
Abstract
People with serious mental illness (SMI) have a higher incidence of type 2 diabetes mellitus (T2DM) and shorter life span due to medical health problems. The chronic care model (CCM) has been used to improve care of patients with T2DM. One clinical organization that provided primary care to patients with SMI had excellent diabetes outcomes but did not have information on how they achieved those outcomes. Thus, we conducted a pilot study chart review for 30 patients with T2DM and SMI to determine how well the clinic’s system aligned with the overall CCM components and which components correlated with diabetes control. We also evaluated use of the CCM using the Assessment of Chronic Illness Care provider survey. Results showed that the clinic had an overall basic implementation level of the CCM, which allows opportunity for improvement. Two elements of the CCM were correlated with hemoglobin A1C and both were in an unexpected direction: self-management support in the variable of percentage of visits that included patient-specific goal-setting (rs = .52; P = .004) and delivery system design in the variable of number of nurse practitioner visits per study period (r s = .43; P = .02). These findings suggest that the clinic may have made more concentrated efforts to manage diabetes for patients who were not in good diabetes control. Providers noted the influence of SMI and social service organization support on these patients’ clinical outcomes. The findings will be reexamined after a fuller implementation of the CCM to further improve management in this population.
Introduction
Patients with serious mental illness (SMI) had poorer physical health than the general population and have a life expectancy of 8 to 32 fewer years; most of the mortality is due to medical causes rather than psychiatric. 1 -6 Factors that contribute to decreased life span are lifestyle, metabolic side effects from antipsychotic medications that can lead to diabetes, limited access to health care, and physiologic changes such as inflammation in people with schizophrenia. 2,7,8 People with bipolar disorder and people with schizophrenia have a significantly higher incidence of diabetes. 7
Patients with SMI and type 2 diabetes mellitus (T2DM) frequently lack adherence to diabetes management guidelines compared to patients without SMI, are less educated about diabetes and self-monitoring, and receive less prevention care for cardiovascular disease. 9 -15 Integrating physical and mental health care in patients with SMI and diabetes has resulted in improved health outcomes, including hemoglobin A1C (HbA1C) levels. 13,16 -18
Standards of Medical Care in Diabetes, by the American Diabetes Association, recommend that care for patients with diabetes be aligned with the chronic care model (CCM). 19 The CCM guides health systems to organize to support the patient in managing their chronic illnesses, and it leads to improved outcomes. 20 -22 The CCM has 6 elements: health system, delivery system design, self-management support, decision support, clinical information systems, and community linkages. 20 Implementing the CCM in settings with patients with diabetes has resulted in improved diabetes indicators, including lower A1C. 23 -25 Implementation of the CCM in a population of people with mental illness has been shown to be effective in improving mental health indicators. 26 However, studies are lacking in evaluating the CCM for people with both SMI and diabetes.
Project Aims
The aims of this project were to determine, within the setting of an urban federally qualified health center (FQHC) that provides primary care to patients with SMI, among patients with SMI and diabetes: (1) how well the clinic’s system aligned with the overall CCM components, (2) which components of the CCM were associated with diabetes control, and (3) any additional factors outside of the CCM that may have contributed to patient outcomes.
Methods
Setting
The site of this study was an FQHC providing primary care to patients, most of whom had a documented SMI. Federally qualified health centers, a designation given to organizations receiving grants under the Public Health Service Act, qualify for enhanced reimbursement. 27 The organization consisted of 3 clinics; all providers were nurse practitioners (NPs). The clinic worked closely with a local social service organization to coordinate care. 28 This FQHC clinic received an award for their excellent diabetes outcomes in 2010 from a state-level agency and consistently surpassed diabetes goals for A1C and cholesterol as set forth in Healthy People 2020 (D. Cesarone, MS, RN, personal communication, April 10, 2015). 29 However, information is lacking about which clinical organizational elements contributed to these outcomes.
Sample
We examined the charts of persons who met the following inclusion criteria: SMI, T2DM as determined by billing codes, and at least 1 clinic visit in the study time period. The electronic medical record (EMR) identified 47 unduplicated patients with a diagnosis of T2DM seen in the month of July 2014 from 2 clinics (the third had only recently opened and was not included in the study). Thirty randomly sampled patient’s EMR numbers were obtained from those reports; those charts were evaluated using the chart abstraction tool for July 1, 2014, to June 30, 2015, in accordance with Joint Commission sampling guidelines. 30 A request to complete the provider survey was made to all providers (NPs) across the clinical organization.
Measurement Tools
We used a provider survey and a chart review. The survey used was the Assessment of Chronic Illness Care (ACIC) survey, version 3.5. 22 One additional question was added: “Are there any additional factors that may impact patient outcomes for this population?” This question allowed respondents to provide additional insight on issues that may not have been captured with the ACIC survey.
The ACIC surveys were scored in accordance with guidelines, resulting in a score for each of the 6 CCM elements. 22 Scores could range from 0 to 11: 0 to 2, limited support; 3 to 5, basic support; 6 to 8, reasonably good support; 9 to 11, fully developed support. 22
We used a chart abstraction tool (see Table 1) that was investigator-designed and adapted from 2 sources: an example chart abstraction tool by RAND Health to measure the use of the CCM with patients who have diabetes and a measurement tool from a RAND Health study that used multiple sources of clinic data to assess organizations’ implementation of the CCM (note 1). 31,32 The chart abstraction tool included questions targeted to assess the different elements of the CCM. All abstracted data from the charts pertained to individual patients, and data were entered into an Excel database with 1 line for each of the 30 patients. The patient was the unit of analysis, and the data were not aggregated by clinic.
Chart Abstraction Tool Content.
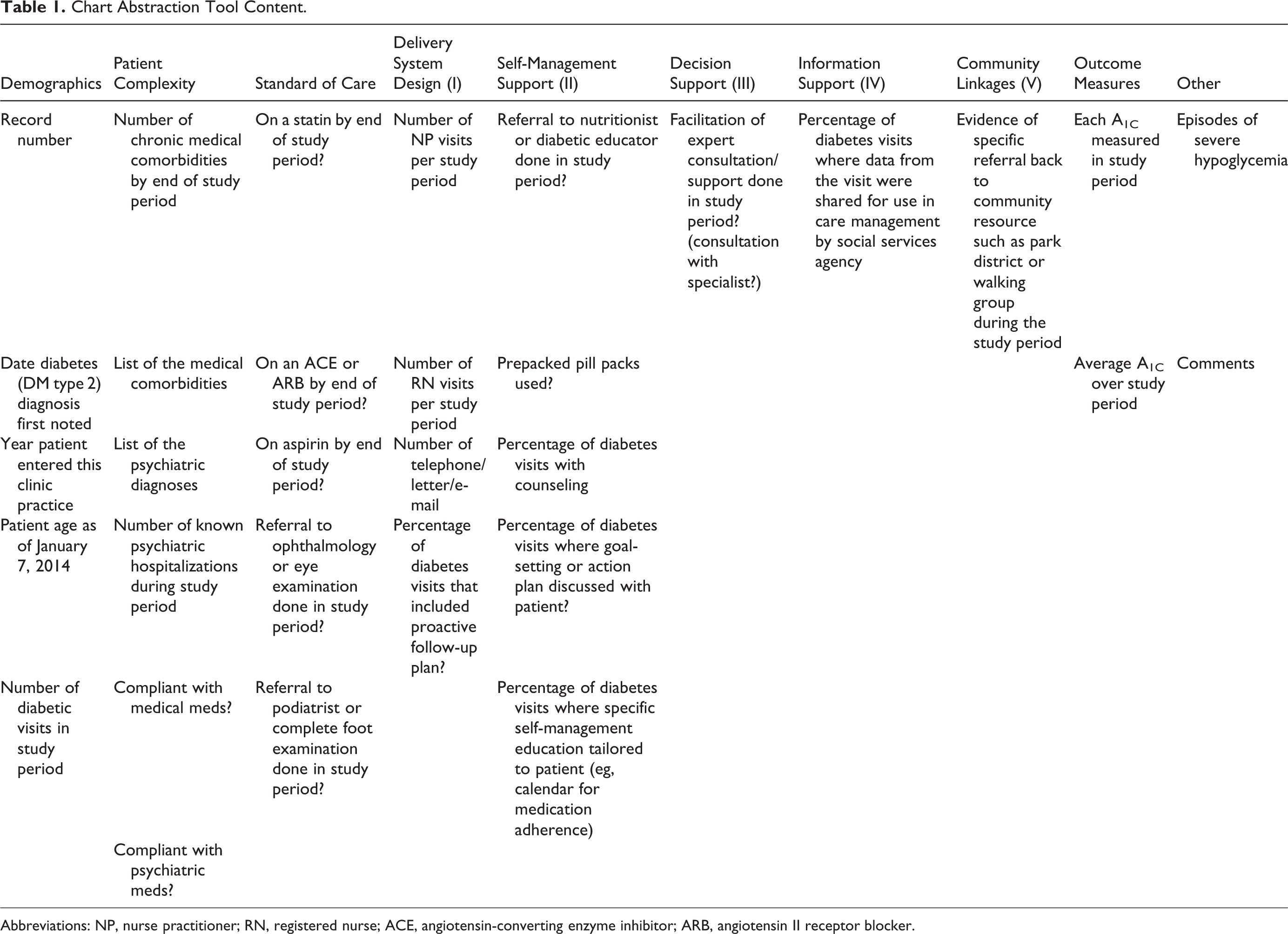
Abbreviations: NP, nurse practitioner; RN, registered nurse; ACE, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker.
Statistics
Descriptive statistics were used to summarize information from the chart review and provider surveys (Excel, SPSS version 22). Means and standard deviations were used for normally distributed variables and medians for nonnormally distributed variables. Variables in the chart review that represented components of the CCM were evaluated for correlation with average A1C result from July 1, 2014, to June 30, 2015. For numerical variables, Spearman correlation coefficient was used to test for associations among A1C and the CCM variables to account for nonnormally distributed data and small sample size. For categorical variables, a t test was used for differences between means.
Research Approval
Institutional review board approval and research council approval were obtained prior to data collection.
Results
The chart review examined 30 charts of patients with SMI and T2DM. The mean age was 52.7 (10.57) years , and ages ranged from 26 to 59 years. On average, there were 5.63 (3.23) diabetes visits in the study period, and the number of visits ranged from 0 to 15 (see Table 2).
Descriptive Statistics.

Abbreviations: NP, nurse practitioner; RN, registered nurse; SD, standard deviation.
Four providers (80% of eligible providers) completed the ACIC provider survey, and the overall mean score was 5.19, indicating basic support for chronic illness care. Two survey respondents answered the question “Are there any additional factors that may impact patient outcomes for this population?” One comment was about the noncompliance of patients with SMI and how that may negatively impact outcomes; the other was on the support received from the social service organization for the patients and how that may positively impact outcomes.
Table 2 shows the CCM variables evaluated from the chart review and which ones had a strong presence in this clinic. There was a significant positive correlation between higher A1C and higher number of NP visits during the study period (r s = .43, P = .02). There was also a significant positive correlation between higher A1C and patient records with a higher percentage of visits where goal-setting or action plan was developed (r s = .52, P = .004). There were no other statistically significant findings between CCM elements and A1C (Table 3).
Analysis of Chart Review CCM Variables and Correlation With A1C.

Abbreviations: CCM, chronic care model; NP, nurse practitioners; RN, registered nurse; DF, degrees of freedom.
Discussion
The 4 ACIC survey responses revealed only basic-level support for chronic illness care, a score often seen with a clinic that has not yet started implementation of the CCM model, suggesting much room for improvement. 32 The score results for each of the 6 CCM elements were as follows: Health System 6.78, Delivery System Design 5.27, Self-Management Support 5.68, Decision Support 5.38, Clinical Information Systems 2.90, and Community Linkages 6.67. Comments from providers show that connection with the social services agency may have contributed to patient outcomes.
Health System
The health system element was measured in the provider survey, not the chart review, due to its global nature. This concept includes visible support for improvement by senior leadership, improvement strategies, and a systematic way to address problems. The survey was completed during a time of transition for the clinical organization marked by high staff and leadership turnover, which may have affected the score.
Delivery System Design
The delivery system design element includes coordination across specialties, clear division of labor among the health-care team, inclusion of all team members to improve outcomes, and strong leadership in clinical practice. The positive correlation of the number of NP visits with A1C was unexpected. Possibly, patients were asked to follow up more often when providers noted the diabetes was not well controlled. Although no other variables in this element were associated with A1C, the number of phone calls had a wide range, including 1 patient with 71 calls in the study period. The chart review revealed times of frequent communication when the patient needed extra support around diabetes management. There were no registered nurse (RN) visits during this study period. It is noteworthy that there was not an RN at all clinical sites in the organization at the time of the provider survey. The delivery system in the clinics had strength in the increased visits with the NP when needed but possible weakness in the areas of inclusion and utilization of all of the health-care team.
Self-Management Support
This element includes having trained educators in empowerment and problem-solving, behavior change interventions, and peer support for self-management. The findings suggest a need for these interventions to be formally implemented. There was an unexpected statistically significant positive association between percentage of diabetes visits where specific goal-setting or action plan was discussed with the patient and A1C. Possibly, as A1C increased, NPs used skills of motivating the patient, including helping the patient set a specific goal. Most patients used prepared pill packs, but there was no statistically significant difference between A1C of those who did and those who did not. Most visits included patient education, but fewer used goal-setting and self-management education. The clinic has a routine procedure to print patient education, but no specific procedure about setting goals or providing self-management education.
Decision Support
Decision support includes facilitation of expert consultation by the provider, which occurred at least once within the study period in only 13.3% of patient charts, and there was no association between this variable and A1C. Decision support also includes integrating diabetes management guidelines into the EMR and educating patients about guidelines, neither of which was a formal part of the clinic routine. This suggests consultation and guideline inclusion need improvement.
Clinical Information Systems
The chart review found that on average 89% of each patients’ diabetes visits included communication to the patient’s social service organization regarding the visit. This variable did not correlate with average A1C, possibly because it is done so often in this clinic as part of the process of care. The clinic did not have the following recommended systems: a registry of patients with diabetes that uses prompts and reminders connected to guidelines, feedback by a team leader, or patient treatment plans.
Community Linkages
The chart review showed that 16.6% of patients received a referral back to a community resource within the study period, such as the local park district or social service organization’s walking group, and this variable did not correlate with A1C. This is a possible area for improvement.
Limitations
This pilot study was limited by the small sample size and lack of comparison group. Additional studies need a larger sample size and a comparison group of patients from a different clinic. Also the results of association do not imply causation.
Recommendations
Based on our chart review, we recommend improvement in the following areas: a standardized way of addressing systems problems, a clear division of labor and inclusion of all members of the health-care team, building EMR alerts in accordance with diabetes guidelines, and protocols for individualized goal-setting and self-management education.
To improve diabetes care for people with SMI, we recommend first evaluating current care patterns and then planning changes based on results within the framework of the CCM. We recommend that a follow-up study be done after full implementation of the CCM in this clinical organization.
Footnotes
Acknowledgments
The authors would like to acknowledge Kevin Grandfield for his editing of this article, Robyn Nisi for her technical assistance, and Colleen Corte for her suggestions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to acknowledge the Research Open Access Article Publishing (ROAAP) Fund of the University of Illinois at Chicago for financial support towards the open access publishing fee for this article.