
Abstract
Objectives:
Whether traffic remoteness from health care service in rural areas influences usage of ambulance service has not been well investigated. This study aimed to evaluate the relation between remoteness to health care facilities and incidence of ambulance calls in rural areas of Japan.
Methods:
We analyzed 155 rural communities of Hiroshima. Data were obtained on all ambulance dispatches from 2010 to 2012. Driving time was calculated from each community to the closest primary/secondary and tertiary health care facility (equivalent to tertiary emergency care centers). We estimated the incidence rate and the incidence rate ratio (IRR) of ambulance calls for each 10-minute increase in the driving time, using generalized log-linear regression models, and evaluated the effect among each specific subgroup of emergency level and season.
Results:
During the study period, the median incidence rate was 436 per 10 000 people in targeted communities. When driving time to the closest primary/secondary facility increased by an increment of 10 minutes, there was a significant increase in the IRR of ambulance calls, especially during colder seasons (IRR: 1.29 [95% confidence interval: 1.11-1.49]), and this relation was also obtained for most emergency levels. In comparison, there was no such increase in IRRs observed for driving time to a tertiary facility.
Conclusion:
This study indicated a positive association between remoteness to primary/secondary medical facilities and the frequency of ambulance calls. The remoteness to a primary/secondary health care may induce an increase in ambulance calls, particularly during cold seasons.
Introduction
Geography plays an important role in access to health care services and potentially affects health care. 1 For example, residents who are remote to health care services had a higher mortality rate when they were dialysis patients, 2,3 infants, 4 or those with asthma 5 compared to residents who were close to services. The negative impact of distance to a health care facility on health may be caused by the distance-decay effect on health care use. This effect has been reported in the United Kingdom, 6 –9 Canada, 8,10 and some African countries. 11 –13
The utilization of ambulance services, however, has not been closely examined in its association with distance to care facilities. It is possible that people who do not receive sufficient daily care due to the remoteness to the care are likely to allow their condition to worsen and subsequently need to call an ambulance. There are no studies that have examined this assumption, except for one US study showing a positive association between accessibility to primary care and use rate of emergency rooms among children. 14
Japan is particularly suited to studying the assumed association between distance and ambulance use because ambulance transportation in Japan is free of charge at any time and for any severity of illness. 15 As such, excessive use of ambulance services is likely to take place. Further, it is politically important to know how distance affects the use of ambulance services. We evaluated the association between distance to the closest health care facility classified according to its function and incidence of ambulance calls in rural areas of Japan.
Method
Study Area and Participants
We selected rural communities in Hiroshima Prefecture, which had the second largest number of designated nonphysician communities in Japan. Details on these designated communities have been described elsewhere. 16 –18 The latest data on nonphysician communities were obtained from the Ministry of Health, Labour and Welfare. 19 The 2010 National Population Census was utilized to describe area-based characteristics.
First, we selected 11 municipalities in Hiroshima, which had at least 1 nonphysician community. Among them, we selected 155 rural communities comprised of 57 710 persons in 2010, including nonphysician communities (n = 78), adjacent communities to nonphysician communities (n = 48), and municipal centers (n = 29). Selected communities are shown in Figure 1, and the definitions for adjacent communities have been provided elsewhere. 18 The smallest census block (“community”), which is a basic unit that composes a municipality (city, town, or village), was adopted as the geographic unit in this study. The centroid point of a census block was adopted as the representative point of the community in the analyses.
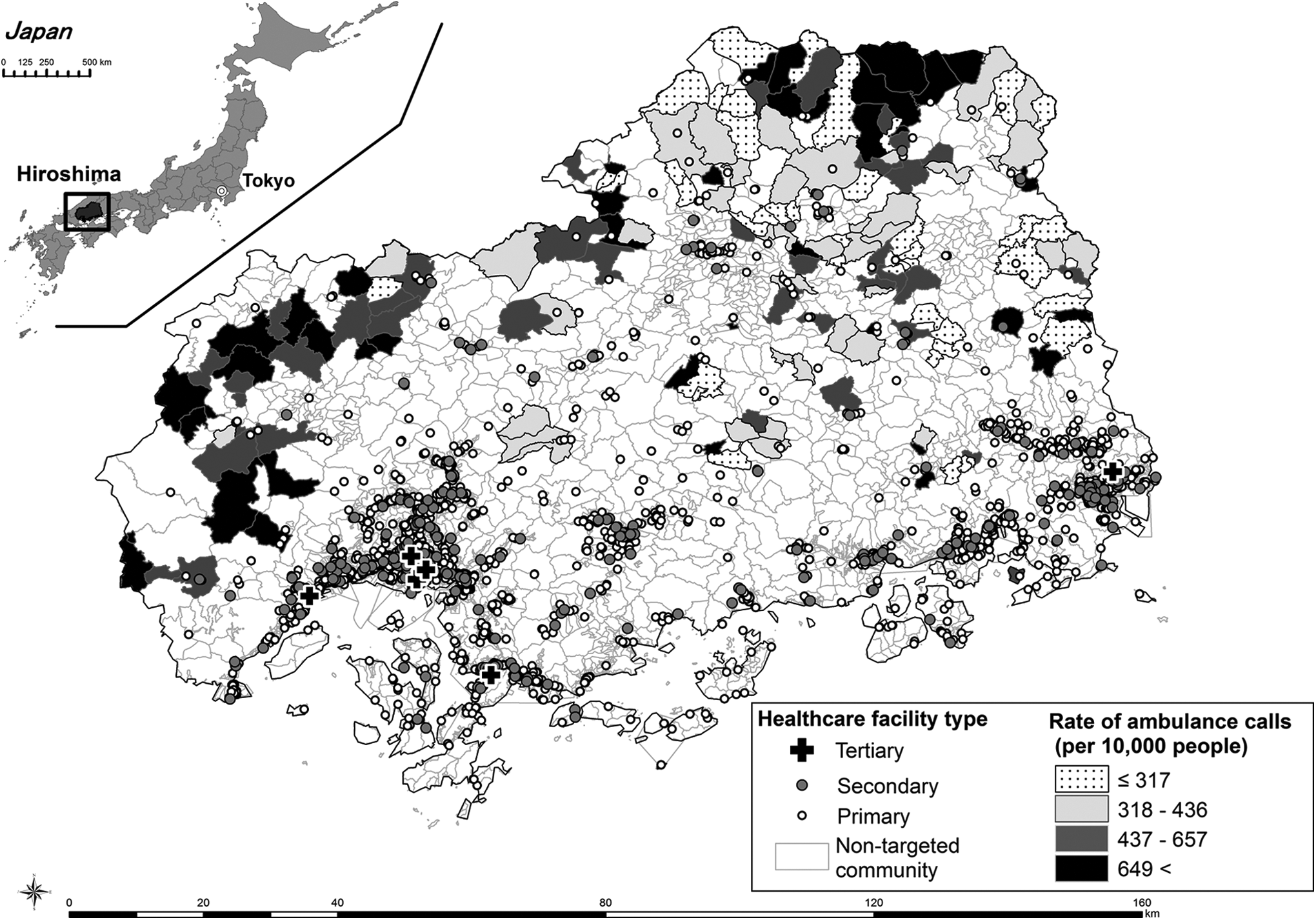
Distribution of health care facilities in Hiroshima prefecture and rates of ambulance calls per 10 000 people at target communities. The ambulance rate was classified by quartile points.
Health Care Facility
A list of all health care facilities with inpatient beds was obtained from the Bureau of Health and Welfare Affairs, Hiroshima Prefectural Government. We classified these health care facilities into the following 2 types: primary and secondary care facilities providing general health care, and tertiary care facilities (equivalent to tertiary emergency care centers) providing specialized health care. Since only 33 communities had primary/secondary facilities (total 62 facilities) among target communities, we used all primary/secondary facilities (2636) and tertiary facilities (6) in Hiroshima prefecture for measuring accessibility.
Measuring Accessibility
We measured driving time by car from each community to the closest health care facility. The computation process included network analysis (ie, determining the shortest driving path between 2 locations on a road network, including highways) using ArcGIS version 10.0 and ArcGIS Data Collection Road Network 2011 (ESRI Japan Inc).
Emergency Ambulance Calls
Anonymized electronic data on all emergency ambulance calls between January 2010 and December 2012 were obtained from all 9 ambulance divisions in the prefecture. According to classifications by the Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications, these emergency events were classified into 5 categories by health severity level at the first medical examination: “deceased” when a person is diagnosed as deceased; “critical” when a person faces a life-threatening hazardous condition such as cardiopulmonary arrest; “severe” when a person has a possibility of facing a life-threatening condition but cannot be defined as critical or deceased; “moderate” when a person needs hospital admission but is not in a critical or severe condition; and “mild” when a person did not require hospital admission. We also classified the data into 2 seasons according to local climate: a cold season (fall and winter) between October and March and a warm/hot season (spring and summer) between April and September as accessibility to care facilities potentially changes between the 2 seasons due to winter snowfall on roads.
Statistical Analysis
First, the incidence rate of ambulance calls per 10 000 people at each targeted community was calculated. Then, we estimated the incidence rate ratio (IRR) 20 of ambulance calls for each 10-minute increase in driving time to the closest health care facility of either type (primary/secondary or tertiary) using generalized log-linear regression models. 21 In addition, to determine whether the effect of driving time was influenced by emergency level or season, we stratified the ambulance call events according to emergency levels and seasons and examined the association between driving time and incidence of ambulance calls. The IRR shows a multiplicative change in incidence of ambulance transportation with each 10-minute increase in driving time. For example, IRR 2.0 indicates that the number of emergency calls increases by 2-fold for each 10-minute increase in driving time from the community. Confidence intervals (CIs) were estimated at the 95% level in all analysis. 22 Analysis was done with SPSS software (IBM Inc, version 22 J).
Ethical Considerations
This study was approved as a study to be conducted without individual informed consent by the Ethics Committee of Epidemiological Research, Hiroshima University (No. 779).
Results
There were a total of 8646 emergency ambulance calls from the 155 rural communities during the study sample period. Table 1 shows community geographic and demographic characteristics and emergency ambulance call rates. The mean percentage of elderly people was 45% among those in the study areas, which was higher than the prefectural mean (24%). The median for driving time to a tertiary facility was far longer than that to primary/secondary facilities. The median rate for ambulance calls, which contained all levels of emergency in each community, was 436 per 10 000 persons. Mild and moderate levels occupied more than 80% of the total dispatches when stratified by emergency level. There was no statistical difference in the median rate of emergency dispatches between a cold (fall and winter) and warm/hot (spring and summer) seasons (P = .537, Mann-Whitney U test). The scatter plots for ambulance call incidence rates against distance to closest facility are shown in supplemental Figure 1. Two communities had higher IRRs than others and had small populations (13 and 20 persons).
Basic Characteristics (2010) and Rates of Ambulance Calls per 10 000 people From the 155 Communities During 2010 and 2012 in Hiroshima, Japan.

Abbreviations: interquartile range, 25th and 75th percentile; SD, standard deviation.
aData of household and population was as of 2010.
bOne island community was omitted because transport by ship was needed.
cThere are 3 calls with unknown level of accident and sickness level.
The rates of ambulance calls per 10 000 people at the 155 communities were classified by quartile points in Figure 1. In general, the 155 rural communities were predominantly located in northern mountainous areas, which were more rural than coastal areas of the south.
Table 2 shows the IRRs of ambulance calls per 10-minute increase in driving time to the closest health care facility. Positive associations were observed between an incidence rate and driving time to the closest primary/secondary facility in any level of emergency except for severe level. Particularly, the incidence had a significant and positive association with driving time at 2 emergency levels: IRR 1.85 (95% CI: 1.27-2.69) for a critical level and 1.80 (95% CI: 1.19-2.72) for a deceased level. In contrast, a negative association was observed between the incidence rate and driving time to a tertiary facility at a severe emergency level (IRR 0.70 [95% CI: 0.48-1.01]).
Incidence Rate Ratio of Ambulance Callsa Per 10 Minutes Increase in Travel Time to a Closest Health Care Facility Among the 155 Rural Communities.

Abbreviations: CI, confidence interval; IRR, incidence rate ratio; NA, not available.
aThe incidence rate ratio for emergency ambulance calls was calculated and increased by 100 people per 10 000 people in mean travel time to the closest health care facility.
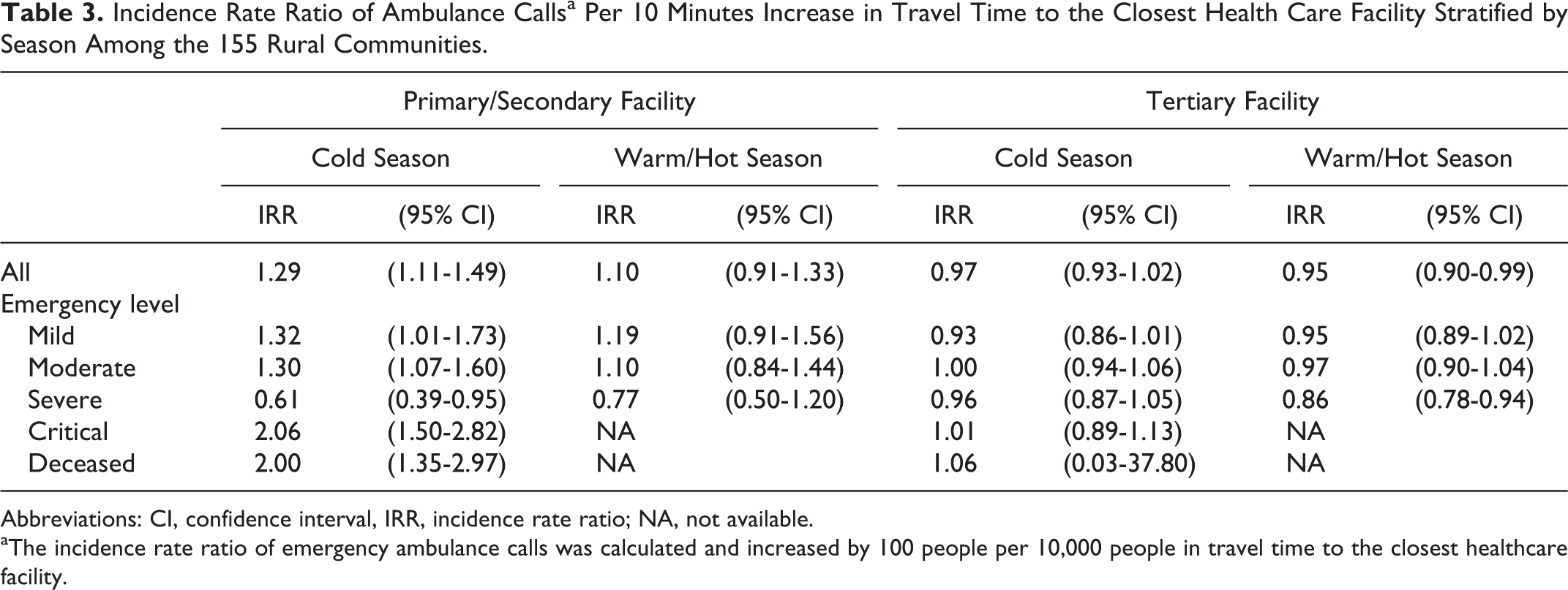
Table 3 shows the results of the subgroup analysis stratified by seasons. A significant increase in the ambulance call rate with an increase in driving time to the closest primary/secondary facility was observed in the cold season (IRR: 1.29 [95% CI: 1.11-1.49]). These significant associations were also observed among most emergency-level subgroups except for severe level in a cold season. In comparison, there was no significant association observed in the warm/hot season. A positive association was not observed between the ambulance call rate and driving time to the tertiary facility in both cold and warm/hot season at any level.
Incidence Rate Ratio of Ambulance Callsa Per 10 Minutes Increase in Travel Time to the Closest Health Care Facility Stratified by Season Among the 155 Rural Communities.
Abbreviations: CI, confidence interval, IRR, incidence rate ratio; NA, not available.
aThe incidence rate ratio of emergency ambulance calls was calculated and increased by 100 people per 10,000 people in travel time to the closest healthcare facility.
Discussion
Ambulance call incidence rate was positively associated with a longer distance to a primary/secondary facility at some particular levels of emergency. This association was more prominent in the cold season than in the warm/hot season. In contrast, there was no such positive association observed between the ambulance call rate and the distance to tertiary facilities.
This finding is consistent with the results of a US study, in which children who lived in remote areas from primary care providers utilized an emergency department more frequently in comparison to those who lived in areas closer to such health care facilities. 14 Two factors may be proposed for this finding. First, a geographic barrier to accessing primary care services might inhibit early intervention of diseases, allowing disease progression and resulting in more ambulance calls. Primary care potentially protects against unnecessary hospitalizations. 23 In this study, an increase in ambulance calls was observed for patients with critical health levels and for those who had died in areas remote from primary/secondary care facilities. Thus having nearby accessible primary/secondary facilities may protect residents from excessive use of ambulance services. Second, persons who live in areas remote from primary care services may have an economic and time incentive to use ambulances. The utilization of medical facilities reportedly decreases with an increase in distance to facilities. 6,7,10 As mentioned, ambulance services are free of charge in Japan. 15 This context may mean that remote persons have an economic incentive to use ambulances as compared with their urban counterparts. Also, the long distance between a person’s home to a health care facility may encourage rural residents to use ambulances because the time benefit gained from using ambulances is greater in a rural than in urban areas.
In the stratified analysis by season, a distance effect was observed more obviously in the cold than in the warm/hot season. According to an official report on ambulance use in Japan, the proportion of diseases among all emergency ambulance calls was 18.7% for cardiovascular, 10.2% for gastrointestinal, and 9.3% for respiratory diseases. 24 A positive association was reported between a low ambient temperature and the incidence of cardiovascular diseases or hot weather and respiratory diseases. 25,26 Thus during the cold season, the morbidities of some cold-related diseases might have increased and consequently ambulance calls also increased in rural areas.
Among the 155 communities in this study, about 70% were classified as a medium snowfall area and 21% of these were an extremely heavy snowfall area. Snow blocks road transportation and makes driving difficult, particularly for elderly people. As such, it is possible that people in snowy rural areas tend to use ambulances instead of their own cars in the winter season.
The high percentage of elderly people in remote areas from primary/secondary facility should be mentioned. The percentage was highly correlated to driving time to primary/secondary facility (R = .51, P < .01). This phenomenon could modify the effect of distance on increased number of ambulance calls, since elderly people tend to lack private-car transport. In Japan, rural areas have rapidly aging populations. 27 Accordingly, health policy should consider contextual factors such as age demographics as well as remoteness to a health facility.
There were some limitations in this study. First, we did not obtain individual information for each record of an ambulance call. Thus, we could not evaluate the effects of multiple ambulance calls by the same person. Second, there were a few negative associations at the severe level, which were opposite to the other emergency levels and did not support our research hypothesis. Although the significance was marginal, we were not able to address whether or not this negative association was a chance finding.
In conclusion, our study addressed a contemporary issue in Japan around ambulance services. The results indicated that remoteness to a primary/secondary care is a key factor that increases ambulance calls in rural areas. To maintain the use of ambulance services at a moderate level, it appears important to improve rural community accessibility to primary/secondary care facilities.
Footnotes
Acknowledgments
We thank Dr Takashi Yorifuji for his valuable input on our study design. The authors would like to appreciate the assistance from the staff of the Health and Welfare Affairs Bureau, Hiroshima Prefectural Government, in providing the health care facilities data, and the Ambulance Division of the city’s Fire Bureaus in Hiroshima in providing the ambulance data. The software used in this study was supplied by the Higher Education Grant Program of ESRI Japan Corp (Tokyo, Japan).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the 21st (2012) Joint Research Project of the Pfizer Health Research Foundation (12-8-075) and investigation research (2014) of the Conference for Emergency Medicine in Rural Areas and Isolated Islands.