
Abstract
Background
Self-scheduling of medical visits is becoming more common but the complexity of applying multiple requirements for self-scheduling has hampered implementation. Mayo Clinic implemented self-scheduling in 2019 and has been increasing its portfolio of self-schedulable visits since then. Our aim was to show measures quantifying the complexity associated with medical visit scheduling and to describe how opportunities and challenges of scheduling complexity apply in self-scheduling.
Methods
We examined scheduled visits from January 1, 2022, through August 24, 2023. For seven visit categories, we counted all unique visit types that were scheduled, for both staff-scheduled and self-scheduled. We examined counts of self-scheduled visit types to identify those with highest uptake during the study period.
Results
There were 9555 unique visit types associated with 20.8 M (million) completed visits. Self-scheduled visit types accounted for 4.0% (838,592/20,769,699) of the completed total visits. Of seven visit categories, self-scheduled established patient visits, testing visits, and procedure visits accounted for 93.5% (784,375/838,592) of all self-scheduled visits. Established patient visits in primary care (10 visit types) accounted for 273,007 (32.6%) of all self-scheduled visits. Testing visits (blood and urine testing, 2 visit types) accounted for 183,870 (21.9%) of all self-scheduled visits. Procedure visits for screening mammograms, bone mineral density, and immunizations (8 visit types) accounted for 147,358 (17.6%) of all self-scheduled visits.
Conclusion
Large numbers of unique visit types comprise a major challenge for self-scheduling. Some visit types are more suitable for self-scheduling. Guideline-based procedure visits such as screening mammograms, bone mineral density exams, and immunizations are examples of visits that have high volumes and can be standardized for self-scheduling. Established patient visits and laboratory testing visits also can be standardized for self-scheduling. Despite the successes, there remain thousands of specific visit types that may need some staff-scheduler intervention to properly schedule.
Keywords
Introduction
Online self-scheduling is used extensively for a large segment of the population for travel reservations, lodging, and entertainment. Travelers have used the internet and mobile connections to self-schedule their airline flights, rail trips, cruises, and rental cars for many years. Self-scheduling hotel and bed and breakfast stays is also not new. Concerts, movies, sporting events, and restaurant reservations are other examples of the plethora of services and events that have self-scheduling available online or by mobile device.
Self-scheduling in medical appointments is a more recent phenomena. For those who want to self-schedule a medical visit and who do not have an established relationship with a medical provider, Zocdoc and Lybrate are services that allow online self-scheduling.1,2 Zocdoc allows patients to scroll through lists of providers from a wide selection of geographic locations and can schedule a wide variety of specialist and generalist visits. In the United Kingdom, the National Health Service (NHS) has self-scheduling of patients with their general practitioners. 3 NHS online 111 also offers some triage prior to recommending a self-scheduled appointment. 4
Online self-scheduling is attractive to patients for a number of reasons. A 2021 survey of 217 online respondents who had booked a service appointment in the past year found that 60% did so online. When asked about the biggest “pain point” of scheduling service appointments, 42% indicated long hold times when booking by phone, and 17% indicated being unable to book by phone other than during provider office hours. 5 The same survey found that 95% were more likely to choose a provider offering online booking over one that didn't (43% answered as “much more likely” and 52% “somewhat more likely”). 5 The complexity and diversity of medical appointments as well as the potential for health consequences and third party costs have made self-scheduling difficult to develop and implement. Even scheduling a routine well-child exam has some challenges. For the child and guardian, it may be preferable to preserve continuity of care and schedule with the child's primary care provider rather than the first mutually agreeable slot with any clinician. Guidelines also dictate changes in the interval between exams as the child ages. 6 Additionally, patient preferences for continuity of care vary based upon whether the visit is for acute or chronic conditions and whether the patient is healthy or has a number of medical comorbidities. 7 Self-scheduled mammograms present other challenges. 8 These radiologic procedures do not require a specific provider but they do have location requirements based on equipment needed for the procedure and mammogram guideline requirements for screening frequency and age when screening starts. 8 The COVID pandemic presented a challenge of scheduling large numbers of COVID tests for those who were exposed and asymptomatic. Symptomatic COVID patients needed to be triaged so that acutely ill patients were not self-scheduling nasal COVID swabs when they needed emergency care. 9 Visit triage before self-scheduling a COVID test is a challenge shared by many symptomatic visit types.
To show the complexity of medical appointment scheduling we quantify and categorize the large number of visit types that are currently scheduled in a multispecialty practice. We also describe additional complexity associated with appointment sequencing, appointment bundling, and pre-appointment data collection needed for successful self-scheduling. In this study we show many examples of completed self-scheduled visits, but we also show that there remain many barriers to successful self-scheduling. Our aim was to give readers an understanding of the ongoing challenges that make medical appointment self-scheduling difficult.
Methods
Setting
Mayo Clinic is a multispecialty medical practice with multiple locations in the USA and internationally. Over 1 million patients come yearly to Mayo Clinic campuses. Mayo Clinic also has multiple primary care sites located in rural, suburban, and urban areas with integrated specialty services nearby.
Scheduling Terminology Used in This Study
The label used by Mayo Clinic to uniquely identify schedulable appointments is the “appointment visit type.” Appointment visit types are given unique numeric codes. All the appointment visit types in this study correspond 1 to 1 with schedulable patient visits, either face to face or virtual. Appointment visit types also identify schedulable patient services such as E-consultations10,11 but patients are not present for these visits, so these visit types were not included in this study. Also in this study we included only completed appointments (appointment no shows were excluded). Since all appointments were completed and involved face-to-face or virtual visits, the term “visit” is used synonymously in this study with completed appointment.
We use the term self-scheduled visit to mean a completed appointment that was scheduled exclusively by the patient (or proxy) online or by mobile app through Mayo Clinic Patient Online Services (the Mayo Clinic patient portal). We use the term staff-scheduled visit to mean a completed appointment that was scheduled with the help of a Mayo Clinic staff scheduler. Visits that were requested online but scheduled by staff were categorized as staff-scheduled visits. Thus, staff-scheduled visits also include online requests for an appointment at a specific time sent via a patient message that went through a staff scheduler to schedule. For self-scheduled visits, the patient/proxy generally sees the same scheduling template that a staff scheduler would see and is able to directly schedule a specific date and time without any staff assistance.
Visit Categories Involved in Patient Care
Mayo Clinic categorizes scheduled patient care visits into 7 mutually exclusive groups.
Consultations: Consultation visit types are generally internal referrals from a Mayo Clinic provider to a Mayo Clinic specialist for consultation on a specific patient care issue. New Patient: This category is for patients who have never been seen within Mayo Clinic (or who have not been seen within a specialty within a defined recent time frame) and were either self-referred or referred by an external provider. New patients require special attention for self-scheduling as they may not have had previous experience with using the Mayo Clinic patient portal, may require clinical review prior to scheduling, and may need to have basic administrative data as well as permissions to share data from other healthcare institutions. Established Patient: These visit types are generally for patients who want to see a provider (specialist or generalist) for another visit (such as continued care). Established patient appointments may be for a specific provider or for a care team member. Established patient visits may also be for a healthcare issue involving new or continued symptoms of varying severity and acuity. Return Patient: Return visits are generally provider-initiated appointments for patients who will return after testing or procedures. This visit type is generally used for providers to explain, review, reexamine, and, with patient input, to plan next steps in their care. Procedures: Procedure visits are for injections, radiology imaging, endoscopy, catheter placement, etc. Testing: Testing visits are for lab tests including venipuncture, but also are used for non-invasive testing such as echocardiograms, electroencephalograms (EEGs), pulmonary function tests, electrocardiograms (ECGs), etc. It should be noted that at Mayo Clinic, outpatient venipunctures and urine collections are a scheduled visit not a “walk in”. Therapy: Therapy visits are for healthcare that may require ongoing regular visits, such as for psychotherapy, physical and occupational therapy, phototherapy for dermatology conditions, and some infusion therapies. Radiation therapy is also included in this category.
During an episode of care, patients may require multiple coordinated visits often from several visit categories. Successful appointment coordination ensures that visits are scheduled at the most convenient locations for the patient, with the proper provider and with adequate spacing between appointments for transportation and resulting of tests. This is an ongoing challenge for self-scheduling.
Development of Self-Scheduling at Mayo Clinic
Development of self-scheduling started with well-child visits and screening mammograms. Those visit types had some advantages in terms of limited complexity,6,8 and both of them had specific guidelines on when to schedule.12,13 Also, because well child exams and screening mammograms are preventive services, those visit types are not associated with a symptomatic illness that could require a triage process. Appointments for immunizations were also based on consensus protocols that were well-defined and already had scheduling templates and nursing infrastructure to implement. Guideline directed immunization was also one of the earlier processes to successfully use self-scheduling.
The COVID pandemic presented an urgent need for self-scheduling and Mayo Clinic patients successfully self-scheduled over 100,000 COVID PCR nasal swab visits. 9 This, as well as broad use of self-scheduling of COVID vaccinations, informed both on the viability of the self-scheduling system and patients’ desire to use a digital platform to schedule visits. The system worked well for this high-volume situation and was used by all patient demographics.
Routine follow-up visits in primary care were another early target for self-scheduling. Patients in primary care often have chronic diseases that require regular follow up to monitor their diabetes, high blood pressure, or lipid management. In addition to scheduling at regular intervals, these recurring visits may benefit from pre-visit scheduling of laboratory tests such as a metabolic profile, lipid profile, or a hemoglobin A1c. The challenge with these visit types was the bundling of pre-visit laboratory and timing the laboratory visits correctly with the follow up provider visit.
Other visit types followed with more challenges involved. Unlike chronic disease visits, new symptom visits in primary care often require triage before scheduling. To address that need a self-triage tool was developed so that patients could self-triage before self-scheduling a visit. Low risk symptoms such as ear and hearing concerns 14 were initially self-triaged before being self-scheduled.15,16
For specialty care, visit self-scheduling (in person and virtual) started more slowly due to unique challenges with each specialty. Self-scheduling for routine specialist consultations or return visits required stakeholder input from each of the specialty practices to manage scheduling processes often unique to that specialty. Specialists often want tests or imaging scheduled in advance of a visit so that results are available to aid in diagnoses and treatment decisions at the time of the consultation. Cardiologists wanted pre-visit testing with echocardiography and electrocardiography for some visit types. Orthopedists wanted specific x-rays with specific views taken, and transplant specialists wanted the ability for patients to self-schedule a large set of blood tests at regular intervals. With enhancements of self-scheduling capabilities, an inventory of self-scheduling processes grew over time to meet the needs of diverse specialties with diverse and unique patient needs.
Scheduling Complexity Background
Each of the 7 mutually exclusive visit categories has hundreds of mutually exclusive visit types. The unique visit types are created with input from multiple stakeholders, including physician and provider staff, access management staff, lab and procedural staff, billing staff, and others. These scheduling visit types as a group create an inventory of visit types that capture many of the nuances of multiple domains of scheduling other than date and time of visit.
Examples of the multiple domains of scheduling include specialty of care (cardiology, obstetrics, family medicine, etc) and subspecialty of care (heart rhythm subspecialist, heart failure subspecialist, heart transplant subspecialist, heart valve subspecialist, etc). Other domains include provider of care (physician, physician assistant, nurse practitioner, nurse, etc), length of visit required, anticipated ancillary equipment or staff needed (eg breast MRI, breast tomography, breast ultrasound), and level of care (eg screening breast tomography vs diagnostic breast tomography). Each of the visit types are assigned unique numeric codes, avoiding unnecessary duplication of visit types for similar appointments.
These unique visit types are the foundation for scheduling. The unique visit types link patients with institutional scheduling templates. Scheduling templates can be as granular as a single provider calendar. For example, for the well-child exam, continuity of care is important; self-scheduling the well-child visit requires that child's parent/proxy links with the schedule of the child's assigned provider. For self-scheduling of screening mammograms, the unique visit type links the patient with one of many radiology scheduling resource templates. The specific radiology scheduling template that gets linked to the screening mammogram visit for a specific patient depends on patient location and the radiology location that has the screening mammography resources.
Self-Scheduling Example
To explain scheduling nuances it is instructive to examine a patient example that could occur by exclusively using self-scheduling processes at Mayo Clinic. Table 1 shows a schedule of visits that could all be self-scheduled by a Mayo Clinic patient. It shows self-scheduling of several visit categories and visit types.
Example of self-schedulable visits from a case illustration of a 25 year old following an ankle injury. This illustrates a single episode of care where multiple visit types are all self-scheduled. Processes that created the self-scheduled visits are in parentheses in the first column. Visit categories with their associated unique visit types are listed in the second column. The third column identifies an additional level of complexity from bundling tests or procedures within visits. In this example, two x-ray views were bundled in a single radiology visit, three lab tests were bundled in one lab blood draw visit, and 2 immunizations were bundled in a single immunization visit. In the third column, unique order types are used to indicate multiple services bundled within a unique visit type.
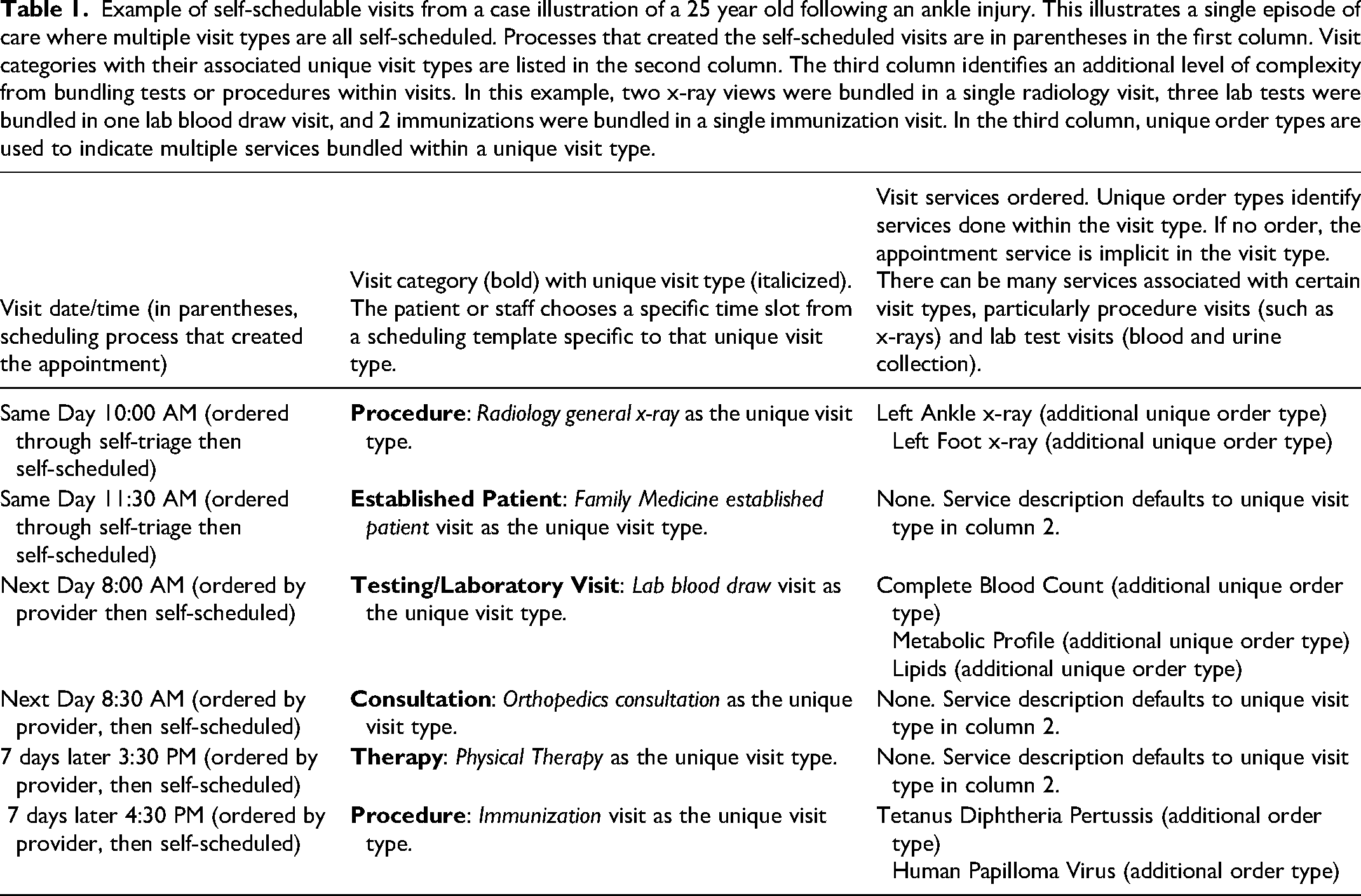
The patient is a 25 year old who was out for a 6 AM ride on a mountain bike trail and fell, injuring his left ankle and foot. He is an established patient at Mayo Clinic and logged into the Mayo Clinic portal Check Symptoms app from his mobile phone where he could self-triage for his ankle injury. After answering some questions about the injury, including some questions using Ottawa rules logic for x-rays of lower extremity injuries, 17 he was offered an opportunity to self-schedule left ankle and foot x-rays prior to a visit with his family medicine provider. He self-scheduled both visits (Table 1, rows 1 and 2). The self-scheduled procedure visit was a radiology visit with the x-rays appropriately sequenced prior to his family medicine office visit so that the provider could have the x-ray interpretation available during the scheduled face to face visit. At the family medicine visit the provider noted some larger and more widely distributed ecchymoses than expected, some weight loss, but no lacerations or large abrasions. The patient stated he had more thirst and urination recently. Although no fracture seen, the family medicine provider wanted further input from orthopedics about additional evaluation since weight bearing was an issue. An orthopedic consultation was ordered and crutches supplied from the office. For the bruising, weight loss, extra thirst and urination, the provider ordered a complete blood count (CBC), complete metabolic profile (CMP), and a lipid profile (family history of high cholesterol). The electronic record also indicated that the patient was due for a Tetanus, Diphtheria, Pertussis (TDaP) immunization and the patient also wanted a Human Papilloma Virus (HPV) vaccine. These vaccinations were also ordered by the provider but the patient wanted to schedule later.
On his way out, the provider orders were finalized by staff at the checkout desk. At that time the patient was given the option to self-schedule the ordered tasks. He elected to self-schedule and the desk checkout staff sent the 3 separate appointment invitations for orthopedics, labs tests, and immunizations to the patient's online services account. The patient was able to self-schedule his orthopedic visit for early the next day and decided to get the blood tests then as well because he could be fasting (Table 1 rows 3 and 4). At the orthopedic visit, an order was placed for physical therapy a week later. He self-scheduled the physical therapy visit for a week later and was able to self-schedule the ordered TDaP and HPV vaccines right before that visit to avoid an additional trip to the clinic (Table 1 rows 5 and 6).
This case illustration was designed to help readers understand several features of the self-scheduling process and the visit types involved. This example involved 5 of the 7 visit categories (established patient visit, procedure, testing, consultation, and therapy), and 6 unique visit types.
Self-scheduling is possible through different processes. Self-scheduling through self-triage 16 and self-scheduling after provider creation of an order are illustrated here. Self-scheduling can also be initiated by an EHR-generated portal invitation to the patient for screening mammograms, or self-initiated through the patient portal as with well-child visits.6,8
Scheduling Complexity Primary Measure
Our primary measure of scheduling complexity was the number of unique visit types that were used for patient scheduling. Each of these unique visit types contained necessary information for scheduling the visit. As a group this is an inventory of visit types Mayo Clinic uses to match patients and their healthcare needs with the right providers, the right tests, the right procedures, and at the right times to optimize healthcare service. We used only visit types that had been scheduled and successfully resulted in completed visits. As noted previously, we excluded all scheduled appointments that were no shows. Counts of unique visit types associated with self-scheduled visits were compared with staff-scheduled unique appointment visit types. The fraction of total unique visit types that were self-scheduled was used to compare the inventory of self-schedulable appointment types to the total inventory of all schedulable appointments. This information is used to identify the current successes of self-scheduling (those with self-scheduled completed visits), and to look for opportunities among visit types yet to be self-scheduled.
Data Collection
We used the data sources of the Mayo Clinic Enterprise Office of Access Management to capture appointment data. Our study spanned 85 weeks of completed visits from January 1, 2022 through August 24, 2023. We collected counts of self-scheduled and staff-scheduled visits, visit categories of the appointments (new patient, established patient, consultation, procedure, etc) and counts of unique visit types associated with completed visits.
Statistics and Ethics
We used Stata 18.0 (College Station, Texas, USA) for data analysis. Chi-Square was used for difference in counts between categories. Our dependent variable was whether a visit was self-scheduled or not. Independent variables included age, sex, race, ethnicity, appointment visit category and unique appointment visit type. This study was classified as exempt by the Mayo Clinic Institutional Review Board (IRB 20-006809)
Results
Scheduling Counts and Demographics: Self-Scheduled Compared to Staff-Scheduled
From January 1, 2022 through August 24, 2023 there were 20,769,699 completed patient care related visits for 1,383,934 patients. Of the entire 1,383,934 patients, 80.6% were registered to Patient Online Services (Mayo Clinic patient portal). Of the entire 20.8 million (M) completed visits, 838,592 (4.0%) were self-scheduled and 19.9M (96%) were staff-scheduled. There were 342,069 patients of 1.38 M total patients (24.7%) who completed at least one self-scheduled visit, and 1.04 M patients (75.3%) whose completed visits were entirely staff-scheduled.
Table 2 shows the demographic comparison of self-scheduled to staff-scheduled patients. There were significant differences in age, with self-schedulers being younger. Self-schedulers were also more female and white, and as a group had fewer Hispanics proportionately. Self-schedulers were almost all registered with Mayo Clinic Patient Online Services (new patient self-scheduling may be accomplished without portal registration). For those who exclusively used staff schedulers, 74.5% (776,082/1,041,865) had a portal account (registered to Mayo Clinic Patient Online Services) for at least part of the study, and thus would have had access to self-scheduling.
Demographics of Patients who Completed any Visits That Were Self-Scheduled Compared to Demographics of Those who Completed Visits Exclusively Scheduled by a Staff-Scheduler.

Table 3 shows the counts and percents for self-scheduled and staff-scheduled visits by each visit category.
Counts and Percentages of Self-Scheduled and Staff-Scheduled Visits by Visit Category.

Of seven visit type categories, self-scheduled established patient visits, testing visits, and procedure visits accounted for 93.5% (784,375/838,592) of all self-scheduled visits and were the top three categories in terms of percent self-scheduled. Established patient visits in primary care (10 visit types) accounted for 273,007 (32.6%) of self-scheduled visits. Testing visits (blood and urine test, 2 visit types) accounted for 183,870 (21.9%) of self-scheduled visits. Procedure visits for screening mammograms, bone mineral density, and immunizations (8 unique visit types) accounted for 147,358 (17.6%) of self-scheduled visits.
Scheduling Complexity: Staff-Scheduled Versus Self-Scheduled
Table 4 shows the counts of the unique appointment visit types that were associated with the seven different categories of staff-scheduled and self-scheduled visits.
Counts of Unique Visit Types That Were Successfully Staff-Scheduled or Self-Scheduled During the 85 Week Study Time Frame. Unique Visit Types Included Only Those That had Verified Completed Appointments.

The appointment types represented in self-scheduled visits were all less than 30% of each of the staff-scheduled appointment types. Thus, there are many appointment types that have yet to be self-scheduled.
Self-Scheduling Challenges and Successes
Table 5 puts into perspective some of the challenges and successes of self-scheduling. It contains examples of some of the counts of successful self-scheduled appointments. Also in Table 5 is a column listing examples of work needed in the continuing development of self-schedulable appointment types.
Summary of experience with opportunities, challenges, successes, and work to be done for defined visit categories.

Discussion
Principal Findings
A multispecialty practice can have thousands of unique appointment visit types. These appointment types are needed to accommodate the diversity of individual patient needs, services requested, provider expertise, and scheduling templates. In our practice, self-scheduled completed visits were associated with less than 2000 appointment types compared to more than 9500 unique appointment types that were staff-scheduled. Overall, self-scheduled visits accounted for 4.0% of all scheduled and completed visits over the 85 week study period. Visit categories with the highest percent self-scheduled visits were established patients (7.1%; 414,088/5,872,276), procedures (3.4%; 166,757/4,852,221), and testing (3.7%; 203,530/5,465,960). Despite having only 4% of total appointments self-scheduled, the self-scheduled completed appointment count was over 800,000.
Practice Implications
Although self-scheduling has had successes in some appointment visit categories and some appointment visit types, it is not clear that a dramatic acceleration of self-scheduling success is inevitable. The thousands of appointment visit types that each have specific scheduling criteria makes it difficult to achieve rapid progress. In addition, the initial successes were in appointment types chosen to have fewer challenges for self-scheduling. For example, established patients in primary care do not require the intake information and pre-visit testing that specialty consultations often need. Success with self-scheduled lab tests is in part due to standardized lab calendars that do not need much modification in the self-scheduling process.
Although significant effort goes into developing self-scheduled appointment types, we are seeing some payoffs in reduced staff work. During the COVID pandemic, staff-schedulers had to respond to a surge in demand for COVID testing. Published reports of self-scheduled COVID testing showed a significant reduction in the amount of staff time involved in scheduling and triage.9,18,19
Self-scheduled mammograms also showed a payoff in reduced staff time for rescheduling. Staff-scheduled mammograms involved extra staff time for subsequent reschedules in 25%. 8 For self-scheduled mammograms, rescheduling occurred in only 7%. 8
Future areas of study should assess how much rework may be associated with self-scheduling. As practices start to use self-scheduling to proactively monitor chronic disease, there can be some additional complexity with patient preferences and comorbidities. Software can accurately select patients who are due for diabetes lab monitoring and send them an appointment offer to schedule a hemoglobin A1c. However, the patient may have other concerns and comorbidities not taken into account in the self-scheduling process. The patient may remember a lipid test, potassium, liver enzyme, or other test that she or her provider wanted to recheck in addition to the hemoglobin A1c that was self-scheduled. As a result, the patient messages the provider that she wants a lipid, potassium, or other test added on to the self-scheduled blood draw. Although adding additional tests to the self-scheduled blood draw can be accomplished, it involves provider and staff input in what was meant to be an automated process.
Non-visit care work burden may be decreased by some self-scheduling. For example, there is some evidence that office visits self-scheduled for ear and hearing concerns were associated with fewer non-visit care tasks such as patient messages, nurse triage, and other patient communications. 16
Patient Implications
Despite the complexity involved with scheduling, the effort to develop and implement self-scheduling appears to be paying off in terms of patient engagement. Previous published work with self-scheduled appointment types have shown that patients take advantage of the 24/7 convenience of self-scheduling. Patients were engaged in self-scheduling from 24% to 43% outside of normal weekday business hours depending on whether self-scheduling screening mammograms, 8 well-child exams, 6 COVID tests, 9 or getting self-triage for self-scheduling of ear and hearing concerns.6,8,9,16 In addition, patient self-scheduling of screening mammography at Johns Hopkins in the US increased 10 fold over 8 years from 3.7%to 37%. 20
Our institution has found that some of the complexity associated with scheduling may be an opportunity for increased patient choice. In our established patient visit types in primary care, continuity of care with their own provider is usually given priority. However, if the time and date selections to see their own provider are not acceptable then they are given the choice to pick dates and times from the schedules of alternate providers on the same care team. Patients often have differing preferences for continuity of care depending on their health status and whether their complaint is perceived as acute or chronic.7,21
Not all patient groups have the same uptake of self-scheduling. There are relatively few articles specifically looking at social and demographic factors that may affect self-scheduling. However, there is more data regarding electronic patient portal use which is a necessary component of self-scheduling. Our findings that younger adults and white, non-hispanic patients are more likely to utilize self-scheduling matches published research regarding mammogram scheduling, telemedicine use during COVID-19, and patient portal use.22–24 Such disparities may further exacerbate access to healthcare among groups at highest risk for poor healthcare outcomes from chronic disease.25,26 Further research is indicated to develop methods ensuring groups at highest risk of poor outcomes have access to self-scheduling convenience.
Future of Self-Scheduled Appointment Scheduling
The need for large numbers of appointment types is unlikely to change. Multispecialty practices will continue to need diverse appointment types to serve the needs of increasingly specialized care. Subspecialty visits are often limited to small groups of subspecialists or even individual subspecialty providers supported by subspecialized care teams. For example, transplant visits both for initial evaluation and subsequent care often involve subspecialty providers and care teams that require unique visit types to reflect this type of care.
As we look to bring in more visit types to become self-schedulable, there are tradeoffs involved. There are development costs which may eventually be paid for by decreased staff-scheduler time. As mentioned previously, there were some estimates of time saved for COVID test self-scheduling by two healthcare institutions, UCSF and Mayo Clinic.9,19 However, with increasing complexity involved in self-scheduling there will need to be further cost benefit analyses prior to developing some highly specific self-schedulable appointments. Self-scheduling lab tests is likely cost-effective because of the numbers of tests involved even if the percent self-scheduled is low (3.7%). However, we need additional research to know how much rework may be occurring because of additional tests needed to be ordered or other modifications of the lab test visit. Other visit types may appear to be cost-effective for self-scheduling because of perceived low development cost and implementation, but they may suffer from low volumes of use, unintended consequences, and inability to sustain maintenance costs.
There is much work to be done around appointment itineraries with more complex visits. Specialist consultations can involve pre-visit questionnaires, review of outside materials, triage of symptoms, scheduling of pre-visit tests, imaging, and procedures. For more efficient use of provider time, these tests, images, and procedures may need to be completed and interpreted before the provider visit. This is no small task and we can only speculate how often rework may be needed in such a complex choreography of scheduling. It is unclear how much self-scheduling can improve parts or all of these more complex scheduling processes, and whether the development costs and maintenance of self-scheduling processes will be paid for by efficiency gains.
Limitations
Mayo Clinic sees patients of all ages who see and get care from primary care providers, specialists and subspecialists. Our appointment visit types represent the wide variety of patients and healthcare conditions that are seen at Mayo Clinic. Our institution uses general appointment visit category types (established patient, new patient, etc) and appointment types (eg established patient family medicine office visit) that are used by many other institutions and are partially generalizable. However, our entire inventory of over 9000 unique visit types, used in varying frequencies during the study, would not be expected to be completely replicated elsewhere.
Numbers of different visit types is a measure of the diversity of appointments but is an imperfect measure of complexity. For example, appointment visit types could be designed to be different for different hours of service such as evenings, or different days, such as weekends. Mayo Clinic does not do this, but theoretically an established patient visit could have a different unique visit type for an appointment on the weekend if the institution thought that was important to distinguish. Our study assumes that the visit types reflect significant differences in the who, what, and duration of visits. The when and where are generally handled by scheduling algorithms and not included in the Mayo Clinic visit types. Also, some healthcare institutions may have less specificity for their visit types and thus have fewer visit types.
Mayo Clinic prioritized the development of certain self-scheduled visits which is reflected in this study. Other healthcare institutions may have prioritized other visit types to self-schedule and may have different views of the challenges posed by self-scheduled visits.
Conclusion
Scheduling for healthcare related appointments is complex. Self-scheduled visits have been successful in some of the less challenging cases of self-scheduling. Our study shows a plethora of appointment types that remain to be considered for self-scheduling. However, the effort needed to develop many of these may increase significantly. Further research into self-scheduling will be important to assess current self-scheduled visits as well as to determine how to prioritize future self-scheduling work based on anticipated development costs and future savings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Data Availability Statement
Data sharing of additional appointment information is not applicable to this article.