
Abstract
Background:
A patient’s health literacy is not routinely assessed during visits with a health care provider. Since low health literacy is a risk factor for poor health outcomes, assessing health literacy should be considered as part of the standard medical workup.
Objectives:
To evaluate the health literacy levels and medication adherence of patients treated by pharmacists in both the general medicine and the chronic care clinics at an urban free health clinic.
Methods:
Eligible patients from the free health clinic completed the Rapid Estimate of Adult Literacy in Medicine (REALM), a health literacy measurement tool, during their clinic visit in 2011. Medication adherence was self-reported by the patients.
Results:
A total of 100 patients participated (mean age = 48). The majority of participants were female (56%) and white (55%). Most (64%) of the patients scored at a high school reading level according to REALM. Only 21% of participants read at a seventh- to eighth-grade level. Overall medication adherence rate was 73%. Forgetting to take medication was the most popular reason given for nonadherence.
Conclusion:
Disease state and adherence were significantly related in patients with HIV/AIDS and hypertension. Patient’s ethnicity was significantly associated with literacy levels (P < .05). Although patients’ literacy levels were not significantly associated with self-reported adherence in this population, availability of a patient’s baseline health literacy level as a part of the medical record may help clinicians to individualize their interaction based on the patient’s health literacy level in order to achieve better health outcomes, including improved medication adherence, especially for underserved populations.
Introduction
By definition, health literacy is defined as “the degree to which an individual has the capacity to obtain, communicate, process, and understand basic health information and services to make appropriate health decisions.”(http://www.cdc.gov/healthliteracy/learn/index.html) 1 –3 Results from prior studies provide evidence that patients’ health literacy has a significant impact on the extent of a patients’ medication adherence 4 –17 and related health care utilization. 18 –20
Adherence can be broadly defined as a patient’s ability to accurately follow a prescribed treatment regimen. 21 In research, this is often operationalized as the patient’s ability to successfully take the prescribed number of doses of a medication. A common metric of defining adherence is taking at least 90% of the prescribed doses. 22 –24 The annual excess of health care costs as a result of medication nonadherence is roughly US$290 billion in the United States. 25 By understanding barriers to adherence, clinicians can help patients become more adherent in managing chronic disease that can alleviate these costs.
Between 30 and 34 million American adults fall into the lowest of the 4 levels of health literacy (“below basic,” “basic,” “intermediate,” and “proficient”), according to results from the 2003 National Assessment of Adult Literacy. 26 Even adults with proficient levels of general literacy may have low health literacy due to the stressful nature of health care visits and unfamiliar medical terminology. In a systematic review of literature examining health literacy prevalence rates, up to 50% of US adults were determined to have low health literacy, while approximately 33% of Medicare enrollees have low or inadequate health literacy. 27,28 However, it is difficult to accurately determine the national prevalence of low health literacy due to different definitions and measurements used across the studies. 29,30
It has been suggested that patients with low health literacy experience a higher rate of medication errors. 2 Standard medication guides approved by the Food and Drug Administration have been estimated to require a 10th- to 11th-grade reading level, leaving many patients with a poor understanding of the content. 31 One study by Davis et al found that patients in primary care settings who had low literacy were 3 times less likely to correctly interpret medication label warnings. 32 Another study by the same authors found that low literacy was associated with misunderstanding medication labels, and only 35% of patients with low literacy could correctly identify how many pills needed to be taken daily. 33 Several studies have reported that health literacy levels may predict medication adherence. 34,35
Counseling patients with low health literacy levels can be a great challenge. Often, these patients do not fully comprehend the benefits and risks of medications or how adherence affects health outcomes.2, 36 Therefore, medical providers can make use of a patient’s health literacy to assist patients in understanding their treatment plans. 2,37 When only 12% of adults in the United States are considered health literate, clinicians must acknowledge an opportunity to improve patient outcomes. 2 Therefore, the objective of this study is to evaluate the health literacy levels and medication adherence of patients treated by pharmacists in both the general medicine and the chronic care clinics at the Kansas City Free Health Clinic (KCFHC).
Materials and Methods
Study Design
The study was conducted by pharmacists at the KCFHC, an urban free health clinic in Kansas City, Missouri. The study estimated health literacy levels and medication adherence of patients in both the general medicine and the chronic care clinics. Rapid Estimate of Adult Literacy in Medicine (REALM) was chosen for its ease of use and short administration and scoring time. In order to be eligible for this study, patients had to be 18 to 65 years old, English speaking, and currently receiving medical care at the KCFHC in 2011. Patients were excluded if their current health condition was so poor that it inhibited normal patient–provider communication.
Measures
Level of health literacy was assessed using The REALM. The REALM is a tool used to identify individuals’ health literacy levels. 38 The entire REALM can be administered and scored in less than 5 minutes, which is convenient for many health care settings. 38 The REALM can also help practitioners identify those patients who have compensated for their literacy deficiencies by requesting patients to pronounce 66 words that may be used during a medical visit with a health care provider. 38 As this is a word recognition test, it is intended to screen patients rapidly and provide an estimate of their literacy levels, rather than testing comprehension or diagnosing specific reading deficits or learning disabilities. 38 The results of REALM are broken down into the following reading level categories: below third grade, fourth to fifth grade, seventh to eighth grade, and high school. 38
Medication Adherence
Adherence was assessed using patients’ self-reported data. Patients were asked by the pharmacists on how many medication doses they had missed in the last 3, 7, and 14 days prior to their clinic visit. If any doses were missed, patients were asked to volunteer reasons why this had occurred. Medication adherence rate (MAR) was calculated by dividing the number of doses taken in 14 days by the total number of doses available. This calculation was adjusted for each patient’s dosing schedule; for instance, if a medication was prescribed to be taken twice daily, then the total number of doses available in 14 days was 28. Patients with an MAR ≥90% were categorized as “adherent,” and patients with an MAR less than 90% were categorized as “nonadherent.” Medication adherence barriers were collected by the pharmacist using open-ended questions and emphasized with the probe “what else” to gather all possible medication adherence barriers experienced by these underserved patients.
Data Collection
Participant recruitment and data collection occurred from September 2011 through November 2011. Patients who came to the general medicine clinic were recruited after the patient had been checked into their room and before their examination with their provider. If the patient agreed, the investigator read the institutional review board-approved consent script describing the nature of the research and the REALM process. Participation in this study was voluntary and did not affect the quality of medical care that the patient would receive.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 20. Descriptive data were gathered for demographic and clinical characteristics of the sample. Adherence was entered as a dichotomous variable, whereby 1 = MAR ≥ 90% and 0 = MAR < 90%. Multivariate logistic models determined associations between adherence, health literacy level, and patient characteristics. Models were adjusted for age, gender, ethnicity, and education. Results were reported in estimated proportion (%) and odds ratio (OR) with 95% confidence intervals (CI).
Results
A total of 100 patients were selected to perform the REALM. The average patients’ age was 48 (range 20-66), and majority was female (56%) and white (55%). Additional demographic and clinical characteristics of the sample are provided in Table 1. There was a significant association between ethnicity and reading level (P = .002). White patients displayed higher literacy levels compared to black patients in the bivariate analysis (Table 1). While 33% of patients reported completion of their high school degree, 64% scored as much according to the REALM. Conversely, 36% of patients could not read at a high school level. In this study, only 21% of patients read at a seventh- to eighth-grade level, which is currently the average American adult literacy level. 3 It is unknown at this time why this discrepancy exists, but with a larger sample size, results may prove representative of the US population.
Demographic Characteristics of the Sample and Health Literacy Level.a
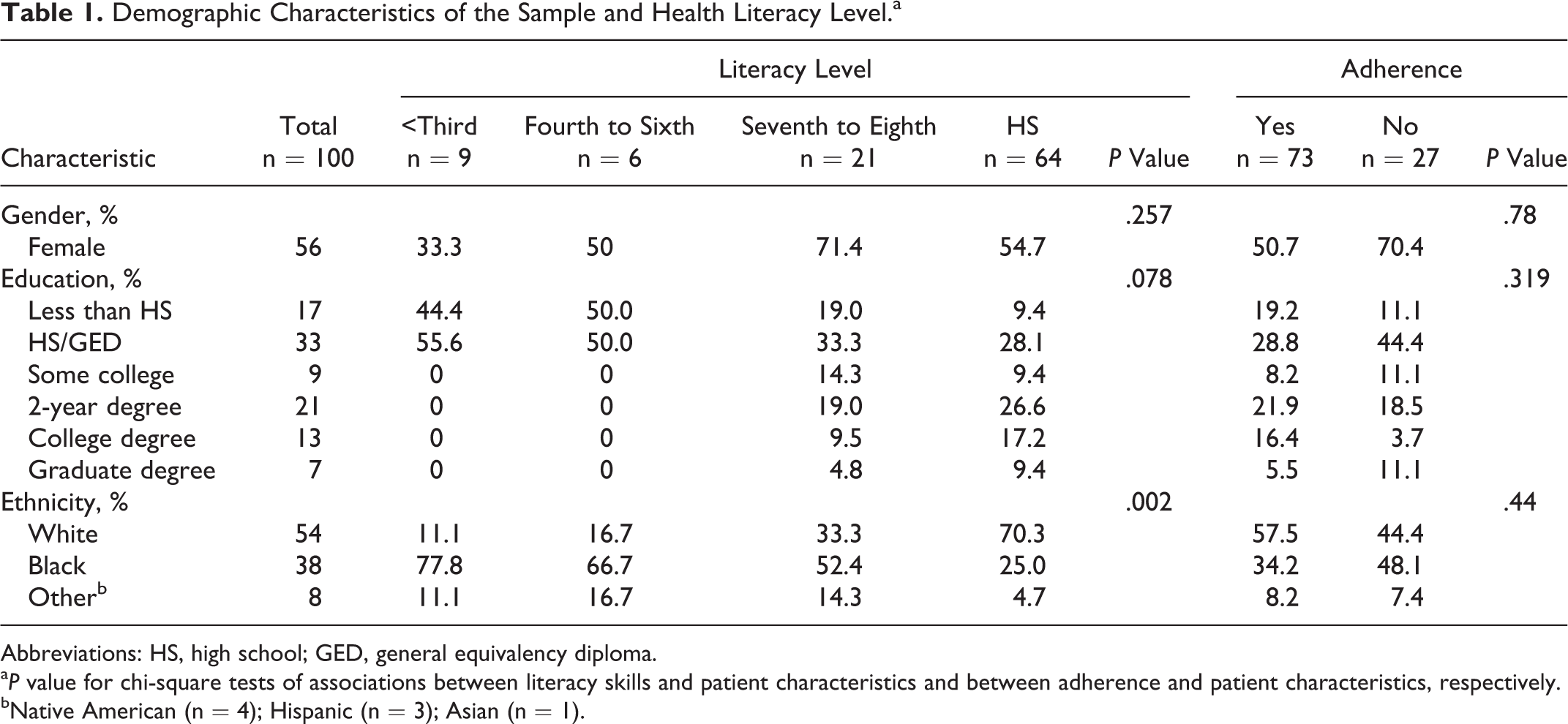
Abbreviations: HS, high school; GED, general equivalency diploma.
a P value for chi-square tests of associations between literacy skills and patient characteristics and between adherence and patient characteristics, respectively.
bNative American (n = 4); Hispanic (n = 3); Asian (n = 1).
Overall, 73% of participants were adherent to their medication regimen. As shown in Table 2, patients with HIV/AIDS had the highest levels of adherence (88%), whereas patients with hypertension reported the lowest level of adherence (64%). When asked to provide a reason for missing a dose, 26% of the patients reported that they simply forgot. Other reasons for missing a dose are reported in Figure 1.
Assessing Patients’ Adherence and Literacy Level.

Abbreviation: REALM, Rapid Estimate of Adult Literacy in Medicine.
aChi-square or Fisher exact if <5 in a cell.
bAs shown in Table 1, some patients reported multiple disease states. As such, there may be some overlap in the analysis of adherence versus nonadherence.
cSignificance determined at P < .05.
dHealth literacy level as determined by REALM scores.

Patients’ reported reasons for missing a dose.
We discovered that health literacy was not an indicator of a patient’s ability to comply with prescription therapy in treating chronic disease conditions. General trends for decreased adherence included lower dose frequency (ie, once-daily dosing) and lower daily pill burden. When patients are separated by disease state and evaluated for adherence, those patients who were HIV-positive showed the greatest trends toward adherence, followed closely by those with diabetes and then hyperlipidemia. Patients who have hypertension were found to be the least adherent. This is consistent with the most common reasons given for nonadherence, as the hypertensive population had the lowest daily pill burden and dose frequency.
Patients with high health literacy level were 21% more likely to be medication adherent (OR: 1.21, CI: 0.68-2.16); however, it is not statistically significant. We also adjusted this relationship by patients’ age, gender, education, and ethnicity, but the OR and significance level remained the same. Male patients were 2.87 times more likely than females to adhere to their medication regimen (Table 2). Moreover, ethnicity, age, and education level were not significantly associated with adherence in the multiple logistic regression model.
Discussion
This study examined the varying levels of health literacy and medication adherence in a group of patients with a broad range of disease states and medication regimens. Disease state and adherence were only significantly related in the HIV/AIDS and hypertension subsamples. Similar to our study, a recent trend report showed that diabetes and hypertension medication adherence was below the national average, particularly in the Midwest. 25 Notably, in this population, white patients displayed higher literacy level compared to black patients (Table 1: P = .002).
Additionally, patients with high health literacy levels were 21% more likely to be medication adherent (OR: 1.21, CI: 0.68-2.16); however, it is not statistically significant (P > 0.05). Therefore, the patients’ literacy levels according to REALM were not significantly associated with self-reported medication adherence in this small study sample. We relied only on self-reported medication adherence in this study, which could be imprecise. More accurate and automated medication adherence measures of tracking adherence, such as electronic drug monitoring (EDM) or partner/proxy reports could have provided more objective data. Moreover, medication self-management approach a new conceptual model including patient’s knowledge, skills, and behaviors necessary for patients to correctly take medications may be the accurate way to measure adherence. 34,39 However, the medication self-management approach does not take into consideration patient’s initial decision to acquire the medication as their primary treatment management option.
In this sample, 21% of patients read at a seventh- to eighth-grade level, which is the average reading level of American adults. 7,25 Therefore, in this underserved population, 64% of the patients read at above average reading level of American adults. Similar to general population, this underserved population reports “forgetfulness” as the most common reason for medication nonadherence. Interestingly, in this underserved population, 9% of the participants reported that they ran out of their medication. It is not clear whether this is happening because these patients did not have enough money to refill their medication or not. It is important to mention that many of these underserved patients are on free supply of medication provided by the free health clinic. Although from these study findings we cannot truly establish the actual reason for their running out of medication, this finding highlights an issue that warrants further investigation.
Limitations
Reliance on self-reported adherence is problematic and unreliable. It is possible that low-literacy patients did not fully understand their dosing regimen and thus could not accurately report their adherence to said regimen. If patients with low levels of health literacy were more likely to underestimate nonadherence, this could introduce systematic bias to our results. Other methods of tracking adherence, such as EDM or partner/proxy reports would provide more objective data. This may explain the discrepancy between our results and those of Murray et al, 34 which utilized EDM to measure adherence. However, it should be noted that the relationship between health literacy and self-reported adherence has been successfully demonstrated in other studies, such as the sample of HIV-positive patients using triple-drug antiretroviral therapy. 35
Our results suggest that adherence may vary by disease state. Indeed, HIV-positive patients may be more motivated to adhere to their drug regimen, given that nonadherence to antiretroviral therapy can have significant consequences, such as reduced viral suppression, poorer immunologic benefit, and overall treatment failure. 40 In comparison, a patient who is nonadherent to their hypertension medication is not susceptible to such risks and therefore may perceive fewer consequences of missing a dose. In light of this, an additional limitation of the current study is the relatively small sample size involving a variety of disease states, which prevented the analysis of the relationship between literacy levels and adherence within each disease category.
Conclusion
In this underserved population, 64% of the patients read at above average reading level of American adults. Overall MAR was 73%. Forgetting to take medication was the most popular reason provided for nonadherence. Interestingly, 9% of study population reported they ran out of their prescription medication. Disease state and adherence were significantly related in patients with HIV/AIDS and hypertension. Patient’s ethnicity was significantly associated with literacy levels (P < 0.05). Although patients’ literacy levels were not significantly associated with self-reported adherence in this population, availability of a patient’s baseline health literacy level as a part of the medical record may help clinicians to individualize their interaction in order to achieve better health outcomes, including improved medication adherence, especially for underserved populations.
Footnotes
Acknowledgments
The authors would like to thank the following: KCFHC, Obie Austin, RN, MSN, BC, ANP, Janna Haston RN, BSN, Tina Jones MA, Kristin Schwartz FNP-C, Carol Varland RN, BA, MHA. Patricia Marken, Pharm D, FCCP, BCPP Associate Dean for Student Affairs, Professor of Pharmacy Practice and Administration. University of Missouri – Kansas City.
Authors’ Note
This study was approved by the Institutional Review Board of the University of Missouri – Kansas City. This study was a public health resident’s research project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.