their families, neighbors, and communities that are part of the greater general public. Women were aware of this societal stigma and felt that it affected their lives and in particular their ability to feel “normal.” Media coverage of HIV/AIDS can also have a negative impact, rather than alleviating or reducing society-level stigma. One woman described seeing PLWHA in Lebanon participating in a TV interview. She explained that the PLWHA sit behind a screen and have their voices changed and speculated that this was because of the fact that the public views HIV transmission as being related to sex, sex work, drugs, being gay, and other socially or legally restricted behaviors and identities. Women’s interactions with self, others, and society have a direct impact on their ability to feel “normal” and deal with perceptions of being “sick.” The stigma that they experience at different levels can threaten their ability to live a “normal” life, which they define as attending to their regular responsibilities and activities. Lebanese cultural and societal expectations for women, such as not having sex before or outside marriage and social value being tied to status as a wife and mother (El Feki, 2013), translate into high levels of stigma toward WLWHA.
Living day by day: Focusing on the present
Having future plans and goals seemed to reflect women’s ability to accept the news of their diagnosis, integrate it into their circumstances, and move forward with a new sense of meaning in their lives. However, regardless of whether they had some conceptualization of a positive future, women navigated everyday life by means of a sharp focus on the present. Whether choosing to avoid thinking about the past and future from a perspective of fear or strength (“what happened, happened”), women were able to function in their environments through a prioritization and focus on “living day by day.” Common among individuals with chronic health conditions (Charmaz, 1991), “living day by day” is a shared experience among WLWHA.
Plans for the future
Women’s ability to plan for the future seemed to indicate acceptance of their diagnosis. Although women’s focus was primarily on “living day by day,” women who were able to verbalize specific concrete hopes about the future appeared to experience stability in their lives. In regard to the future, women spoke about the meaning that children and motherhood would bring to their lives. They talked about the fears associated with not being able to have children if they had not given birth prediagnosis and were in their reproductive years (n = 2) and discussed the relief they felt if they had had children before becoming aware of their HIV infection (n = 7). Two women wondered how they would find meaning in life if their sero-status prevented them from having children: “The future? I’m scared because of one thing. I’m still young. I’m still strong. But what will tomorrow bring me if I don’t have a family of my own?” Moreover, despite the Lebanese expectation of children caring for elderly parents when they are no longer able to take of themselves, the desire to have children was not motivated by this concern. Having children was directly tied to deriving meaning in life for almost every WLWHA in the sample.
Women were also concerned about disease progression. The fear and worry experienced was typically associated with the perception of knowing that HIV/AIDS would one day bring death and therefore dwelling on the future was undesirable. One woman had lost a friend to AIDS and expressed her lack of desire to see a WLWHA at the end of her life because it would feel as if she was watching herself die. Similarly, another woman feared what tomorrow would bring, so she preferred not to ask too many questions about her health for fear of the answers. Women also worried about logistical concerns of daily life in Lebanon. Women who were employed at the time of the interview worried about losing their jobs if their status became exposed and/or about being required to take an HIV test for a new position. They were also concerned about medication supply shortages, both in general and because of political conflict; the need to carry medication as well as have an extra emergency back-up supply was viewed as a burden among women on ARV treatment. Women described the constant fear of their status being exposed at the societal level as well as the eventual need for medical care and hospitalization when they would become “really sick.” Overall, women minimized their thinking about and planning for the future, and instead chose to focus on the present by living “day by day.”
What happened, happened
Women’s descriptions of contracting HIV/AIDS by using the phrase, “what happened, happened,” indicated resignation that allowed for acceptance of their sero-status and for a focus on the present by letting go of the past. Similar to their views of the future, they expressed the lack of desire to dwell on the past and instead focus on the ability to accept the events in their lives. When reflecting on becoming infected with HIV/AIDS, many women described being less worried about the small concerns in life and being more attuned to the needs of others and the “bigger picture” issues such as others’ suffering and contributing positively to other people’s lives. Many women described themselves as less superficial because of having to face a life-threatening diagnosis; one woman explained that she wished she could have changed her character and gained the depth she did without having to go through the difficult experience of testing positive and living with HIV/AIDS. Rather than blame her late husband for infecting her, one woman expressed this concept of acceptance and moving on: “My husband loved us. I don’t think he wanted me to get HIV. He was ashamed to talk about it. Well, it happened. We can’t change it. I wanted to go ahead with my life.” Others referred to the role of religion in their process of letting go of the past.
Focusing on the present
Accepting what happened in the past and making plans for the future were parts of a larger process of integrating a diagnosis of HIV/AIDS into women’s lives. However, these processes faded into the background of their lives as they focused on the present; living “day by day” became forefront. Many women described the past as painful and this was largely the motivator for focusing on the present and living “day by day.” They faced high levels of stigma that they had to overcome to focus on the present and live their lives in a way that was manageable for them. Women typically thought about the past and future minimally and focused on everyday life as a means of accepting their sero-status and embracing normalcy. One woman explained: “It’s only now that I learned to live day by day. Live for the moment . . . I’m living day by day, living for the moment . . . I don’t want to think about [my health deteriorating]” (see Table 2). For WLWHA in Lebanon, living day by day is an important part of the narration of their lived experiences about what it means to live with HIV/AIDS. Their focus on living in the present is likely influenced by the nature of living with a chronic condition. Focusing on the present and living day by day represent an integral part of women’s acceptance process and the way in which they create meaning in their lives.
Discussion and Conclusion
For women in Lebanon, making meaning of living with HIV/AIDS was a dynamic process that begins with an extremely difficult diagnosis event and then required coping strategies according to disease progression and personal context. For the women in the study, being HIV-positive was part of a daily experience, but because of the choices they had made and their efforts to accept their status and create new meaning in their lives, living with HIV/AIDS at times felt like other chronic and less stigmatized conditions. Obtaining the emotional support they needed introduced the risk of exposure to stigma and rejection. For WLWHA, starting ARV medication meant that the body was not strong enough to fight the virus on its own. Taking medication and seeing an HIV specialist regularly were constant reminders that threatened women’s ability to feel “normal.” Being infected with HIV meant that opportunities for future intimate relationships and childbearing were much more challenging, but not impossible. WLWHA used different strategies for obtaining the emotional support they needed, navigating stigmatizing messages, negotiating disclosure decisions, and maintaining stability within the context of a life that had new meaning because of the diagnosis. As WLWHA learned how to live with HIV/AIDS, they created new meanings in their lives by working through some or all of the overarching elements in the process of acceptance.
Women’s experiences are situated within a contextual environment of factors that affected the way they coped with being HIV-positive in Lebanon. Factors such as economics, culture, religion, and gender norms influenced WLWHA’s self-perceptions as well as their quality of life. For some women, being diagnosed with HIV/AIDS threatened their financial stability because of job loss, loss of spouse, or the need to purchase ARV medication when supplies are disrupted. Within a culture that values strong familial bonds (Lipson & Meleis, 1983), women experienced a great deal of inner conflict about their relationships with family members about whether to disclose, how to gain support, how to prevent transmission, and how to avoid being a burden. However, cultural norms often facilitated the financial and emotional support of unmarried and widowed women within the family structure when financial or medical circumstances necessitated assistance. Some women found strength and comfort in their faith and/or religion, as PLWHA have found in other contexts (Cotton et al., 2006; Plattner & Meiring, 2006; Tuck & Thinganjana, 2007), and described this source of comfort as a personal experience rather than something they shared with their religious communities. Gender norms affected women’s concerns about their ability to attend to household duties safely and effectively, as has been found in other settings (Harrison, Short, & Tuoane-Nkhasi, 2014). In addition, gender norms also influenced WLWHA’s opportunities for intimate partnership and created an intensification of perceived or actual stigma.
The present study contributes to the literature by providing a theoretical framework for understanding the process of diagnosis and sero-status acceptance among WLWHA. It also contributes greater understanding through theory development about the experiences of WLWHA; this understanding can be used for service delivery implications, policy recommendations, effective interventions, and resources (Herzlich & Pierret, 1987; Sandelowski, Lambe, & Barroso, 2004; Zhou, 2008). Grounded in the data, the theoretical framework can be used to understand the process that WLWHA go through to accept their sero-status and to create new meaning in their lives that have been changed because of HIV infection. In Lebanon, women’s process of acceptance comprised some or all of the six elements in the overarching framework. Each woman received the news of her infection as a major life event. Women’s experiences with receiving the news and accessing care were influenced by their particular circumstances as well as structural and cultural factors in the Lebanese context. Starting ARV treatment was another major event that women experienced or anticipated as a difficult hurdle in the process of creating new meaning in life. Women’s experiences with stigma influenced both their ability to view themselves and their lives as “normal” and their rational decisions about disclosure. Finally, WLWHA’s focus on the present reflected their desire to find and maintain stability, as defined by their situations, perceptions, and experiences with the changes caused by being HIV-positive.
This study’s three major themes reflect both the individual and social impact of HIV/AIDS on WLWHA. The first major theme, Stand by My Side: Decisions of Disclosure, highlights women’s need for social and emotional support outside their relationships with their physician(s). Their need for this type of support motivated WLWHA to make decisions about disclosure in the hopes of gaining positive reactions and having someone stand by them. They risked rejection, shame, blame, fear, and withdrawal, among other potential consequences, when they made decisions that compromised their ability to maintain privacy about sero-status, but facilitated the possibility of gaining necessary support. The second major theme, Being “Sick” and Feeling “Normal”: Interacting With Self, Others, and Society, reflects an internal process among WLWHA that is influenced by factors in their physical and social environment. External messages about HIV/AIDS affected women’s individual awareness of being HIV-positive and the meaning of living with HIV/AIDS. Their social interactions with others either helped to mitigate or to magnify the adverse effects of stigma. Women emphasized their desire to avoid the view, from both themselves and others, of being “sick.” Their desire to feel “normal” motivated their choices about disclosure, among other life decisions. The third major theme, Living Day by Day: Focusing on the Present, indicates the way that WLWHA pursue, achieve, and maintain stability by minimizing reflections on the past and future. These three major thematic constructs contribute to our theoretical understanding of the lived experiences of WLWHA as they adjust to and create new meaning about their lives.
The meaning of living with HIV/AIDS for women in Lebanon is similar in some ways to that of PLWHA in other contexts. Women in the present study who seemed to be coping well appeared to have accepted their sero-status and described themselves as functioning, attending to their responsibilities, and living a “normal” life. Similarly, for WLWHA in Massachusetts and California, shifting the meaning of HIV/AIDS from negative to positive was linked to desirable outcomes such as ARV adherence, better mental health, and stress reduction (Bova, Burwick, & Quinones, 2008; Westling, Garcia, & Mann, 2007). Similar to WLWHA in the United States who used spirituality and religion as a coping strategy (Cotton et al., 2006; Tuck & Thinganjana, 2007), some WLWHA in Lebanon identified their faith as a source of comfort and as motivation to let go of the past. Women’s faith, however, did not emerge as a major theme in the research and was present in only a few of the women’s experiences. WLWHA in Lebanon, similar to individuals in Kenya (Curran et al., 2014), viewed ARV initiation with dread and indicative of poor health.
The meaning of living with HIV/AIDS for women in Lebanon also differed from the experiences of PLWHA in other contexts. Finding meaning among WLWHA in the United States has been described as “the movement through fears of death while finding meaning in living” (Leenerts & Magilvy, 2000, p. 62). For the women in the present study, however, finding meaning was unrelated to facing the possibility of dying because of complications related to HIV/AIDS. WLWHA in this study resisted thoughts about death and becoming “sick”; the meaning they created in their lives centered on living in the present without dwelling on or dealing with death or the future. Whereas WLWHA in Finland experienced a shift in their focus from planning for the future to living in the “here and now” because of their diagnosis (Kylmä, Vehviläinen-Julkunen, & Lähdevirta, 2001), WLWHA in Lebanon focused on the present in an effort to find meaning in daily life and to cope with the changes caused by living with HIV/AIDS. The meaning in their lives was derived from a focus on the present that enabled them to find a sense of stability and control. Conversely, PLWHA in Namibia obtained a sense of control, purpose, and meaning through the perception of personal deservedness of HIV infection. Unlike WLWHA in Lebanon, PLWHA in Namibia viewed HIV infection as a punishment from God and themselves as worthy of blame (Plattner & Meiring, 2006).
This study contributes to the existing literature by providing a theoretical framework for understanding the process of diagnosis and sero-status acceptance among WLWHA. The meaning of HIV/AIDS in the lives of women in Lebanon is influenced by contextual factors including economics, culture, collectivism, religion, and gender norms. For WLWHA in Lebanon, HIV infection means a daily awareness that influences everyday life. In the process of accepting their sero-status and creating new meaning, women learn to navigate the challenges that HIV/AIDS poses and to view themselves and their lives as “normal.”
Footnotes
Acknowledgements
We thank the HIV community of researchers and service providers in Lebanon. In addition, we would like to acknowledge Joelle Hatem and Hassan Cherry. This project is dedicated to the individuals who bravely shared the stories of their lives with us.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received grants from the following sources: UCLA AIDS Institute/Center for AIDS Research Grant number AI28697, the UCLA Graduate Division, and the TZ Chapter of the Philanthropic Educational Organization.