
Abstract
Background/Objective
The prevalence of chronic pain and its links to the opioid epidemic have given way to widespread aims to improve pain management care and reduce opioid use, especially in rural areas. Pain Management Specialty Care Access Network-Extension for Community Health Outcomes (VA-ECHO) promotes increased pain care access to rural Veterans through knowledge sharing from specialists to primary care providers (PCPs). We explored PCP participants’ experiences in VA-ECHO and pain management care.
Methods
This qualitative study is based on a descriptive secondary analysis of semi-structured interviews (n = 10) and 3 focus groups with PCPs participating in VA-ECHO from 2017–2019. A rapid matrix analysis approach was used to analyze participants’ responses.
Results
VA-ECHO was an effective workforce development strategy for meeting PCPs’ training needs by providing pain management knowledge and skills training (eg alternative care approaches and communicating treatment options). Having protected time to participate in VA-ECHO was a challenge for many PCPs, mitigated by leadership and administrative support. Participants who volunteer to participate had more positive experiences than those required to attend.
Conclusions
VA-ECHO could be used for meeting the workforce development needs of PCPs. Respondents were satisfied with the program citing improvement in their practice and increased confidence in providing pain management care to Veterans despite some challenges to participation. These findings offer insight into using VA-ECHO to meet the VHA’s workforce development to improve Veterans’ access to pain management care. The ECHO model presents opportunities for workforce development in large complex healthcare systems and garnering ongoing support for this training model is necessary for promoting workforce development for PCPs.
Introduction
Chronic pain is a major public health problem affecting over 20% of the U.S. adult population 1 and is linked to the opioid epidemic in the United States. Individuals in rural areas are particularly impacted due to varying factors, including limited access to pain care since pain management clinics are mainly located in urban medical center settings, reliance on primary care for pain management and barriers to accessing non-pharmacologic pain treatments.2,3 The opioid epidemic has prompted widespread aims to change pain management practice policies across various settings 4 to reduce the suffering from pain, while also containing the rising toll of harms associated with opioid medications. 3 The Veterans Health Administration (VHA) provides training to primary care providers (PCP) and staff to improve their understanding of and ability to provide pain management care, including providing alternative pain care and strategies for reducing opioid use especially among rural Veterans. 5 These efforts require practitioners to find balance between providing appropriate chronic pain care and minimizing opioid misuse.
The VHA Specialty Care Access Network-Extension for Community Health Outcomes (SCAN-ECHO, also known as VA-ECHO) program, adapted from Project ECHO®4,6 was designed to increase rural Veterans’ access to specialty care by training VHA PCPs to deliver pain management care. Remote training and mentoring are particularly suited for rural areas where workforce development may not be the focus and less resources are available. Workforce development involves coordination of programs and policies in an organization that influences the success of employees and work system by prioritizing ongoing education and skills development to positively influence the future success of a program. 7 Although VA-ECHO and similar programs for chronic pain 8 aim to educate and empower PCPs, the success of these programs is not clear, 9 particularly as a workforce development strategy. Studies evaluating VA-ECHO demonstrate the program’s impact on improving pain management for Veterans, indicating positive outcomes in terms of PCPs’ confidence and knowledge of treating chronic pain and higher patient utilization of other health services (ie mental health, physical therapy) as opposed to opioid prescribing.10–13
Prior pain management VA-ECHO studies used quantitative measures, including surveys, to measure training outcomes (eg, confidence, knowledge, prescribing trends, patient service utilization).11,12 We used qualitative methods to extend our understanding of VA-ECHO as a workforce development strategy for the VHA to improve pain care, a concept that is limited in literature about the ECHO method. This analysis focused on a subset of data from a larger evaluation of Pain Management VA-ECHO. 14 The objective of this paper was to describe how PCPs’ participation improved their knowledge and skills for pain care and to inform strategies for workforce development.
Methods
Qualitative methods were used in this study and as part of a larger evaluation of VA-ECHO programs 14 focused on informing the expansion and implementation of VA-ECHO to improve veterans’ access to pain management care. Qualitative methods offer a way to understand what is happening, why and how providers and patients are impacted by interventions and can capture complexities and nuances that are immeasurable by quantitative measures. 15 This secondary analysis focused on a subgroup of PCPs who participated in a pain management VA-ECHO program included in the larger evaluation. We chose to focus on one VA-ECHO pain management program and their participants to control for programmatic variations across VA-ECHO programs included in the original evaluation. Evaluation activities were reviewed by the Research and Development Committee and deemed to constitute healthcare operations and not human subjects research. 16 VHA employee unions reviewed and approved instruments before recruitment and data collection started. Participation in the evaluation was voluntary and participants consented to the use of the anonymized data for reports and future publications.
Participants and Setting
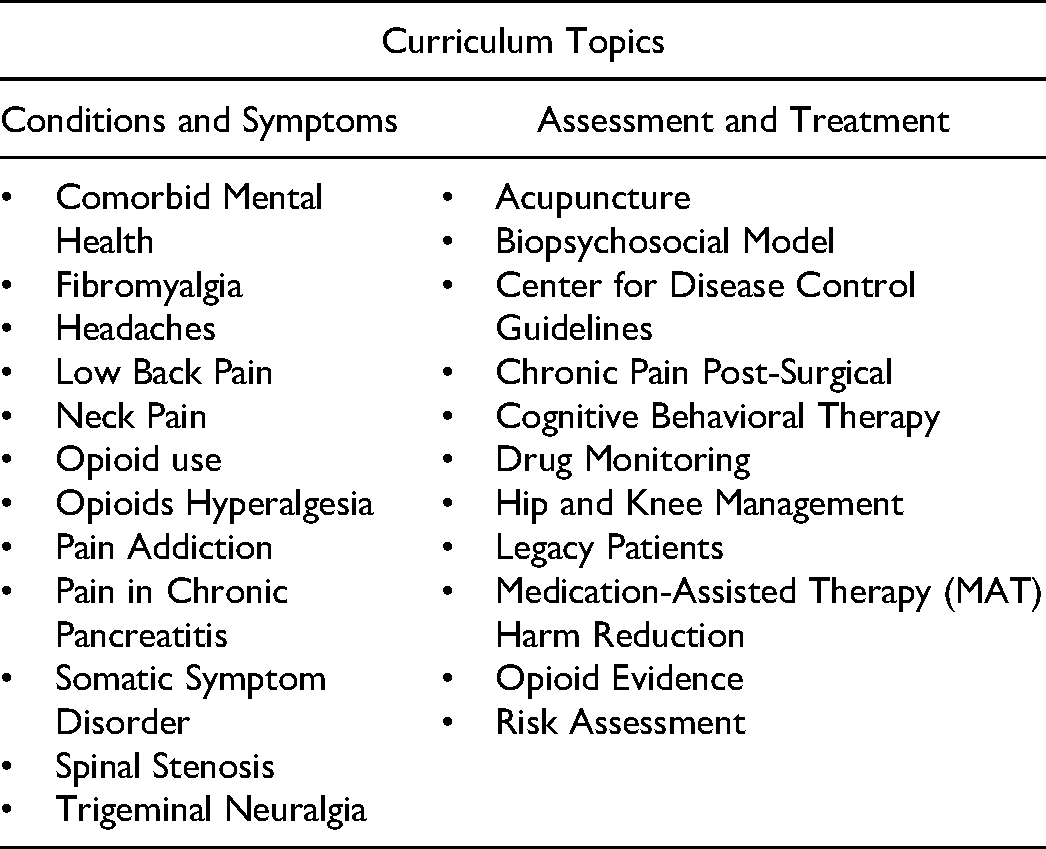
The pain management VA-ECHO program was delivered from a midwestern, urban Veterans Affairs Medical Center (VAMC; hub site; Figure 1) using video teleconferencing technology. The program was led by a multidisciplinary pain management specialist care team. The pain management specialty team invited a cohort of primary care providers (PCPs) delivering care in outpatient clinics within geographically diverse urban and rural VAMCs and VHA Community-Based Outpatient Clinics (CBOCs) (these VAMCs and CBOCs referred to as spoke sites). The specialty team facilitated weekly meetings over the course of one year that included didactic training, mentoring, and case consultations covering a range of pain management topics (Table 1). Sessions lasted approximately one hour. Additional topics were introduced based on participant feedback.

Pain management VA-ECHO program structure.
VA-ECHO Curriculum Topics.
The Table Below Lists Examples of Topics Covered in the VA-ECHO Curriculum. Note That Additional Topics Were Discussed Throughout the Program Based on Participant Feedback.
Seventy-five (N = 75) PCPs (physician assistants, physicians, and/or nurse practitioners) from five rural and urban midwestern spoke sites were trained between 2016 and 2019. Program attendance data were used to identify these program participants for recruitment.
Data Collection and Analysis
Primary data collection was completed between May and September 2018 by an experienced team of qualitative researchers. A semi-structured interview guide (previously published by Ball and colleagues 14 ) and focus group guides (Appendices 1.1 and 1.2) were used to explore providers’ experiences delivering pain management care and participating in the VA-ECHO program, including facilitators and barriers to attendance, practice changes, perceptions of the impact of program on patient care and access, and suggestions for program improvement. Individual interviews lasted approximately 30 min. Pre- and post-participation focus groups lasted 30 to 60 min. Interviews and focus groups were audio recorded and transcribed for analysis.
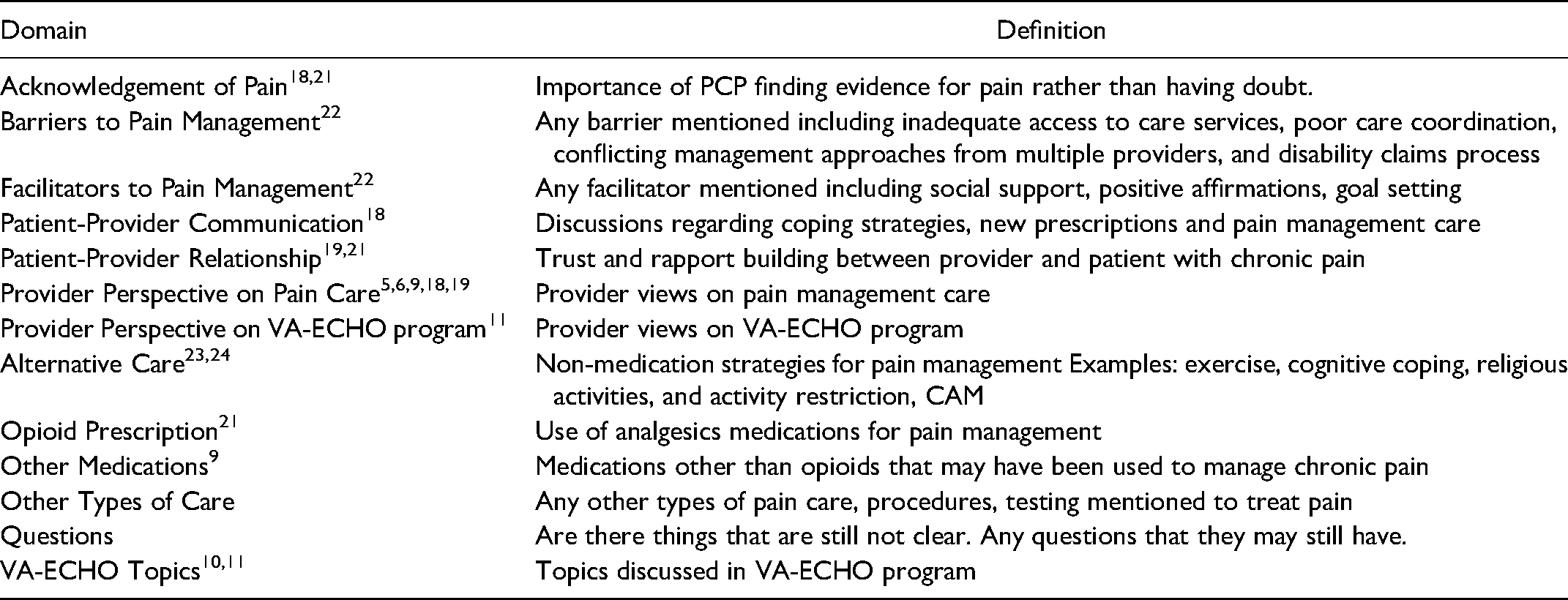
Interview and focus group data were aggregated for rapid matrix analysis 17 applying deductive domains 18 (Table 2) from key definitions derived from the literature including workforce development, 7 confidence in treating pain, 19 barriers to pain management, 20 patient-provider communication, 18 alternative care, opioid prescribing for pain management, and provider perspectives on pain care. 20 Analyses focused on understanding how PCPs’ participation in VA-ECHO improved their knowledge and skills for pain care to inform strategies for workforce development. Inductive domains were added to capture emergent topics (eg experiences with program enrollment). These steps were repeated and included regular discussion among the primary qualitative team to verify the validity and credibility of findings to reach consensus.
Domain Matrix.
Results
We completed eleven (n = 11) individual interviews with program participants. One respondent (n = 1) was not a PCP, and their data were excluded from the analysis. Ten respondents (n = 10) included physicians (3 male, 7 female) from rural and urban spoke sites (3 rural, 7 urban). We facilitated three focus groups, all were a gender-mixed composition of five to eight respondents from rural and urban spoke sites. The final data analyses included the aggregated findings from individual PCP interviews (n = 10) and focus group data.
Five main findings are presented, reporting PCPs’ perspectives on how VA-ECHO facilitated workforce development, how providers’ training needs and expectations were met, how the training improved providers’ knowledge and skills, and the ways in which barriers and facilitators to program participation and voluntary program enrollment influenced participants’ experience.
VA-ECHO Facilitates Workforce Development on System Level
Most respondents reported that the ECHO-based training and education of providers could help them improve care delivered to patients on a healthcare-system level, supporting the definition of workforce development (Table 3 quotation (Q1).
Supporting Quotations for Findings.

Facilitating Practice Changes to Improve Workforce Development on an Individual Level
Meeting Providers’ Training Expectations and Needs
Respondents reported wanting to learn to improve conversations with their patients about tapering medications and alternative pain care strategies. Many respondents were satisfied with the breadth of topics presented, but some respondents felt the program was too focused on minimizing opioid prescribing and that there were some missing topics (e.g pain management for geriatric patients, hospice, and palliative care) reflective of the respondents’ individual patient populations (Q2). Many respondents identified case presentations as valuable and helpful for understanding complex patients representative of their patient panel (Q3).
Improving Providers’ Pain Management Knowledge and Skills
Most respondents reported improved knowledge and abilities to deliver pain care (Q4). Many respondents described making more appropriate referrals, reducing new and tapering existing opioid prescriptions (Q5).
Barriers, Challenges, and Facilitators to Program Participation
Providers described barriers, challenges, and facilitators to participating in VA-ECHO. Having limited time for participation and scheduling conflicts with patient care was a challenge for some but could also be a barrier to participation (Q6).
Supervisory support for flexibility in making their schedule and having supervisors “block time off,” and obtaining “administrative support” and “buy-in” from Chief of Staff were essential facilitators for respondents participating in the program (Q7).
Voluntary Program Enrollment Influences Participant Experience
Respondents reported being recruited to participate in the program in various ways. Some learned about the program at a pain conference, some received emails from administrators asking about their interest in the program, and others were directed to participate by their organization’s leadership (Q8). Many respondents participated in the program based on their own learning objectives, eg, to learn about pain management options and resources; Others wished to change the culture of pain management at their site.
Although most respondents reported positive experiences with the program. Providers’ perception of whether their participation was voluntary influenced their overall program experience. Those who volunteered to enroll in the program emphasized their satisfaction with the program and reported little to no complaints about the program itself. Some respondents who were required to participate by their supervisors, or perceived that participation was mandatory due to performance issues (eg opioid prescribing rates) discussed more criticisms of the program (Q9).
Discussion
The objective of this analysis was to describe PCPs’ experiences participating in VA-ECHO and how this program contributed to their workforce development for pain management care. Providers perceived their knowledge and skills improved through participating in the program. Respondents who volunteered to participate in the program expressed more positive experiences with the program. Limited time and scheduling constraints were reported as the main barriers to participation, and administrative support was essential to overcome this barrier.
Previous remote training and mentoring program studies have focused on improving relevant patient and provider outcomes. 9 Using an interprofessional training model similar to VA-ECHO is an effective approach for pain care.4,10–14 Our work extends our understanding of program participants’ experiences with VA-ECHO and provides evidence supporting how this program fulfilled participants’ workforce development needs. The ECHO model presents opportunities for workforce development in large, complex healthcare systems, and there is support for this training model to be used as an effective approach for promoting workforce development for providers treating opioid use disorders. 9
Pain management care for geriatric, palliative, and hospice patients was an unmet training need identified by some respondents based on their individual patient populations. Overall, most providers reported that VA-ECHO program provided knowledge and skills necessary for reducing opioid prescribing, making more appropriate referrals for pain management care, and improved the quality of care they delivered. These findings align with another study’s evaluation of Project ECHO for substance use disorders 9 to promote workforce development which found that providers experienced increased self-efficacy and overall improvement of their knowledge. Our study of VA providers identified similar findings, supporting the use of VA-ECHO as a strategy for to address the shortage of pain management care services in remote and underserved areas. 5
An emergent finding from this analysis was that for some participants, volunteering versus required participation may influence their experience of the program. This was important for workforce development as it suggested that allowing participants to volunteer to participate may foster positive experiences for participants. The time commitment required for participation in VA-ECHO may conflict with meeting performance metrics focused on seeing more patients and increasing access and may deter or prevent participation. 21 Reduced clinic time was found to be the main barrier to participation in another study. 9 These competing demands of mandated participant enrollment and reduced clinic time impact workforce development and have implications for organizational assessment of performance measures and their prioritization. 25 Program participant engagement strategies should be examined to garner buy-in and address barriers to participation.
Limitations
The findings may not be representative of all VA-ECHO programs which span a range of specialties and program participants and may not be generalizable to non-VHA providers. Given that this work was a secondary analysis and individual demographics were not initially collected, we were not able to identify individual respondents and thus participant-level analysis was limited. We did not interview providers who chose not to participate in the program. Thus, there may be more we do not understand about barriers to program participation and workforce development needs. Also, the small number of rural respondents limited analysis of factors unique to rural settings.
Strengths
Strengths of this analysis include that the analysis was conducted with the original data set and with members of the primary evaluation team involved in the original data collection and analyses 14 and prior evaluations of pain management VA-ECHO.10–13 Although our overall respondent numbers were limited, our data were sufficient in quality and quantity due to the narrow evaluation scope, purposive sample, rich quality data collected through the methods employed, and analysis approach support substantive data saturation to generate informative, meaningful findings. 25
Future Directions
Future directions for the program could include expanding the program curriculum to address the pain management needs of geriatric, palliative, and hospice care. Additional studies are necessary to determine the program’s impact on rural populations. 9 Future studies should incorporate mixed-methods to measure the effectiveness of VA-ECHO training for reducing opioid prescribing and impact on other patient care outcomes. 26
Conclusions
Most respondents reported that VA-ECHO supported their professional development for delivering pain management care. Providers experienced knowledge (eg alternative care approaches) and skills (eg communicating treatment options with patients) improvements through program participation. Limited time and scheduling constraints were reported as the main barriers to participation, and administrative support (eg scheduling flexibility and supervisor buy-in) was essential to overcome this barrier. Although providers described challenges to participation and some unmet training needs, overall, the respondents felt that participation in the VA-ECHO program improved their practice and increased their confidence in providing pain care. These findings support that VA-ECHO contributed to their workforce development for pain management care.
Footnotes
Acknowledgments
This work was supported by the VA Collaborative Evaluation Center, A collaboration of VA Medical Centers in Aurora, CO, Seattle, WA, and Cleveland, OH.
Author Contributions
SS, KS, LS, and SB contributed to the study design, data collection, data analysis and writing the manuscript. DA, MH and DCA were primarily responsible for the design of the larger evaluation of the SCAN-ECHO program and contributed to the writing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided by the Office of Rural Health. Visit www.ruralhealth.va.gov to learn more.
Appendix 1: Interview and Focus Group Guides
Staff interview and focus group example semi-structured questions and probes.
Generic prompts: If responses are limited or require clarification, probes may be used to illicit more detailed responses. Probes should use words or phrases presented by the participant using one of the following formats:
What do you mean by … ?
Can you tell me more about …?
Can you give me an example of …?
Can you tell me about a time when … ?