
Abstract
Introduction:
As the US health-care system has evolved over the past decade, access to obstetric care in rural communities has declined, and there has been a challenge in retaining obstetrics and gynecology (OB-GYN) providers to train the next generation of physicians. The current pilot study sought to identify the factors that influence faculty who train medical students within the field of OB-GYN with the hope of influencing recruitment and retention of providers for the future.
Methods:
Clinical OB-GYN faculty within the University of Washington School of Medicine regional medical education program were surveyed about practice patterns and beliefs regarding medical student training as part of a pilot study on provider recruitment and retention.
Results:
Fifty-seven eligible respondents completed the survey. Most (88.9%) reported their hospitals encourage student participation in patient care. Students in their practices participate in many aspects of patient care, including conducting exams (96.2%) and participating in the operating room (94.3%). The majority found the rewarding aspects of teaching medical students to be intellectual stimulation (90.9%), continuing the tradition of medical teaching (87.5%), and the intrinsic satisfaction of teaching (83.6%). Challenging aspects of teaching included reduced reimbursement (40%) and the student/workload (63.6%).
Discussion:
Medical student education continues to rely on a generation’s medical professionals to impart their knowledge to the next. We hope that with a better understanding of the benefits of participation and minimization of the challenges, we can perpetuate this tradition despite the uncertainty in our health-care system.
Introduction
The American health-care system is in the midst of the most substantial changes in its history (since the passing of the Social Security Act in 1965 which created Medicare and Medicaid 1 ). At the core of these changes is the goal of providing affordable quality care to as many Americans as possible. Access to care however requires access to a provider and yet the US health-care system is not necessarily organized around training future physicians. Medical education continues to rely principally on an unpaid apprenticeship model. 2 Unfortunately, concerns about issues such as reduced reimbursement and a lack of data to the contrary are impacting the willingness of practicing physicians to train the next generation. 3 –5 As of yet, however, there appears to be no substitute for the education that comes from being in the exam room with a patient while being proctored by an experienced provider. The challenge for all medical schools, therefore, is developing and maintaining these clinical experiences for their students. The primary objective of this pilot study was to identify the factors influencing providers’ willingness to teach medical students as well as their perceived threats to continued participation. 3 This was a subset of a larger survey of practicing obstetrician gynecologists (OB-GYN) who are courtesy faculty of the University of Washington School of Medicine (UWSOM). With this information, we hope to study this topic further through future studies. We believe this information will help to develop and study interventions designed to identify, recruit, and retain health-care providers to the courtesy faculty in the future.
Methods
Sample and Study Design
The sample used for this study consisted of physicians currently practicing OB-GYN in the WWAMI (Washington, Wyoming, Alaska, Montana, Idaho) region where the UWSOM administers its distributed educational model. 6 The physicians were courtesy faculty who volunteer to teach medical students and were part of a larger survey on OB-GYN provider recruitment to the WWAMI region. One hundred fifty-five individuals were initially contacted about the survey in May 2016. Three subsequent e-mails were sent with a link to the online survey over the next 4 weeks. For nonrespondents, 2 separate mailings with paper surveys were sent during July 2016. The survey consisted of 30 questions about practice setting, practice profile, partner recruitment, and teaching, with 8 additional questions about the respondent’s background (see Appendix A). The online survey study was administered through Real Magnet between May and June of 2016.
Data Analysis
For this study, statistical analysis was performed using IBM SPSS Statistics 24.0, IBM Corp (Armonk, New York). The focus of the study was on the questions regarding respondents’ teaching practices and beliefs. The survey consisted of 8 questions regarding this topic and, for purposes of data analysis, responses to question 35 were recoded as follows: responses of “very challenging” or “minimally challenging” were combined and considered to be “challenging”, while responses of “minimally rewarding” and “very rewarding” were combined and considered to be “rewarding”. Question 36 was also recoded by combining responses of “strongly discourages” and “discourages” to create the response “discourages,” while responses of “strongly encourages” and “encourages” were combined and considered as “encourages.” Practice location was condensed to 4 variables instead of 6, with “urban–inner city” and “urban–non-inner city” combined into the response “urban,” and “mid-sized town (10 000-50 000)” and “rural” combined into the response “rural.” “Suburban” and “military” remained separate responses. Chi-square tests were performed for comparative analysis of categorical variables and analysis of variance tests were used to compare group means of continuous variables. Results were considered statistically significant at P < .05. Unless otherwise noted, all percentages reported were calculated excluding missing data.
Results
Response Rates
Of the 155 providers who were initially contacted for this survey, 16 were excluded for not having a correct address and 2 had left the state. Seventy-three of 137 eligible participated for a 53.2% response rate; however, of those 73 participants, only 57 completed the additional questions focused on practice patterns for teaching medical students.
Demographics
The demographics for the respondents are outlined in Table 1. In general, this was a predominantly white group (92.9%), with male practitioners making up the majority (66.1%). Respondents had an average age of 50 and an average of 18 years practice postresidency. Those who practice in a rural location made up 46.4% of the participants, with most respondents practicing general OB-GYN (83.9%). Male respondents had, on average, significantly more years of practice (21.78) and were significantly older (average 53.59 years of age) than female respondents (average of 43.74 years of age and 11.47 years of practice; P < .001).
Demographics.

Student Teaching
The mean number of years that respondents reported teaching medical students was 10.36 years, with a standard deviation of 7.68 years; 42.1% of the respondents also teach DO students and 19.2% of those who teach DO students reported that MD and DO students rotate with them at the same time. The majority (88.9%) indicated the hospital they work in encourages student participation in patient care, while 11.1% said that it discourages student participation.
Clinical Teaching Provided to Students
Respondents were asked whether the students they teach participate in various clinical activities. The most common responses were that students conduct exams in the clinic (96.2%), participate in the operating room, rather than just observe (94.3%), conduct procedures in the hospital, such as Foley placement (86.8%), and participate in deliveries, rather than just observe (84.9%).
Analyses were performed to find if there was a relationship between student participation in clinical activities and location of the physician’s practice. Providers who teach students in a suburban area were significantly more likely than those in urban or rural areas to report that those students participate in deliveries rather than just observe (χ2 = 8.35, P = .015). In addition, respondents who train students in rural areas were more likely than those in urban or suburban areas to report that students conduct procedures in the hospital (χ2 = 7.936, P = .019). Further information about clinical teaching provided to students can be found in Table 2.
Clinical Teaching: Student Participation.
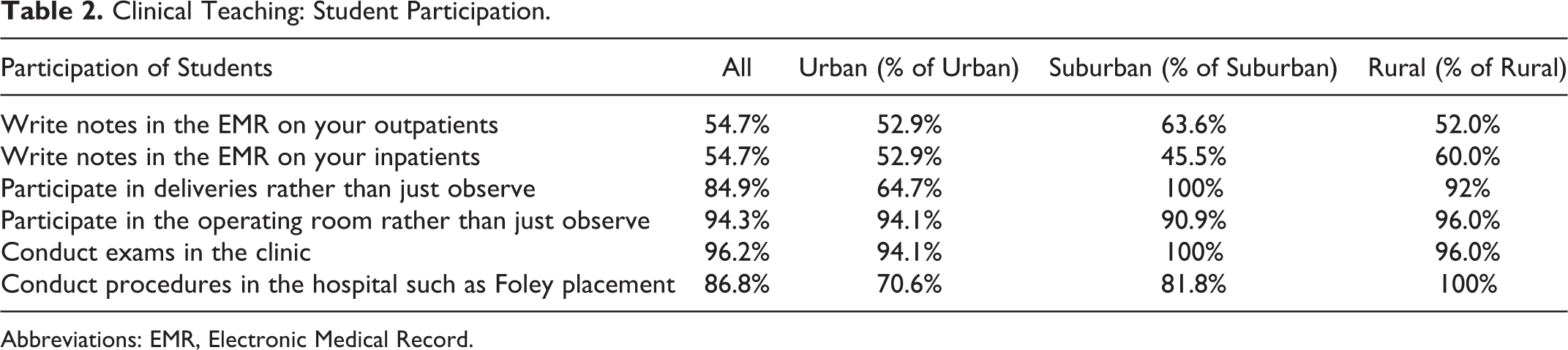
Abbreviations: EMR, Electronic Medical Record.
Challenges and Rewards of Teaching Medical Students
A series of questions on the survey asked respondents to rate whether various aspects of teaching medical students were challenging or rewarding. The most challenging aspects of teaching were reported to be student/workload (63.6%), flexible schedule (45.3%), impact on patient care (44.6%), reduced reimbursement (40.0%), and limited resources (37.0%). The most rewarding aspects of teaching medical students were reported to be intellectual stimulation (90.9%), continuing the tradition of medical teaching (87.5%), intrinsic satisfaction of teaching (83.6%), creates sense of pride in medicine (83.3%), and giving back to the medical community (80.4%).
Younger respondents (those born after 1951) more often viewed the intellectual stimulation of student teaching as rewarding (χ2 = 10.432, P = .034). There were no differences between the location of the respondent’s practice and the aspects of teaching the respondents found to be challenging or rewarding.
Discussion
During the decline in rural obstetrics facilities in the last 10 years, 7 the UWSOM has found it increasingly difficult to identify and cultivate OB-GYN providers in particular, who are willing to share their clinical experience with medical students. In 2011, the UW OB-GYN department was able to provide 10% more training sites than necessary; however, in the last 5 to 6 years, that surplus has steadily declined to a shortfall of 5.6% (personal observation, M.F.F.). This observation prompted our interest in trying to identify what encourages and discourages our clinic to continue teaching. Our results show that providers who teach have students who are actively participating in various aspects of clinical work, while most hospitals encourage student participation in caring for patients. In addition, we are encouraged that much of this group of active teachers continue to find the intellectual stimulation, the tradition of teaching, and its intrinsic satisfaction the most rewarding aspects of participating in medical education. Furthermore, we feel fortunate that the impact of student teaching on reimbursement was less often challenging than the workload of teaching, as the latter is far easier to address with the resources of the medical school. Because there is no reasonable replacement for mentored teaching at this point, we feel this pilot data will allow us to better study the impact of more specific interventions for provider participation at the student, mentor, and facility level. 8,9
Inherently, survey studies rely on subjective information from respondents and may be subject to biases that could impact our results. However, because these surveys are confidential, it can be conceived that respondents were able to answer questions candidly with no fear of repercussions for negative responses. Although the response rate was beneficial for our pilot study in observing trends in OB-GYN teaching practices for this population, the small sample could be considered a limitation. Small samples can create difficulties in generalizing results to the larger population, and the margin of error for results may be higher with a more robust sample. In future studies regarding this topic, we would aim for both a higher response rate and a larger sample of participants in order to better understand this population.
Moving forward, we intend to study interventions with our faculty such as online distributed teaching, prerotation simulation, and reduced administrative burden to reduce the challenges of participation. Ideally, more information about the benefits of student teaching at the personal and institutional level will dispel myths and barriers to participation.
Footnotes
Appendix A
Authors’ Note
UW Human Subjects Division Application #51691; exempt under category 2 as determined April 14th, 2016.
Acknowledgments
The authors wish to thank Lauren Stark and Dr Viksa Mendiratta for their contributions to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided in part by Grant UA6MC19010 from the Maternal and Child Health Bureau of the Health Resources and Services Administration.