
Abstract
The increasing recognition of adverse childhood experiences as a significant factor in adult health outcomes underscores the need for trauma-informed care (TIC) in healthcare settings. The purpose of this study was to assess the psychometric properties of the TIC Provider Assessment Tool (TIC-PAT) designed for primary care providers. The TIC-PAT aligns with the TIC Pyramid framework and assesses both universal trauma precautions and trauma-specific care. A total of 176 primary care providers in the United States completed the TIC-PAT through an anonymous online survey. Findings through exploratory and confirmatory factor analyses revealed a unidimensional (one-factor) model, consolidating questions into a concise 10-item measure. This study contributes an efficient assessment tool for the provision of TIC by primary care providers in healthcare settings, promoting better patient–provider interactions and enhancing provider awareness of trauma's impact on health.
Introduction
The prevalence of individuals experiencing traumatic events during their lifetime is evidenced by a recent metaanalysis of 206 studies, revealing that over 60% have experienced adverse childhood experiences (ACEs). 1 The ACE Study in the late 1990s underscored the long-term impact, linking childhood trauma to increased risk of mortality from chronic diseases in adulthood. 2 This exposure leads to chronic stress and health issues commonly encountered by primary care providers. 3 To address this, healthcare organizations must adopt trauma-informed care (TIC) practices, particularly among lower-income communities with a higher prevalence of ACEs 4 so health equity might be realized. 5 Evaluating TIC provision is crucial for ensuring patient-centered, high-quality healthcare that respects the unique needs of patients and physicians.
While few validated instruments exist for assessing the provision of TIC, King et al 6 validated a 21-item tool, Baker et al 7 (2018) developed and validated the Attitudes Related to Trauma-Informed Care Scale (ARTIC), and Kokokyi et al 8 developed the 29-item Physician TIC Survey. However, no study has introduced a unidimensional short form specifically assessing provider practices within the TIC pyramid framework. 9 A tool concentrating solely on TIC practices could seamlessly integrate into current healthcare assessment protocols, lessening the time demand and cognitive strain on busy providers.
Conceptual Framework
The TIC Pyramid 9 was developed in response to the absence of a unified approach in applying TIC within healthcare settings. It draws on an extensive review of TIC literature, which highlighted two fundamental domains of practice: universal trauma precautions and trauma-specific care (see Figure 1). Universal trauma precautions are further divided into 2 categories—patient-centered communication and care and understanding the health effects of trauma. Patient-centered communication and care provide the foundation of the framework (Level 1) and refer to provider communication and behavioral strategies for helping patients with a trauma history better connect with healthcare providers without screening the patient for trauma history. Understanding the health effects of trauma is Level 2 of the pyramid and refers to the provider's understanding of the impact of trauma on the health of patients including maladaptive coping behaviors—also without screening the patient for trauma history.

The trauma-informed care pyramid. *Universal trauma precautions; **trauma-specific care.
Trauma-specific care in the framework builds on universal trauma precautions and is divided into 3 categories—interprofessional collaboration, understanding providers’ own history and reactions to trauma, and screening. Interprofessional collaboration is Level 3 and refers to the extent to which providers are aware of professionals in other specialty areas to whom referrals could be made to assist patients who disclose a trauma history. Understanding providers’ history and reactions to trauma is Level 4 and refers to the extent to which providers can recognize how their own life experiences may influence their ability to provide TIC to their patients. In addition, it refers to the potential for vicarious victimization or the experience of having emotional reactions to patient trauma stories, which if left unchecked, could lead to burnout. Screening for patients’ trauma history is level five and top of the pyramid.
Purpose of the Study
The study aimed to assess the psychometric properties of the Trauma-Informed Care Provider Assessment Tool (TIC-PAT) among primary care physicians in the United States. The TIC-PAT was developed based on the TIC Pyramid, 9 and incorporates the 2 dimensions of universal trauma precautions and the 3 dimensions of trauma-specific care.
Methods
Sample and Procedures
The TIC-PAT was administered as an anonymous online survey through the Reaction Data platform (see: https://reactiondata.com/). Providers were recruited through email invitations. Participants gave their informed consent, and all processes adhered to ethical standards following approval by the institutional review board.
A total of 13,532 physicians were targeted through the Reaction Data sampling frame. Physicians were familiar with receiving pulse surveys from Reaction Data and worked in various settings including hospitals, private practices, community clinics, outpatient centers, surgical centers, urgent care centers, long-term care facilities, rehabilitation centers, and academic medical centers. Physicians not practicing primary care in one of these settings were excluded from the study. No incentives were used to encourage physicians to participate.
Instrument Development
The TIC-PAT was developed based on the five areas of the TIC Pyramid framework—patient-centered communication and care, health effects of trauma, interprofessional collaboration, understanding one's own personal history and reactions, and screening. The initial 20 questions were aligned with specific suggestions for TIC practice. 9 All items used a 5-point Likert scale. The initial instrument's content validity was verified through review by 1 expert in TIC and 2 primary care providers. These experts provided valuable feedback related to question framing, response options, and survey organization. The survey underwent a pilot test involving a small sample of primary care physicians before being administered to a larger group of primary care physicians. Subsequent data analysis involved the application of factor analysis.
Data Analysis
Data were cleaned and item distributions were examined in Stata 18. Exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were conducted in Mplus Version 7 using a structural equation modeling framework. EFA and CFA require one to consider both the theory and how well the data fit the model. 10 For the EFA, output was allowed for 1 to 5 factors based on having items in the five areas of the TIC pyramid framework—patient-centered communication and care, health effects of trauma, interprofessional collaboration, understanding one's personal history and reactions, and screening. Each factor structure was examined to ensure theoretical rationale and that at least 2 items were loaded on each factor. Items with factor loadings less than .30 or with cross-loadings on multiple factors greater than .30 were sequentially dropped.11,12 Following the EFA, CFA was conducted, again requiring factor loadings greater than .30. For the CFA, we also examined model fit, with a root mean square error of approximation (RMSEA) close to .06 and a comparative fit index (CFI) close to .90 indicating adequate fit. 13
All models were estimated using a robust weighted least square estimation. This estimator is appropriate for ordinal data. Missing data ranged between 1% and 32% across all TIC-PAT items. There was no difference in missingness based on race, gender, or age. To handle missing data, full information maximum likelihood (FIML) was used. The FIML calculates missing information like multiple imputations. 14
Results
The final sample of 176 primary care physicians practicing in the United States began the survey. A good model fit was observed through factor analysis which supports the notion that the sample size was sufficient for capturing meaningful patterns in the data.
Sample Description
Most participants (77%) reported their race as White or Caucasian, 8% reported Asian or Pacific Islander, 2% Black or African American, 4% multiracial or biracial, 1% as other, no respondents reported Native American or Alaskan Native, and 8% preferred not to answer. The median age group of respondents was 46 to 55 years of age (44% of the sample; 4% reported < 35 years, 23% 35-45 years, 22% 56-65 years, and 8% 66-75 years). Most of the sample reported their sex as male (67%).
Exploratory Factor Analysis
Model fit improved with more factors. However, in 4- and 5-factor models, some factors did not have at least 2 variables loading on them after removing items that cross-loaded on another factor. In 2- and 3-factor models, after dropping items with low loadings (below .30) and high cross-loadings on multiple factors, the resulting factors did not have a good conceptual framework rationale. As such, to retain theoretical integrity, a unidimensional model (1-factor) was identified.
For a unidimensional model, having 20 items was not deemed to be necessary. As such, 2 items from each of the five TIC Pyramid areas were retained with the highest factor loadings (see Table 1). This resulted in a 10-item factor. The EFA was then rerun with only these 10 items in a single factor. Factor loadings ranged from .38 to .77 (see Table 2). Cronbach's alpha for a 10-item factor was very good (α = .85).
Exploratory Factor Analysis Factor Loadings for a Unidimensional Model.
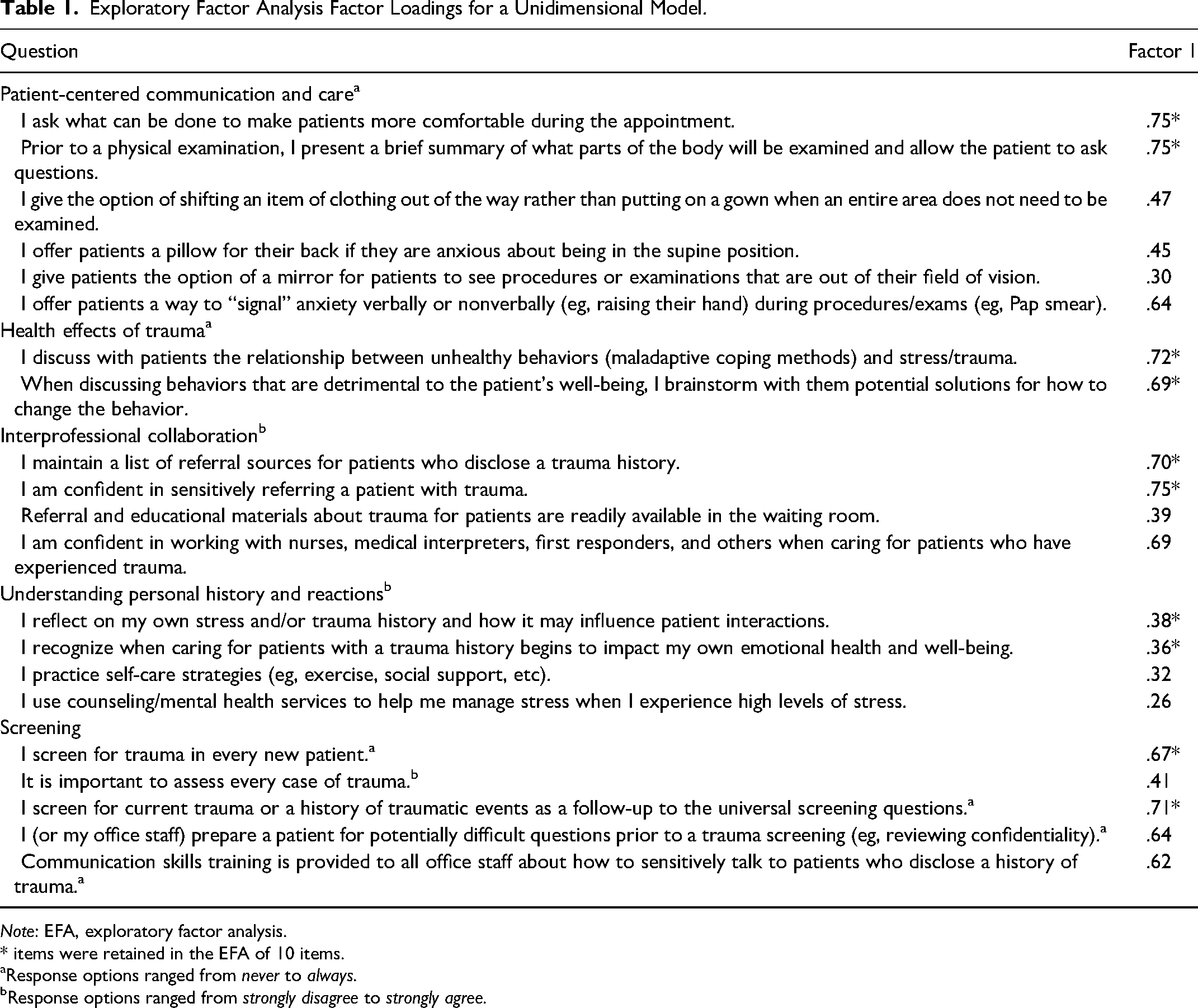
Note: EFA, exploratory factor analysis.
* items were retained in the EFA of 10 items.
Response options ranged from never to always.
Response options ranged from strongly disagree to strongly agree.
Exploratory Factor Analysis Factor Loadings for a 10-Item Unidimensional Model.

Note: RMSEA, root mean square error of approximation; CFI, comparative fit index.
Error terms were correlated between the two items in each of the 5 areas. Model fit: RMSEA = .051; CFI = .988.
Confirmatory Factor Analysis
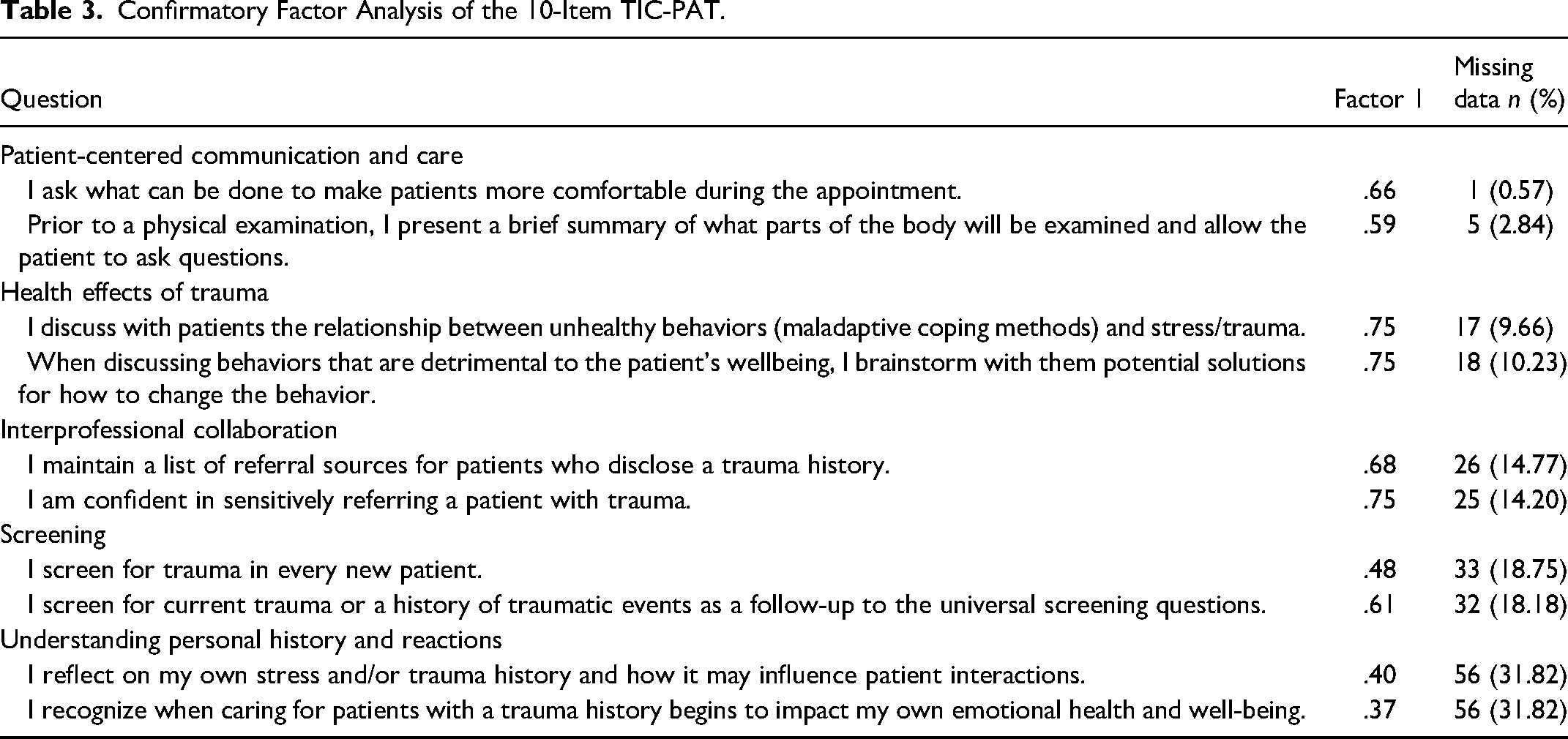
The need to correlate error terms between items from the same dimension was expected, but a CFA model was first fit without correlating error terms. As expected, the model fit for the initial CFA was below the model cutoffs. In SEM, decisions should be made when developing models that are based on theoretical justification. 15 As such, error terms were then correlated between the 2 items in each of the 5 dimensions. This resulted in a good model fit (CFI: = .988; RMSEA = .051). Factors loadings ranged from .37 to .75 (see Table 3). The 2 items from the “Understanding Personal History and Reactions” had the lowest loadings, but because they were above the minimum cutoff threshold determined a priori and because they were important parts theoretically to the model they were retained. There were no differences in TIC-PAT scores based on sex, race, or age group (results available upon request). Table 3 also includes the amount of missing data for each item.
Confirmatory Factor Analysis of the 10-Item TIC-PAT.
Discussion
The purpose of the study was to explore the psychometric properties of the TIC-PAT among a group of primary care physicians in the United States. The TIC-PAT was constructed to provide a short, validated measure of TIC among healthcare providers. A unidimensional 10-item measure had both good reliability and model fit statistics and face and content validity. Each of the questions in the 1-factor TIC-PAT aligned with the 5 domain areas of the TIC Pyramid 9 framework including patient-centered communication and care, understanding the health effects of trauma, interprofessional collaboration, understanding providers’ own history and reactions to trauma and screening. Because of the 1-factor model, subscales were not identified for each domain area.
In the realm of TIC measurement instruments, limited options exist for healthcare settings. King et al 6 successfully validated a comprehensive 21-item tool assessing TIC knowledge, attitudes, and practices among healthcare professionals. Baker et al 7 introduced the ARTIC, offering a 45-item long form, a 35-item composite form, and a 10-item short form tailored for staff in educational and human service settings. While Kokokyi et al 8 utilized the 29-item Physician TIC Survey, its validation status remains unexplored. Additional TIC-related instruments have been identified across a broad spectrum of care settings. 16 Recognizing the absence of a brief practice-oriented TIC instrument specifically designed for primary care, the current study aimed to fill this gap. The focus was on validating a succinct, 1-dimensional short form emphasizing the assessment of primary care providers’ practices in implementing TIC. This contributes to the literature by offering a targeted and validated instrument tailored to the unique context of primary care settings.
Examining the implementation of TIC in primary care settings offers valuable insights for refining provider education, thereby enhancing the delivery of high-quality, patient-centered care. 17 The assessment of TIC also plays a crucial role in supporting providers’ well-being by bringing issues related to vicarious trauma to light. 18 Utilizing the TIC-PAT, a validated brief instrument, enables an overall evaluation of primary care providers’ provision of TIC, thus furthering these advantages. As a concise form, it is less time-consuming, offering greater convenience for healthcare professionals dealing with time constraints. It also minimizes cognitive load for ease of use and works to support the continuous improvement of primary care providers. Consequently, integrating the TIC-PAT into the onboarding process for new primary care providers would help ensure it becomes a routine part of their healthcare practice and enhance awareness of trauma's impact on health.
Limitations
The results of this study should be interpreted within the context of the following limitations. First, it is considered best practice to conduct EFA and CFA on random split samples. However, because of the small sample size, EFA and CFA were conducted on the same sample. Second, missing data were high (above 30% on some items). The initial 20-item survey was likely more difficult for physicians to complete due to length and time constraints. The 10-item TIC-PAT may be more feasible for busy provider offices to complete. Data appeared to be missing at random, so FIML was used to account for missing data. However, further research should be conducted in other samples with less missing data to ensure similar results in the factor structure. Third, the study utilized a convenience sample, comprising largely White or Caucasian (77%) and male (67%) respondents. This sampling limitation may affect the external validity and generalizability of the findings.
Future research should examine the construct validity of the questionnaire. One way of doing this would be by examining the association between the TIC-PAT and the expected TIC-related patient health outcomes in clinical settings.
Conclusion
To our knowledge, the TIC-PAT is the first short form scale of TIC designed specifically for primary care providers. This study focused on examining the psychometric properties of the TIC-PAT among a group of primary care physicians in the United States, aiming to provide a concise measure of TIC practices among providers. The results demonstrated that the TIC-PAT, with its unidimensional 10-item measure, exhibited good reliability, model fit statistics, and face/content validity. Aligning with the TIC Pyramid 9 framework's five domain areas, this instrument represents a valuable contribution to TIC measurement tools, particularly in the context of primary care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.