
Abstract
Aim:
Primary care practitioners should screen young adolescent patients for idiopathic scoliosis and refer those who could benefit from bracing to prevent curve progression and the need for surgery. Adolescents without a regular source of primary care may be at higher risk for not having their scoliosis diagnosed in time to benefit from bracing. We sought to determine whether adolescents with idiopathic scoliosis and a regular source of primary care are at lower risk of scoliosis surgery.
Methods:
We followed a cohort of 3722 adolescents (10-18 years) whose diagnosis of adolescent idiopathic scoliosis was confirmed by an orthopedist or physiatrist, using linked administrative data of physician visits and hospital admissions, from 2001 to 2010. We used survival analysis to compare those with and without a regular source of primary care with regard to having scoliosis surgery, adjusting for covariates.
Results:
Among the 3722 adolescents with scoliosis, 12% did not have a regular source of primary care and 158 had scoliosis surgery. Adolescents with a regular source of primary care had a lower risk of scoliosis surgery (hazard ratio 0.60, 95% confidence interval 0.40-0.89), especially those whose regular source of primary care was a pediatrician (hazard ratio 0.48, 95% confidence interval 0.30-0.76).
Conclusion:
Adolescents with scoliosis and a regular source of primary care were less likely to undergo scoliosis surgery. Policy makers need to be aware of the importance of primary health care for children and adolescents and ensure that they are not forgotten in their campaign for primary care improvement.
Adolescent idiopathic scoliosis (AIS) is a complex 3-dimensional deformity in adolescents, and AIS surgery is the most common procedure in pediatric orthopedics. 1 Surgery is effective in correcting the deformity but has costs and potential risks or side effects. 2 –4 Bracing can prevent the need for surgery, if persons are diagnosed early enough. 5,6 Primary care practitioners should screen young adolescents during office visits 7,8 and refer appropriate cases to orthopedic specialists.
Key concepts on how family physicians can detect, refer, and manage AIS have been reviewed by Reamy and Slakey. 7 They suggest the use of the Adams Forward Bending Test along with a scoliometer to measure the rib hump and the referral of patients with curves above 20° irrespective of Risser grade (growth potential). Others feel that those who have finished their growth and have curves <40° need not be referred. 9 Those with curves under 20° should be observed by the primary care physician at a frequency of every 6 months. Referrals may be inappropriate or too late to benefit from bracing, 10,11 and there may be an increased rate of surgery when compared with populations that have school screening programs in place. 11 Although there are gaps in knowledge among primary care practitioners when it comes to scoliosis, most primary care practitioners know enough to refer urgent cases that have a high risk of progression. 12
Persons who do not have a regular source of primary care may be at higher risk for not having their scoliosis diagnosed in time to benefit from conservative treatment and will require surgery. Our aim was to determine whether adolescents with idiopathic scoliosis and a regular source of primary care (family doctor or pediatrician) are at lower risk of scoliosis surgery.
Methods
The research design is an administrative data-based cohort study, in a context where all residents are covered by universal health insurance for doctor visits and hospitalizations. Data were denominalized, and we received ethical authorization from the Access to Information Commission of the province of Quebec.
The population consists of persons who live in the city of Montreal (aged 10-18 years) diagnosed with AIS 13 identified from the linked Quebec provincial physician claims database and Quebec provincial hospital services database. All persons diagnosed with AIS between 2001 and 2010, whose diagnosis was confirmed by an orthopedic surgeon, are included in the cohort.
The outcome of interest in the study is surgical treatment of AIS. The independent variable is having a regular source of primary care. We adapted the algorithm described by Shah et al 14 to our physician claims database, whereby the primary care doctor who was seen the most in the 2 years prior to diagnosis was deemed the regular source of care. We identified whether this doctor was a family physician or a pediatrician. Persons who did not see a primary care physician were classified as not having a regular source of primary care.
Certain other factors may be associated with having surgery and also having a regular source of primary care. Children who are diagnosed at a younger age have the potential for more growth, increase in the scoliosis, and possible need for surgery. 15 –17 Also younger children may be more likely to have a source of regular primary care. 18 Scoliosis is more prevalent in girls, and curve progression is higher among girls. 15,16,19 Female gender may be a factor in accessing primary care. 20 Socioeconomic status, even in a context of universal health care, is associated with having a regular source of primary care, 21 although it is unclear whether it is associated with having scoliosis surgery. In our administrative cohort study, socioeconomic status is based on a validated index of material deprivation that uses census tract data. 22 Pattern of health care use may be associated with recognition of the scoliosis sooner (ie, those who visit the doctor more frequently would be more likely to have their scoliosis detected). 11,15 We defined pattern of previous health care use as number of physician visits (to any doctor) in the year prior to diagnosis of AIS. Severity of the scoliosis curve is a strong predictor of the need for surgery. 16,19,23 Although we do not have this indicator for curve severity in the administrative database, younger age at diagnosis can serve as a proxy for severity and those diagnosed younger are at higher risk for curve progression. 24 Further, it is possible that if a primary care physician first diagnoses the patient and enters that diagnostic code for the visit (ie, confident in the diagnosis without need for confirmation by a specialist), this may denote a more serious curve. Thus, adjusting for who made the first diagnosis may also be a marker for severity.
Analysis
We used the model inspired by Penchansky and Thomas 25 and Andersen, 26 focusing on predisposing factors (having a regular source of primary care and socioeconomic status) and perception of need (age, gender, severity, and history of health care use) to determine their influences on outcome (having surgery for AIS). We first used descriptive statistics to characterize our population, followed by bivariate associations between the explanatory variables and the outcome. Next, we used Kaplan-Meier analysis and the log rank test to assess whether time until surgery for scoliosis is associated with having a regular doctor (family doctor or pediatrician) versus not having a regular source of primary care. In the multivariable time-to-event analyses, we used Cox proportional hazards regression to determine whether scoliosis surgery (and time to surgery) is associated with having a regular source of primary care, adjusting for sex, age (at diagnosis), prior health care use, whether the first scoliosis diagnosis was made by a primary care physician, and socioeconomic status. We also adjusted for the interaction of age and sex; younger girls with scoliosis may be considered at higher risk of curve progression (and surgery) than younger boys. 19 Time zero was set as the date of first diagnosis of AIS. We also calculated another Cox model, separating the main independent variable into having a regular family physician, a regular pediatrician, or having no regular source of primary care (reference category) adjusted for the same covariates as in the previous model. Analyses were done using SAS version 9.1.3.
Results
Between April 1, 2001, and March 31, 2010, a total of 3722 persons (aged 10-18 years) living in Montreal were diagnosed with AIS by an orthopedist. The average age at first diagnosis of AIS was 13.8 years (standard deviation 2.13), and 65.2% were female. Among all 3722 persons in our cohort, 12.3% did not have a regular source of primary care, whereas 44.4% had a regular family physician and 43.3% had a regular pediatrician. In the year prior to AIS diagnosis, 10.67% had not seen a doctor. There were 158 (4.25%) persons who underwent surgery for AIS. A description of our cohort can be found in Table 1.
Description of Cohort.a

Abbreviation: AIS, adolescent idiopathic scoliosis.
aN = 3722.
Bivariate analysis indicated that 3.8% of those with a regular source of primary care had surgery for AIS compared with 7.4% of those with no regular source of primary care (P = .0003). Mean age at diagnosis was higher among those with no regular source of primary care (14.4 vs 13.7, P < .0001).
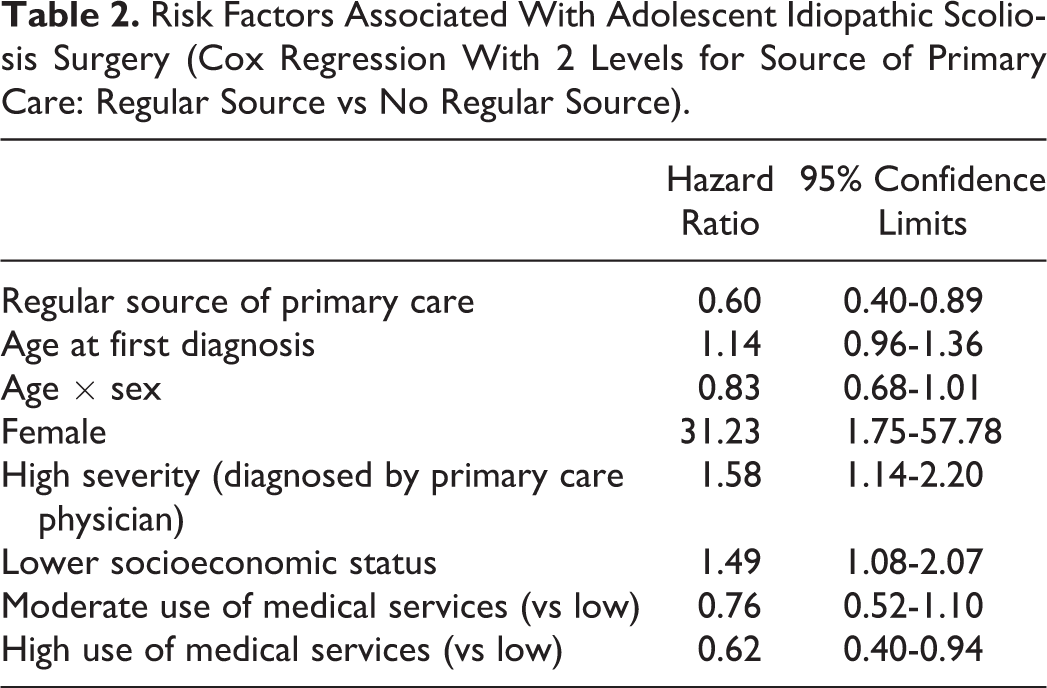
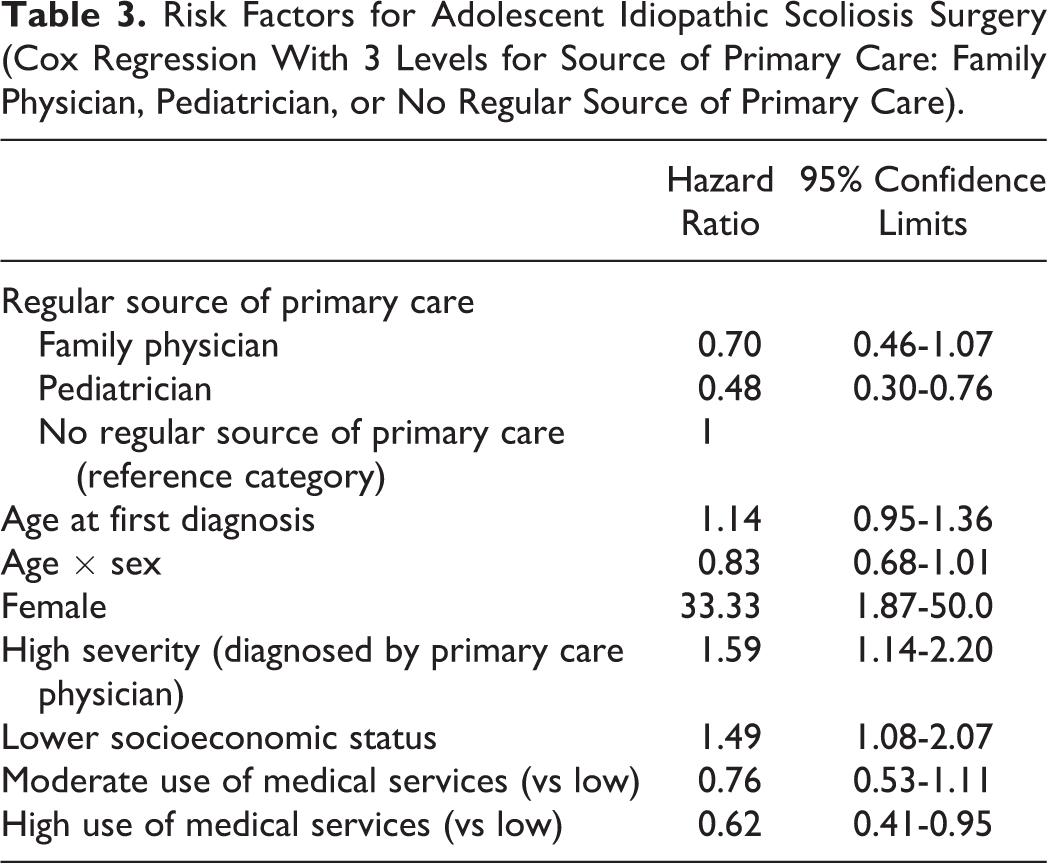
Kaplan-Meier analysis (Figure 1) showed that having a regular source of primary care was associated with decreased risk of surgery (log rank test P = .0001). The results of the Cox regression analysis are reported in Table 2. Persons with a regular source of primary care (family physician or pediatrician) were at lower risk for having surgery for AIS (hazard ratio 0.60, 95% confidence interval 0.40-0.89). Being female, having a higher severity (first scoliosis diagnosis by primary care physician), being a higher user of medical services and having a lower socioeconomic status were associated with higher risk of AIS surgery. We repeated the Cox regression, separating the main independent variable into 3 categories: regular family physician, regular pediatrician, and having no regular source of care (Table 3). Although for both types of regular source of primary care, there was a lower risk of undergoing AIS surgery, the estimate was statistically significant only for the pediatrician.

Kaplan-Meier curves for adolescent idiopathic scoliosis (AIS) surgery and having a regular source of care (pediatrician, family physician, and no regular source of primary care). Log rank test: P = .0001. The figure depicts the survival function (percentage with no scoliosis surgery) over time from first diagnosis for those who had no regular source of primary care versus those who had a regular source of primary care: family physician or pediatrician. The solid curve depicts those with a pediatrician, the curve with the smaller dashes depicts those with a family physician, and the larger dashed line those with no regular source of primary care. The y-axis indicates the percentage of patients who did not have scoliosis surgery, and the x-axis indicates time (in days). The figure shows that those who did not have a regular source of primary care had an increased risk of surgery.
Risk Factors Associated With Adolescent Idiopathic Scoliosis Surgery (Cox Regression With 2 Levels for Source of Primary Care: Regular Source vs No Regular Source).
Risk Factors for Adolescent Idiopathic Scoliosis Surgery (Cox Regression With 3 Levels for Source of Primary Care: Family Physician, Pediatrician, or No Regular Source of Primary Care).
Discussion
In our cohort of urban adolescents, we found that adolescents with AIS who had a regular source of primary care were less likely to undergo surgery for AIS, especially for those who had a pediatrician as their regular source of care. Having a regular source of primary care may favor early diagnosis and appropriate management, reducing the risk for AIS surgery.
In order to access specialized scoliosis clinics in Canada, patients require a referral from another physician. In general, being without a regular source of primary care is associated with a lower chance of being referred to a specialist. 27
Delays in seeing an orthopedic specialist for AIS may occur as a result of delay in referral by the primary care practitioner or delay in getting an appointment once referred to the orthopedic specialist. In Canada in 2012, approximately 15% of adolescents (12-19 years of age) did not have a regular medical doctor. 28 In our urban cohort, we found that just over 12% did not have a regular doctor. Delays in getting an appointment to an orthopedist may also be problematic. 11,12 Irrespective of the reasons, many AIS cases appear to be detected and referred too late to benefit from conservative treatment. 10,11 Our results imply that having a regular source of primary care may help improve the situation. The importance of primary care for adolescents has been highlighted for sexual health, mental health, asthma, and musculoskeletal health associated with sport injuries 29 –33 ; however, very little attention has been paid to scoliosis. Furthermore, primary care reform has concentrated for the most part on adults (especially the elderly patients or those with chronic disease) and very little on children and adolescents. 34
Our study emphasizes the importance of primary care for adolescents with AIS, to potentially prevent the need for surgery, which is costly and has a risk of complications. 2,3 Study strengths include the use of population-based data and the fact that all patients were diagnosed with AIS by an orthopedist. Although we do not know who were prescribed a brace, appropriately referred and who were not, this is part of the question we wish to answer (ie, it is in the “causal pathway” of the association between having and not having a regular primary care source) similar to studies that assess screening effectiveness. 35,36
There is no measure of severity in these databases, and delays for consultation may be affected by severity. We used age at diagnosis as a proxy for severity, which can be an indicator of severity. 24 We denoted those that were first diagnosed with AIS by the primary care physician as likely being more severe. Although severe cases are likely to be identified by the family, 11 they would require assessment by a primary care physician before referral to the specialist. There may be other potential confounders that cannot be assessed from the database, such as patient’s psychological status, attitudes, beliefs, preferences, and expectations toward medical care. Finally, there may have been patients who were appropriately referred and prescribed braces but who did not adhere to wearing the brace leading to progression of their scoliosis and the requirement for surgery; however, recent research indicates good compliance in wearing the brace. 37
The conclusion is that having a regular source of primary care for children and adolescents is associated with a lower frequency of AIS surgery than among those without a regular source of primary care. Those who were under the care of a pediatrician were more likely to benefit. Policy makers need to be made aware of the importance of primary health care for children and adolescents and ensure that this segment of the population is not forgotten in their campaign to ensure access and high-quality primary care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Ehrmann Feldman was supported by a senior salary award from the Fonds de recherche santé - Québec.