
Abstract
Objective:
To investigate the prevailing level of adherence to a dosing algorithm and a recall schedule and its relationship with the time in therapeutic range (TTR) among patients with atrial fibrillation.
Methods:
The study was carried out at a regional primary care clinic in Malaysia. Patients on anticoagulation therapy aged older than 18 years were included in the study. The participants have received continuation of their anticoagulation therapy at the primary care clinic for at least 6 months to 1 year after being discharged from a tertiary center. Correlation and multiple regression studies were performed to determine the significance of the predictors of TTR.
Results:
A majority (217) of patients with atrial fibrillation received anticoagulation therapy at the clinic followed by patients with mitral valve replacement and aortic valve replacement. The mean TTR for patients with atrial fibrillation was 57.6%. General practitioners (GPs) adhered to 75.5% of the dose protocol but fared poorly in adhering to the recall schedule (36.2%). The concordance to the dose algorithm and recall schedule were significantly related to TTR. Multiple regression analysis proved that the concordance to the dose algorithm and recall schedule were important predictors of the level of TTR in patients with atrial fibrillation.
Discussion:
The study provides preliminary evidence on the relationship between a validated dose algorithm that is integrated with a recall schedule in the control of TTR in patients with atrial fibrillation on anticoagulation treatment. A larger multicenter study is needed to confirm the results of this finding.
Introduction
Oral vitamin K antagonists (VKAs) are often used in various clinical settings and have a high level of efficacy in the prevention of thrombosis. 1 However, the optimal management of patients on long-term oral VKAs remains a complex task influenced by drug interactions, patient compliance, dietary habits, and inter-individual biological variations. 1 Also, patients have a greater tendency to either experience bleeding or a thromboembolic episode due to the narrow therapeutic range of VKAs. 2
The monitoring of anticoagulation therapy requires a strategy that minimizes the fluctuations yet maintains the required therapeutic levels that prevent thromboembolic episodes. One such monitoring method is the time in therapeutic range (TTR) index. The TTR is a reliable technique to assess the quality of anticoagulation therapy. 3 Furthermore, an increased TTR level is associated with antithrombotic efficacy, decreased mortality, and stroke rates. 3,4
The American College of Chest Physician (ACCP) guidelines recommend the use of a decision support tool to monitor patients on VKA therapy. 5 In a study involving the utilization of an inexpensive 2-step decision algorithm at a tertiary center, there was a significant improvement in mean TTR amongst patients treated at the anticoagulation clinic. 6 However, when a similar protocol was utilized at a primary care setting, the study produced poor results as the mean of the TTR group was proven to be not superior to usual care. 7
The primary aim of this prospective study is to examine the relationship of the prevailing practice of dose adjustments and patient recall period (without a decision support tool) on TTR among patients with atrial fibrillation (AF) at a primary care setting. The study will also help elucidate information on the prevalence and demographics of patients on anticoagulant treatment at a primary care setting.
The results of this study could help determine whether the quality of anticoagulation management in primary care could benefit from a standard dose nomogram that incorporates the element of a structured recall schedule.
Methods
Study Design
The study was conducted at the outpatient department of the Seremban Primary Health Clinic where most primary care patients in the district received anticoagulation treatment. A prospective descriptive study was conducted to determine the mean TTR in patients with the diagnosis of AF. All patients receiving at least 6 months of anticoagulation therapy at the primary care clinic were recruited into the study. Doctors adjust the warfarin dose based on previous clinical experience without the aid of a decision support tool. The proportion of concordance to a standard protocol was calculated in relation to a validated decision support tool to reflect adherence to the dosing and recall algorithms.
Study Patients
All patients receiving anticoagulation therapy at the primary care clinic were identified. Patients with AF (only patients with nonvalvular AF) receiving anticoagulation treatment at the outpatient department were recruited into the study. Patients were encouraged to refer to the warfarin booklet in their possession that provides information on dietary advice and possible drug interactions.
Patients were excluded if they were treated with a VKA other than warfarin, if they have been recently initiated on warfarin (less than 6 months), and if the therapeutic international normalized ratio (INR) range is not consistent with the recommendations stated in the 9th edition of the Antithrombotic Therapy and Prevention of Thrombosis guidelines of the ACCP. 5 Other exclusion criteria include patients who (1) had less than 6 months of anticoagulation management at the primary care clinic and (2) had incomplete data to aid statistical analysis.
Warfarin Dose Adjustment and Recall Period Scheduling
All decision making on dose adjustments and recall periods were based on clinical experience without the intervention of a decision support tool. The concordance to dose protocol was calculated based on an algorithm from a previous study. 6 Adherence to the dose protocol comprises (1) no dose changes if INR is within the therapeutic range, (2) 10% alteration in the weekly dose when 2 consecutive INR readings are out of range by no more than 0.5 units below or 1.0 unit above the therapeutic INR range, and (3) 10% to 20% dose adjustment in the weekly dose of warfarin when the deviation from the therapeutic INR range is greater. For very high INR derangements, warfarin would be withheld and/or given vitamin K when required.
The compliance to a recall period component was tested. The recall schedule was adapted from clinical literature. 8 Patients with 1 episode of high INR are recalled in 7 to 14 days after stopping treatment for 1 to 3 days. A low INR reading would necessitate a recall within 7 to 14 days. For a single therapeutic INR, patients will be scheduled to a 4-week appointment. Patients with consecutive 2, 3, 4, or 5 therapeutic INRs will be scheduled for an appointment at 6, 8, 10, and 12 weeks, respectively.
Data Analysis
The Rosendaal method serves as the basis of the calculation of TTR in this study. 9 In accordance to a previous study, 6 the following were excluded in the analysis: (1) the interval of more than 56 days between 2 consecutive INR readings and (2) the period 1 week before and 3 weeks after maintenance interruption.
The concordance with the dosing algorithm was determined by calculating proportions related to the adherence to the dose nomogram described subsequently (Table 1). Adherence was calculated by quantifying similarity between usual practice and the recommendations in the dose algorithm. The proportions of decision making in agreement with the recall schedule were calculated in a similar manner.
Demographic Data of Patients on Anticoagulation Treatment at the Clinic.
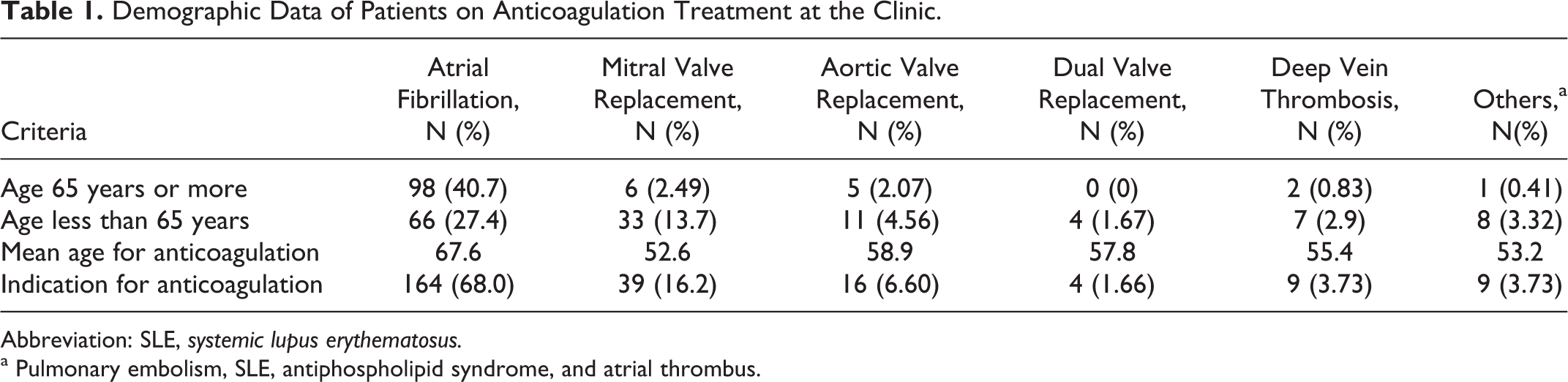
Abbreviation: SLE, systemic lupus erythematosus.
a Pulmonary embolism, SLE, antiphospholipid syndrome, and atrial thrombus.
Compatibility of the dose algorithm and recall schedule to the TTR in each patient was assumed by only including results that were in line with the exclusion criteria in the calculation of TTR using the Rosendaal method.
Statistical Analysis
Sample estimation and power analysis were determined through the G*Power software (version 3.1.9, University of Kiel, Germany). The sample size estimation of 74 patients was calculated using the effect size of 0.22, a confidence interval of 95%, and the margin of error of 5%. This gave a statistical power of 0.95.
The obtained descriptive data were reported as mean and percentages. Correlation and regression analyses were performed to determine the relationship between the mean TTR, the consistency of dosing using the algorithm, and the proportions of adherence to the recall schedule. The predictors that have significant influence over TTR were included into the regression analysis with TTR as the outcome variable. SPSS statistical software (version 20; IBM Corp., USA) was utilized to perform statistical analyses on data obtained from the study.
Results
The Prevalence of the Indications for Anticoagulation Therapy in the Primary Care Setting
A total of 294 patients received anticoagulation treatment at the primary care clinic. The majority of patients who received anticoagulation therapy had the diagnosis of AF (73.8%, 217 of 294) followed by mitral valve replacement (MVR) and aortic valve replacement (AVR). The least common indication for anticoagulation were patients with dual valve replacement (1.36%, 4 of 294).
Of 217 patients with AF, 164 were selected for the final statistical analysis; 53 patients with the diagnosis of AF were not included in the final analysis due to the rules set in the exclusion criteria described earlier.
Demographics of Patients on Anticoagulation Therapy
The demographics of patients on anticoagulation therapy is presented in Table 1. There was a greater number of patients above the age of 65 who received anticoagulation with the diagnosis of AF (40.7%). In comparison, there were higher rates of patients below the age of 65 receiving anticoagulation therapy who had MVR (13.7%), AVR (4.46%), dual valve replacement (1.67%), and deep vein thrombosis (2.9%).
The mean age was highest in patients diagnosed with AF (67.6 years), followed by dual valve replacement (57.8 years) and deep vein thrombosis (55.4 years). Majority of patients receiving anticoagulation treatment at the clinic were males (54.2%). A large proportion of patients receiving anticoagulation treatment at the clinic were of Malay descent (48.5%), followed by Chinese (39%) and Indians (11.6%). The main indication for anticoagulation treatment was AF (68%). The proportions of patients who had MVR or AVR were at 16.2% and 6.6%, respectively.
Mean TTR, Adherence to Dose Algorithm, and Adherence to Recall Schedule in Patients With AF
The descriptive statistics of both dependent and independent variables are presented in Table 2. The mean TTR for AF was 57.6%. The frequency of INR readings within range was at 50.7%. Doctors without any decision support tool adhered to at least 75.5% of the protocol stated in the dose algorithm. However, adherence to the recall schedule fared poorly at a rate of 36.2%.
Results of Regression Analysis of TTR, Dosing Algorithm, and Recall Schedule.

Abbreviations: TTR, time in therapeutic range; ANOVA, analysis of variance; VIF, variance inflation factor; Sig, significance.
Correlation and Regression Analyses Between TTR, Dose Algorithm, and Recall Schedule in Patients With AF
The results of the regression model are presented in Table 3. Time in the therapeutic range was significantly correlated with the dose algorithm and the recall schedule (r = 0.367, P < .01; r = −0.212, P < .01). Multiple regression analysis was used to test whether the dose algorithm and recall schedule significantly predict changes in the TTR.
Results of Descriptive Statistics for TTR, Dosing Algorithm, and Recall Schedule.
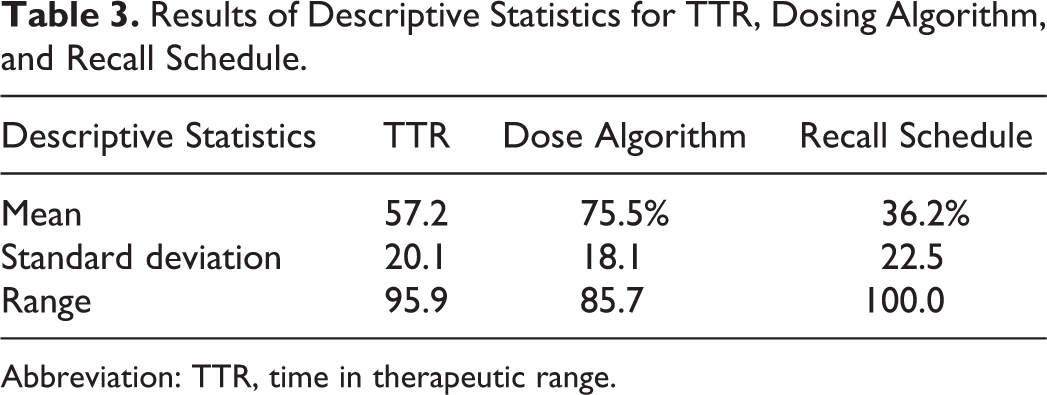
Abbreviation: TTR, time in therapeutic range.
The results of the regression show that the 2 predictors explained 15.6% of the variance (R 2 =.17, F 2,16 = P < .01). The dosing protocol significantly influenced the TTR (β = .41, P < .01) as did the recall schedule (β = −.17, P < .01). Hence, the regression equation derived from the following analysis: [TTR] = 0.406[dose algorithm adherence] − 0.167[recall schedule adherence] + 33.0.
Discussion
Main Findings
This analysis would be the first in Malaysia documenting the prevalence, the current level of adherence to protocol, and the monitoring of TTR in a primary care setting among patients with AF. A similar study was conducted at a tertiary care center in Malaysia but excluded observations on TTR and adherence to a dose protocol or recall schedule. 10
The mean TTR in this study is lower than the recommended range of TTR at 58% to 65% for antithrombotic effect. 1 The data from this study show that the low levels of TTR could be explained by the lack of adherence to a dosing algorithm. The regression model also indicates that improvements in TTR could be achieved by increasing adherence to a dosing protocol. A substantial shift in favor of the positive predictor (adherence to a dosing protocol) could override the negative predictor (adherence to a recall schedule). This translates to the flexibility in the maintenance of an optimal TTR, despite an increase in the duration of between 2 INR readings or an increase in the frequency of recall due to a deranged value.
The regression model seems to explain that a validated nomogram has the potential to reduce the variability in INR readings among patients with AF on VKAs. Increased variability between readings caused by a phenomenon called the “ping pong effect” 11 could be palliated by the implementation of an effective dose algorithm with an integrated recall schedule.
Secondary Outcomes
In an earlier study, the prevalence of patients with MVR on anticoagulation therapy supersedes that of patients with AF. 12 In this study, the prevalence of patients with AF on anticoagulation therapy is more than patients with MVR. These findings seem to confirm the results from a study conducted at a primary care setting 12 and tertiary care. 13 The mean age of patients with AF on treatment was much lower than the mean age of similar studies at a primary care setting. 7,14 The proportion of the male population on anticoagulation treatment was greater than females, similar to other studies done at tertiary care centers, 6,13 but there was a slight female preponderance at primary care centers. 7
Study Limitations
There are few limitations of this study. The study recruited patients with AF from a single regional primary care clinic. Although most patients were from other primary care clinics who did not have access to INR investigations, these results might not be representative of all primary care clinics in Malaysia.
Secondly, this study did not focus on the correlation and regression analyses of other groups (MVR, AVR, dual valve replacement, and deep vein thrombosis) who received anticoagulation treatment at the primary care clinic. The sample size was insufficient to provide enough statistical power for a significant finding. A multicentered study with a larger population size would be required to achieve this objective. In classifying patients with AF, no differentiation was done to distinguish patients with paroxysmal and chronic AF. All patients were categorized under the broad term of AF.
Conclusion
There is a relationship between TTR and the predictors of a dose nomogram which incorporates the elements of a recall schedule. The preliminary results from this study indicate that poor adherence to a dose algorithm that is coupled with a recall schedule could lead to a decline in TTR. However, the 2 predictors examined in this study only explained less than half of the effects on TTR.
Larger studies should be conducted to verify the model described earlier as a method to improve the TTR among patients on anticoagulation therapy at a primary care level, especially patients diagnosed with AF through case–control studies.
Footnotes
Authors’ Note
The study protocol received approval from the Malaysian Medical Research Ethic Committee.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.