
Abstract
It is known that Florida school employees known as Migrant Advocates facilitate or broker MSF health care access for migrant and seasonal farmworker (MSF) families, but it is not known how states without a Migrant Education Program might also broker MSF health care access. To address this, present study examines the role of school employees in brokering health care access to immigrant Mexican and Indigenous Guatemalan MSF families in Connecticut. Informed by prior work, interviews (n = 12) with parents and elementary school employees showed that (1) a vast array of non-Migrant Advocate school employees, mostly Latinx women, directly brokered physical and psychosocial MSF health care access, often through developing deep social relationships and (2) barriers to brokerage included language inaccessibility, school employee gaps in knowledge of MSF health care needs, and transportation and related structural issues. Importantly, the school’s location near MSF homes is an important contributor to the success of the school’s brokerage efforts. Findings offer insight into how a school health broker model might be implemented, and advance understandings of MSF health and health care access.
Keywords
Introduction
Migrant and seasonal farmworkers (MSFs) are people who work on farms or in agriculture, typically planting and harvesting crops—they may move for work with the crop cycle (migrant) or remain stationery and work on the farm during the crop season (seasonal). As understood by the concept of structural vulnerability (Hernández-Rosete Martínez et al., 2005), MSFs are vulnerable to oppression due to their multiple minoritized social positions within the United States and global structures, which often result in poor health outcomes (Arnold et al., 2021; Bade, 2004; Campbell-Montalvo & Castañeda, 2019; Holmes, 2013; Quandt & Arnold, 2020).
However, researchers have identified one way that such minoritized peoples are supported in their access to resources: facilitation or “brokerage” by a third party (Burt, 2005; López-Sanders, 2017). A recent study in Florida K–12 schools found that a group of predominantly Mexican women school employees known as Migrant Advocates brokered access to health care for Indigenous and non-Indigenous Mexican MSFs (Campbell-Montalvo & Castañeda, 2019). Migrant Advocates were trusted, easily accessible, and seen frequently by families, often going above and beyond their official duties to facilitate MSF families’ access to health care by providing interpretation, translation, and transportation. This brokerage was made possible by the state’s federally supported Migrant Education Program (MEP), which provided financial and other assistance to specifically aid these students through Title I Part C of the Every Student Succeeds Act. These findings introduce the possibility of a novel mechanism to address MSF health in the form of a school health broker model. Yet, across the United States, public K–12 schools vary in their systems of key personnel (e.g., nurses, Migrant Advocates, social workers, paraprofessionals) available to support MSF families.
In the conversation about the role of schools in MSF health care brokerage, it is not clear how schools without an MEP, such as those in Connecticut, meet MSF children’s health needs (i.e., reported physical and psychosocial ailments or health conditions) and health care access (i.e., ability to use “personal health services to achieve the best health outcomes”; Millman, 1993, p. 4). To address this, the present study centers on how key personnel in a Connecticut school understand the health needs and broker health care access of MSF families and their children. The current investigation, including the recruitment of school employees providing resources akin to health care access brokerage, is informed by Campbell-Montalvo and Castañeda (2019). The present inquiry also highlights the experiences of Indigenous Guatemalan families, adding to previous research.
Structural Vulnerability and Brokerage: Migration Health Risks and Access to Health Care
Marginalized social positionings and structural vulnerability of MSF children and families affect their health outcomes and hinder their access to health care (Hernández-Rosete Martínez et al., 2005). Researchers have shown that unequal social and economic policies, poor working conditions, and low wages increase MSF families’ physical and psychosocial health risks. Specifically, farmwork-related structural factors lead to exposure to environmental hazards affecting physical health, including pesticides and heat, and an increased risk of being overweight and obese (Quandt & Arnold, 2020). Moreover, MSFs in the United States are at higher risk of diabetes due to higher health markers in weight, blood pressure, dental health, and cholesterol, as compared with non-MSFs (Bade, 2004; National Center for Farmworker Health, 2017). MSFs also report increased levels of chronic pain (Holmes, 2013) and hearing loss (Masterson et al., 2017).
Farmwork-related structural factors also spur psychosocial hazards such as discrimination, financial impoverishment, food insecurity, and interpersonal violence (Quandt & Arnold, 2020), and children engaging in farmwork are not excluded from experiencing hazards (Arnold et al., 2021). Additional vulnerabilities for MSFs include a lack of transportation, linguistic barriers, immigration status, lack of insurance, as well as lack of familiarity with the U.S. health system (Campbell, 2016; Campbell-Montalvo & Castañeda, 2019; Castañeda, 2010). These intersect to affect psychosocial health wherein farmworkers report higher rates of ailments such as depression (Limon et al., 2018). Additionally, at school, MSF students often encounter negative reactions of others to their identity and community memberships (i.e., xenophobia), which affects their development and can lead to psychological trauma (Saldaña et al., 2021; Villarreal Sosa, 2019).
Many of the same structural influences putting farmworkers at increased physical and psychosocial health risk also present barriers to their access of services that could improve these conditions. MSFs’ access to public assistance for food, shelter, and medical health resources is affected by citizenship and other policies (i.e., U.S. Department of Homeland Security, 2018). In comparison with non-MSFs, MSF families, including those in Connecticut, access Medicaid and Children’s Health Insurance Program services at a lower rate (Oropesa et al., 2015; Vargas & Ybarra, 2016; Yun et al., 2013). National ideologies discount these structural risks as well as the structural obstacles to accessing supports that protect health, instead attributing health and health outcomes to individual responsibility, and family health to the responsibility of mothers (Gálvez, 2019).
The ethnic, migratory, and racial characteristics of farmworkers are relevant to understanding their structural vulnerability. Eighty-three percent of MSFs are of Latinx origin, and 75% are immigrants (Hernandez & Gabbard, 2018). Latinx children display emotional changes following the passage of anti-immigrant policies, including fear and depression (Rubio-Hernandez & Ayón, 2016). According to the U.S. Department of Agriculture (2016), about half of farmworkers are unauthorized, which brings health risks. There are also barriers to health care service provision for immigrants (Viladrich, 2021), especially those who are undocumented, including not knowing the rights that individuals have when accessing care, privacy concerns, and not trusting that systems will be responsive to their needs (Valdovinos et al., 2021). Though it is not known how many Indigenous Latinx MSF people live in Connecticut, one million Indigenous Latinx people reside in the United States (McGuire & Georges, 2003). Indigenous MSFs are marginalized on multiple ethnic, racial, and national axes (Casanova, 2012; Casanova et al., 2016; Zúñiga et al., 2014), with worse markers of health than those who are not Indigenous (Bade, 2004; Holmes, 2013; National Center for Farmworker Health, 2017). Movement of Indigenous Central Americans into the United States has been thrust into the spotlight in the recent years as parents sought reunification with their children as they were separated at the U.S.–Mexico border (i.e., Schmidt, 2018). These movements have been spurred by multiple push and pull factors, including the 1960 to 1996 Guatemalan civil war, during which the wounds of 500 years of violence against Indigenous people were reopened, resulting in immense individual and group trauma; afterward political corruption, organized crime–related homicides, and threats to environmental sovereignty in Indigenous areas were rampant (Villarreal Sosa & Lesniewski, 2020). Historically, Mexicans have come to the United States to try to escape inequality and secure better economic opportunities (Campbell, 2016). At the same time as these pressures encourage movement into the United States, anti-immigrant discourses, as well as those regarding the fertility of Mexican women, shape interactions between MSF families and educators, medical personnel, and others who affect their access to resources (Gálvez, 2011).
Within this context, key school personnel may bridge or “broker” gaps in access to health care services (Burt, 2005; Campbell-Montalvo & Castañeda, 2019; López-Sanders, 2017). Previous research has examined brokering in educational contexts, focusing on “child language brokering,” wherein children facilitate communication between parents and teachers (García-Sánchez et al., 2011; García-Sánchez & Orellana, 2006). Scholarship has also examined child language brokering in health care settings when it comes to conflict resolution and children protecting their families from misperceptions of health care providers (García-Sánchez, 2014). Yet, prior work has also shown that school employees often Latinize students as only Latinx and not Indigenous, resulting in an under counting of Indigenous Latinx people and the languages they speak, contributing to brokerage activities not being available in Indigenous languages (Almasalkhi, 2021; Baquedano-López, 2019; Baquedano-López & Borge Janetti, 2017; Campbell-Montalvo, 2020a, 2020b, 2021; Campbell-Montalvo & Castañeda, 2019; Campbell-Montalvo & Pfister, 2021; Chón et al., 2021; Saldaña et al., 2021).
In the intersecting body of research on health care, brokerage, and education, actors such as school social workers often challenge power structures and become social change agents in the process of mediating MSF students’ physical, cultural, and psychological transformations (Villarreal Sosa, 2019; Villarreal Sosa et al., 2021). They often provide mental health services when students are dealing with trauma (Villarreal Sosa, 2019). Other actors, such as health advisors, also provide crucial services, such as the home-delivery of knowledge of pesticide dangers for children whose families engage in farmwork (Quandt & Arnold, 2020). The aforementioned Migrant Advocates take students to eye appointments, provide transportation for specialist visits, perform translation at doctor’s appointments, and discuss reputable clinics with families (Campbell-Montalvo & Castañeda, 2019). Indeed, a range of community resource persons provide parenting support to families with a migration background (Vindevogel & Van Wolvelaer, 2021).
Our present study builds on this corpus of scholarship, particularly Campbell-Montalvo and Castañeda (2019), by locating schools as a site at which powerful nodes, or linkages of social connections between people, affecting the health of MSF families operate. Specifically, our inquiry is driven by the research question:
In alignment with our focus on structural vulnerability, we frame our work within the Whole School, Whole Community, Whole Child Model. The Whole Child Model conceptualizes schools as intersections of individuals, families, educators, and the local community important to a child’s overall well-being (Centers for Disease Control and Prevention, 2015). It has 10 components focusing on access to food, health education, social and emotional climate, health services, psychological services, employee wellness, family engagement, and more (Centers for Disease Control and Prevention, 2015). This model offers a site of analysis at the nexus of these structures enabling a focus that can inform policy change affecting health care access.
Method
Research Site
Nearly 20,000 MSF adults live in the Connecticut River Valley region (State of Connecticut, n.d.), yet there is no verifiable data on how they and their children are served by local schools. In Connecticut, unlike as required by mandates in states with MEPs, students’ migrant status is not identified during school registration (Connecticut State Department of Education, personal communication, October 2, 2017). Duke (2011) suggests that most Connecticut MSFs are from Latin America or the West Indies, though changing migration routes and economic shifts have influenced the current demographic compositions of migrants as well as the types of crops in which they work. MSFs in Connecticut have commonly worked in shade and broadleaf tobacco, fruit trees, or in nurseries throughout the state (State of Connecticut, n.d.).
To inform on the applicability of previous research and understand how health care access brokerage might be occurring in a state without a MEP, data for this study were collected from one elementary school in Eastern Connecticut that we refer to using the anonym “Nippawus.” Nippawus is located near farms known to employ MSFs. Table 1 summarizes school, district, and state students’ characteristics with respect to percentages of selected racial and ethnic groups and students classified as “English Language Learners” (Connecticut State Department of Education, 2020). Nippawus is demographically similar to its district but serves a larger percentage of “English Language Learners.” Many children from migrant families attending Nippawus are from Guatemala and speak K’iche’, not English, and often not Spanish.
Student Characteristics at School, District, and State Levels, 2017–2018 (Connecticut State Department of Education, 2020)

Rounded to nearest hundred. bData have been suppressed to ensure student confidentiality.
Outside of the predominantly monolingual English-speaking teacher workforce, most staff (i.e., the principal, administrative assistants, the nurse, social workers) at Nippawus speak both English and Spanish. Written communication to families is sent home from the school in English and Spanish. Some classrooms use bilingual programming. Additional Spanish–English bilingual employees provide services uncommonly offered in other schools, such as through the school’s state and federally grant-funded Family Resource Center (FRC) or in the capacity of a Family Liaison. There is no known Indigenous language-speaking employee at Nippawus.
Participants and Recruitment
This study is scaffolded on first author Campbell-Montalvo’s previous multisited and multimethod elementary school ethnography (Campbell, 2016; Campbell-Montalvo, 2020a, 2020b, 2021; Campbell-Montalvo & Castañeda, 2019; Campbell-Montalvo & Pfister, 2021; Saldaña et al., 2021). The previous study included a total of 46 interviews (17 with school employees such as Migrant Advocates and 23 with parents, including MSF parents), a focus group with Migrant Advocates (n = 7), ~150 home visits with MSF families, and additional classroom and school observations including at events serving MSF families specifically and generally (~100). Though more Guatemalan MSFs are now being served in the area, at the time of the earlier study, most MSF students served in Florida were Indigenous and non-Indigenous Mexicans.
Given that Connecticut has no Migrant Advocates, in the current study we sought to identify school personnel (e.g., the social worker, the school nurse, FRC staff members, etc.) who might perform similar roles as Migrant Advocates. To understand the parental perspective of this inquiry, we recruited MSF parents who accessed resources provided by the school from these school employees. A total of 12 interviewees were recruited: six were MSF parents and six were key school personnel. Given that the study mobilized preexisting theory and sought to determine applicability of findings from previous research in a new context, six parent and six personnel interviews had the information power needed (Malterud et al., 2016). In addition, this sample size is able inform on some of the health needs experienced by the population of interest as part of the more exploratory part of the study, given that a complete description of all aspects of health needs was not the goal (Malterud et al., 2016). Participants and their selected characteristics are listed in Table 2. Notably, all but one of the participants—the people existing in the care roles sampled—are Latinx women, coinciding with Campbell-Montalvo and Castañeda (2019), which found that Latinx women school employees members and Latinx mothers frequently took on the provision of care discussed here. In both the Florida and Connecticut research, while relevant school employees were Latinx, their race and nationality were somewhat dissimilar to those of the students they served.
Selected Participant Characteristics
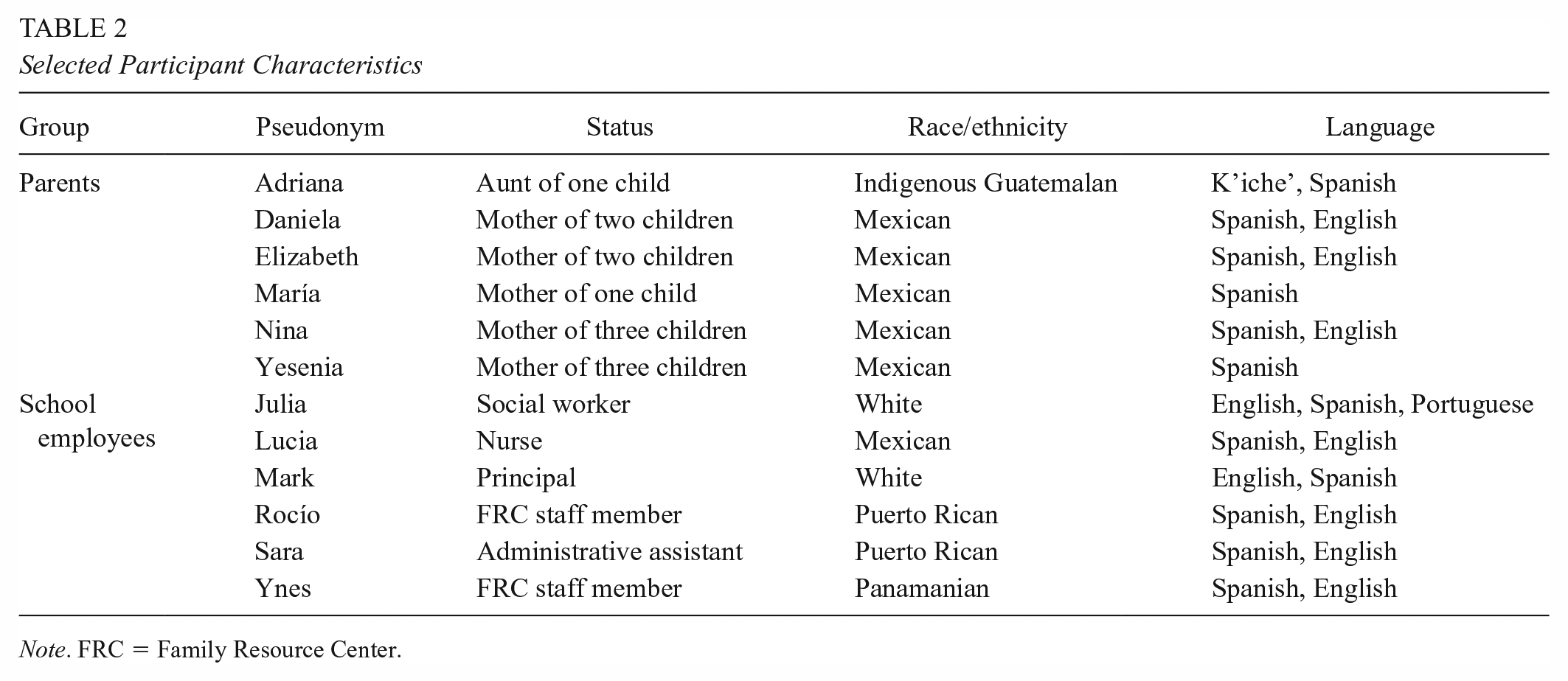
Note. FRC = Family Resource Center.
To facilitate recruitment and provide background information for interviews, over the course of 2 days per week for 2 months during the 2018–2019 school year, members of the research team spent time at the research site (i.e., spending time in school office, attending parent classes and events such as a Mother’s Day Breakfast with MSF participants at the FRC). Participants were selected based on how they matched the inclusion and exclusion criteria in the study. Inclusion criteria included the following: (1) MSF parents speaking English and/or Spanish with at least one child enrolled at the school and (2) school personnel speaking English and/or Spanish who work directly with MSF students. Exclusion criteria included participants younger than 18 years old. The study protocol was approved by the University of Connecticut Institutional Review Board.
Data Collection and Analysis
Themes from previous research informed the data collection and analytical methods employed in the present study. For example, Campbell-Montalvo and Castañeda (2019) found that MSF families encountered barriers to health care access, but key school personnel (Migrant Advocates) interacted with families consistently, providing important, culturally relevant knowledge about how to access health care (though Advocates faced their own barriers in health care brokerage). For the present study, data were gathered using semistructured interview protocols adapted from Campbell-Montalvo and Castañeda (2019) that focused on MSF health needs, MSF health care access, school employee health care brokerage, and obstacles to brokerage. Parent interview guides were created in Spanish and English, and school personnel guides were created in English. The complete guides are provided in Appendices A to C.
Interviews were conducted during the 2018–2019 school year, and each participant was interviewed one time. Interviews with parents were conducted by a member of the research team who identifies as Chicana and is fluent in Spanish and English. The interview often comprised parents’ sole in-depth interaction with the research team. Interviews with school employees were conducted by a White woman member of the research team. Most school employees had had more in-depth interactions with research team members prior to the interview, particularly given that the interactions were a necessary starting point to understand the site and locate participants.
The interviews lasted 45 to 60 minutes and were conducted in English or Spanish in the school conference room or privately in employee offices. The interviews were robust dialogues in which probing questions were used to prompt thick descriptions as needed—enabling the elicitation of more information out of a smaller sample (Malterud et al., 2016). Informed consent from participants was documented and all interviews were audio-recorded and transcribed verbatim.
Data were analyzed in their original language, with translations provided by the authors in the footnotes. Based on the study’s research question, previous scholarship, and after the researchers reviewed the transcripts, a codebook was developed to code the interviews with subthemes relating to specific health care needs, methods of brokerage, and barriers to brokerage. Thematic analysis (Braun & Clarke, 2006) was then used to identify subthemes and to compare school personnel and parent views on how employees brokered MSF students’ health needs and health care access.
Findings
Interview data showed that MSF students attend Nippawus, but employees offered varying estimates regarding how many MSF students attend the school. Mark 1 (a White principal) estimated that 10% to 15% of students’ families were MSF, while Lucia (a Mexican nurse) estimated 25%, and Sara (a Puerto Rican administrative assistant) 30%. Mark noted that 10% to 15% of students from the current school year were newly arriving immigrants, with most coming from Guatemala, and many were Indigenous K’iche’ speakers. Interviewees explained that chain migration and church connections facilitated job searches for incoming migrant families and encouraged a continued movement of people to the area.
Three major themes emerged from participant interviews regarding health needs and health care access brokerage. These were structurally influenced and included (1) physical health needs and their brokerage, (2) psychosocial health needs and their brokerage, and (3) barriers to brokerage.
Physical Health Needs: Immunization, Vision, and Dental
The first group of health needs relates to MSF families’ physical health needs, with these needs and access to services to treat them being affected by structural vulnerability. These needs include the necessity to meet school requirements associated with immunizations as well as general physical health needs, including those such as dental and vision care.
Like students across the United States, students at Nippawus must meet immunization requirements to enroll in school—a need embedded in a more general necessity of health care access. Federal, district, and school policies state that children without immunizations are not permitted to attend school. Schools are required to keep track of whether students have fulfilled these requirements, and Nippawus must annually report the percentages to the Connecticut State Department of Public Health (2020). Lucia shared that Nippawus often struggles with immunization fulfillment rates in part due to Guatemalan families not being familiar with such a requirement: “They are accepted into [a Guatemalan] school without evidence of a physical, without confirmation of immunizations.” For families seeking to enroll their children who have received immunizations, many lack previous health records but still must provide these records to fulfill the health requirements. Sara observed that the school has “had students that didn’t start the [school] year [on time] because they weren’t immunized.” Immunizations are such a critical need for MSF children and families accessing school and school resources that Sara suggested later in the interview, “I don’t know if we have the resources to do it, but if we can do an immunization clinic, I think it would be very good.”
There were also vision and dental needs. For instance, Lucia reported how Guatemalan students tended to have more issues with vision: They are finding that a large percent of students from Central America, . . . Their vision is impacted because there’s less protection from the sun . . . oftentimes [they] require eye glassware or corrective lenses. . . . Where they’re living, closer to the equator, [it puts them at increased risk] . . . Vision is a chronic issue.
Lucia also identified dental issues as another critical health concern among Guatemalan MSF students. She discussed the condition of one of the students’ mouths: I had a little child bump his lip last week. I wanted to make sure dentition was intact. He lifted up his lip and [his teeth] were black from the front [of his mouth] to the back. I’ve seen a few [black teeth] in the back in the past but [these were] black from the get-go.
Brokering Access to Physical Health Resources. School employees brokered families’ access to health care addressing physical health concerns through a range of actions. These included talking directly with clinics to make sure immunization requirements were being met, providing follow-up and support for families to remember and attend appointments and follow medical advice, providing health education opportunities, offering translation and interpretation at appointments, providing health education opportunities, offering transportation and accompaniment to appointments, making deep relationships, offering vision screening and eyeglasses, connecting families with dental clinics and providing information about how to access low-cost services or arranging free services at school, partnering with local organizations, and utilizing exemptions for immunization requirements. Importantly, these brokerage actions, including those aimed at prevention, often went beyond the provision of information, and instead comprised the work of connecting people with services directly.
For instance, school staff brokered access to immunizations and general health care by connecting families and resources by speaking directly with medical professionals regarding obtaining immunizations and specific treatments needed for students as well as by providing follow-up and appointment reminders. Lucia explained, Oftentimes, . . . they’re registering the child and [the clinic’s medical assistant will] call and ask if the parents provided me with a copy of their immunizations. . . . [In another example, I tell the clinic,] “That’s why we facilitated the appointment, confirming treatment for the child with scabies.” [Another example is] we’ve made an appointment for so-and-so, the medical assistant would call me, she’ll say, “This person has missed two appointments. Do you have a way of reaching out?” . . . [So I’ll call home to see] if the student went to the appointment or if the family member has gone and gotten their next Hepatitis B [shot]. . . . [I also tell them,] “Remember, you have the appointment” or “I happen to have noted that you had an appointment. How’d that go? I haven’t seen the paperwork.”
In addition, Lucia and the FRC offered a range of health education opportunities. Lucia taught issues related to reproduction to all students, noting that for reproductive care, once a year, I speak to the fourth-grade girls. Basically, about the changes that will be or have been occurring in their bodies . . . a male teacher or staff member that is really wonderful [gives the talk to the boys].
The FRC additionally provided family resources on reproductive education. Lucia also provided general health education to parents. For example, when students go home from school sick due to vomiting, she often calls the parents and instructs, “Remember, handwashing, number one. Wash the [door] handles.” The FRC similarly supported general health care education through programming such as teaching families about care for injuries.
Likewise, school employees provided transportation and went to medical appointments with families as needed, often forming deep relationships with them. Transportation, translation, and interpretation are provided officially through school or when Rocío, Ynes (a Panamanian FRC staff member), and the Family Liaison give rides and attend appointments with families outside of their work hours. For example, Ynes accompanied a mother to prenatal visits, built a relationship with her, and took her to the hospital when she was in labor. As Ynes showed, these visits were crucial when it came time for delivery: I have a mother . . . who had a baby. . . . She called me in labor and was afraid. I went to the hospital. Luckily, I had been going with her to the prenatal appointments and the doctor knew me. When I got there, they allowed me to stay until she had the baby.
Employees discussed the deep relationships they formed with families. Ynes recalled how one of the migrant mothers refers to her as tia-abuela (great aunt) because she had provided support to the woman’s now adult children as they made their way through the public schools. Ynes also talked about how she had been working with another parent for years and had become a godmother to her child, “We never baptized her through the Catholic Church, but we presented her in the church. She still says I’m the godmother. She calls me for anything.”
To address vision and dental needs, school employees worked with parents and collaborated with local organizations. For instance, Lucia worked with the Lions Club (an international nonprofit service organization) to provide free vision screening to low-income children. Lucia explained, “We’ve gotten authorization for the Lions Club to screen our children, hopefully next year, for vision” and to collect used eyeglasses at the school library. In another example, Lucia discussed providing guidance to the parents of a second grader who needed vision screening. She explained to the parents how they could go about seeing an optician and obtaining eyeglasses with Husky Health, Connecticut’s Medicaid and Children’s Health Insurance Program. Lucia recalled telling the parents: “This is what you need to do. [Your daughter] needs to go see a doctor.” . . . At that time, I ended up referring them to the local clinic and they were able to get eyeglasses with the help of the Lions Club. She got glasses within a month’s time.
The FRC also helped with vision (and hearing screenings). Regarding dental care, school employees brokered access to health care by directing students with dental issues to services at the local clinic that has a partnership with the town. However, Lucia shared, “Students’ families are restricted or limited by availability at the local clinic. It has a dental department, but it is [cost prohibitive].” Sara explained how she helps families sign up for additional dental services, In the beginning of the year, we give a package from [the local clinic] and we have two times per school year that a van comes that gives service to the students that have Husky [Health]. They get a cleaning and checkup.
Mark added, “Sometimes they’ll just bring all the equipment in, and we’ll empty a room and give them a space. They’ll run the dental clinic there.”
When immunization medical needs could not be addressed, school employees facilitated enrollment of undocumented families’ children without required health documentation if they were in the process of addressing the immunization. This provided the children with access to the food and resources made available at school. Lucia and Ynes reported that many MSF families lived in shared houses with other families, relatives, and acquaintances, which the State of Connecticut defines as homeless. While children from homeless families are permitted to enroll in school without meeting the school health requirements, Lucia extends this exemption to undocumented students in families living in their own dwellings. Lucia marked them as fulfilling the requirements, and shared her rationale for doing so: “If they are not [fulfilling the requirements], technically, they should not be allowed to come to school. . . . Do I do that? Are you kidding? We’ve got a guarantee of food here. Why would I do that?” Instead, Lucia, together with Ynes, Rocío, and the Family Liaison permit the students’ enrollment while they are “in the process of a catch-up schedule” or working on fulfilling the school health requirements.
Trauma and Psychosocial Health: Domestic Violence, Discrimination, and Language and Schooling Differences
The second group of health needs relates to MSF families’ psychosocial health, a more prominent concern in parent interviews than physical health. As is the case in understanding physical health, psychosocial health needs and health care access must be contextualized to the structural violence and legacy of historical trauma as well as economic inequality encouraging emigration (i.e., Campbell, 2016; Obinna, 2021). Psychosocial health needs include the need for care related to trauma caused by violence, discrimination, and language and schooling differences. Both school employees and parents clearly connected mental health risks to violence-related trauma, offering specific examples of how they were manifested at school (i.e., anxiety, attention issues, fears of being disliked). Similar connections were made to the trauma effects of bullying, assault, language differences, and a lack of familiarity with formal schooling opportunities.
Participants reported psychological trauma-related needs due to interpersonal violence. For instance, Mark commented that domestic violence was a problem faced by local families: “There’s been more domestic violence here in this school . . . students suffer from trauma, and you can see it based on their behaviors.” Lucia similarly emphasized that many children at school suffer from posttraumatic stress disorder, “There is not a child in this school who is not high risk.” She believed that Guatemalan MSF children had increased risk exposure of family violence or alcoholism. Daniela, a Mexican mother of two children, connected the domestic violence experienced in her household with effects on her children’s mental health. She shared that her elder daughter suffered from anxiety attacks, had difficulty keeping attention on her schoolwork, and was worried that people at school “would not like her anymore.” Daniela shared, Mi hija la mayor sí tenía un poco de problemas de comportamiento. Sí viene de—sufrimos un poquito de violencia doméstica, y ella como que tiene estos ataques de ansiedad. Y aquí en esta escuela le dio mucho eso. Lo que pasa que ella cuando pierde como la atención, como que dice, “Ya no me van a querer.” Ella siente que ya no la van a querer, ella reacciona así. Pero me ayudaron mucho en esta escuela. . . . Yo puse mucho de mi parte para ayudarle.
2
Along with trauma stemming from violence, an additional mental health concern related to trauma shared by most parents originated in how MSF children were treated by peers because they were Latinx and/or immigrant. Though Elizabeth, a Mexican mother of two, felt that discrimination was not a problem and reported that her children loved school, the remaining five parents had extensive comments on the matter. For instance, Nina, a Mexican mother of three children, talked about her children being bullied at school as a common occurrence: [Mis niños] han tenido un poquito de problemas con el bullying en todos lados, pero es por . . . maybe es las noticias o todo lo que está pasando. Como que a la gente mexicana o la gente latina los tiran más. Yo lo veo normal porque en todos lados hay—en el trabajo, en la escuela, en todos lados.
3
Yesenia, a Mexican mother with three children, talked about her first-grader constantly being physically assaulted by another girl, also a first-grader, on the school bus. Her daughter was frequently told that she needed to go back to her country and that she was not going to amount to anything because she was not born here: Siempre la trataban mal, siempre le decían que se regresara a su país, cosas así, feas. Tuvo bastantes problemas en el autobús porque una niña siempre la rasguñaba, la desgreñaba, le pegaba, le decía bastantes palabras malas, que ella nunca iba a llegar a ser nadie en esta vida porque ella no había nacido aquí y ella sí había nacido y podría ser presidenta de la nación.
4
Yesenia continued that talking to the other girl’s mother did not help, and Yesenia was unable to speak to the bus driver directly because she did not speak English and the driver did not speak Spanish.
Participants also reported trauma needs relating to the mistreatment of children who spoke Spanish or K’iche’, with many in the latter group not having experience in formal educational settings. For instance, Yesenia shared how her youngest daughter, who spoke Spanish, had many difficulties when she entered first grade a few years ago. Yesenia’s daughter cried every day for 4 weeks because she could not understand anyone at school: Cuando mi hija llegó de seis años que solo entró a primero, ella sabía leer y todo, pero solamente en español. . . . Ella hubo un tiempo donde unas cuatro semanas donde ella lloraba todos los días para ir a la escuela porque se le hacía difícil entender a los demás.
5
Likewise, Julia noted that Indigenous Guatemalan K’iche’-speaking students experienced stress, describing a situation when a student was put in a bilingual Spanish-English program and felt like “an outcast” in class because he spoke K’iche’. At the same time, Mark and Julia discussed how many Guatemalan students dealt with these language issues while also trying to learn how to deal with formal schooling, which could trigger mental health issues. As children acclimated to new routines and surroundings, they experienced feelings of discomfort and stress. For instance, Julia described a student for whom she was asked to support, “He had never gone to school in Guatemala, so he went into second grade, . . . because of his age that’s where they placed him.” Confirming the issue being common, Mark shared, I think the biggest struggle is students with interrupted formal education that are coming . . . Many of the families from Guatemala especially . . . have said that [they did not have access to schooling in their homeland] because the school is either far away—they couldn’t get there, or they didn’t have money to pay school fees. All those challenges.
Brokering Access to Psychosocial Health Resources. School employees brokered services for psychosocial health needs by working with parents, providing counseling, discussions with classmates to improve climate and receptivity to at-risk students, resources (i.e., trilingual books), and psychosocial health education and skill-building. Like brokerage for physical health needs, brokerage for psychosocial health needs included multipronged approaches from a range of school employees, including teachers, social workers, FRC staff, the Family Liaison, as well as other organizations.
In terms of brokerage of psychosocial health needs related to trauma, school employees and parents discussed how they worked together to address problems. For instance, Yesenia, whose daughter experienced harassment on the school bus, talked to the teachers who then conversed with the bus driver so they could monitor the children’s behavior on the bus and intervene when needed. With the school staff’s help, the situation got better.
As well, in the case of Yesenia’s other daughter, who cried for weeks because she could not understand anyone, the school psychologist and social worker provided assistance and conversed with the mother in Spanish. Yesenia shared that her daughter received emotional support to overcome the stress related to communication in a new language and environment: Con la ayuda de la trabajadora social y con la ayuda del psicólogo avanzó y se quedó en primer grado. Fue mucha ayuda la que me dio la escuela. El psicólogo [ . . . ] hablaba el español y el inglés bastante, él me ayudaba bastante.
6
Similarly, on behalf of the K’iche’-speaking student who felt like an outcast, the teacher offered assistance and expressed interest in the student’s educational experience as well as his emotional state and encouraged other students to include him. Julia offered support and, along with the teacher, met with the student’s mother. Julia explained how she assessed the needs of such families, “I gather a social history. I ask mom what brought them here, how they got here, what resources they had in Guatemala.” Julia referred this family to the Family Liaison who was able to procure trilingual books (K’iche, Spanish, and English) to help the boy begin his studies. These collaborated efforts improved the situation and reduced the burden of stress for the student.
In addition to these counseling and psychological services available at school, preventative and educational resources are offered. In her capacity as a school social worker, Julia offered social skills programming, the objective of which was to teach students mindfulness, stress coping strategies, and how to understand feelings. Additionally, the FRC organized various educational workshops or lectures for parents and/or students relating to psychosocial health education, including resources on self-care. The FRC collaborated with agencies from the county to provide classes on child development and parenting, programs for children from birth to age 3, workshops on family well-being and healthy cooking skills, and activities on “why is it important to spend time with your child.” Rocío explained, We always base activities around developmental [stages and issues] and [supporting] family engagement. . . . Being there for your child, how important it is. We try to always wrap it around the family.
She continued, “Tomorrow we have a program that is going to finish, [it was] 4 weeks of cooking healthy. . . . I always offer pizza for dinner like tonight.” Adriana, an aunt of one child, is part of a playgroup organized by FRC. Such workshops, Adriana explains, are also an opportunity for parents to meet each other, socialize, and share ideas about parenting. Adriana said she had positive experience with the group, remarking, “Me la he pasado bien.” 7
Barriers to Brokerage
While school employees helped families access care that they would otherwise likely be unable to obtain, there were obstacles to brokerage. These included a lack of language accommodation for K’iche’ speakers at school, a likely gap between families’ needs and school employee knowledge of those needs, and the same structural influences that resulted in the health needs and obstacles to accessing health care in the first place. These barriers provide insight as to how brokerage might be improved.
There is not a K’iche’-speaking personnel member at school, affecting brokerage efforts with this especially vulnerable group. The interviewed school personnel were all aware that the school served Kʼiche’ families, though that knowledge did not always extend to others in the district. Lucia explained, “Folks always assume that our children [and parents] are Spanish-speaking—that is the large minority, but in all actuality, they don’t speak Spanish. They speak Kʼiche’.” When dealing with the language barrier with K’iche’-speaking families at school, administrators said that they try to either have other families and friends come in who can interpret for them or they use Google’s translator website. Lucia’s experience illustrates the language barrier that K’iche’ speakers face when accessing health care and how she used pictographs to connect: That has been tough. Aside from speaking slowly, oftentimes parents will bring in someone who is Spanish-K’iche’ bilingual. I spoke to a parent recently. . . . I offered them information in Spanish, they declined it. I provided them with . . . a picture board . . . through gestures or demonstration, for head lice.
To help address accessibility for MSF families, Sara expressed the need for a “community resource guide” tailored to local needs and resources. She added that it should be available in English, Spanish, and K’iche’ since most of the school’s existing pamphlets and handouts were in Spanish and English only. She also noted that identification practices during intake in which the school employees could determine which families might benefit from resources provided to MSF families could be helpful.
While families and school staff reported putting forth good effort at communication and meeting MSF children’s needs, data suggested there may be a gap between families’ needs and school employees’ awareness of families’ needs. MSF families could lack knowledge about the resources available to them through the school or how and to whom they could address their needs to access such resources. For school personnel to connect families to resources, they had to know what families’ needs were, but the aforementioned linguistic inaccessibility for Indigenous families showed linguistically accessible interactions were uncommon. Mark highlighted additional reasons, such family reticence in interacting with government entities, for this gap: That’s why I love our FRC, because the team there is working hard to make parents feel comfortable coming in to school and sharing what their needs are. We do have a lot of resources that are at our disposal, but if we don’t know what specific families’ needs are, it’s hard to serve them. Like I said, bridging that gap between families that may be a little fearful about government systems [and us is important]. If we can bridge that gap, families feel comfortable coming here, feel comfortable to share their needs.
MSF families were often structurally vulnerable in several ways, such as needing to exercise the aforementioned fear of surveillance, being undocumented, and having low income—these intertwined vulnerabilities both affected their health needs and access to brokerage. Some families feared that their employer or the state might monitor them through their efforts to obtain medical care, which could lead to deportation. Lucia commented, “Sadly . . . our families live in fear of the possibility of being reported for just showing up for an appointment. . . .” Similarly, Mark recounted cases of parents being under surveillance: “I’ve seen parents that are undocumented that are wearing those incarceration ankle bracelets. . . . There also have been kids’ parents being sent back to their home country.” In addition, being undocumented encouraged parents to engage in fieldwork, which is often low-paying, because, as Ynes said, “Some farms are known not to check their workers’ legal status.” As a result, families often could not afford a phone and therefore did not have a working or local number. They sometimes provided the school phone numbers of relatives or friends as a contact method, which may further hinder communication and complicate brokerage. Rocío described related barriers to health care access: Transportation is always big because you got to get places. That transportation for them is not available . . . it’s tough. I would say money, that’s a struggle. I’m sure for everyone, especially if they’re coming here and then not having . . . that support.
Reaching medical sites for an appointment or coming to school from work during the day could be difficult or impossible for parents. Many families lived in close proximity to the school and could walk there for various programs. To take advantage of the school’s proximity in addressing MSF health needs, Mark suggested, “I think if each school had a school-based health center, that would be amazing and offer whatever other resources that we could share.”
Discussion
In sum, this research showed how school employees without an MEP bridge the gap between MSF family health needs and health care access, corroborating and advancing research on MSF health, MSF health care access, and school health broker models. Specifically, the school health broker model found in Florida exists in Connecticut even though the state lacks the Title I Part C funds supporting an MEP (Campbell-Montalvo & Castañeda, 2019). This work offers insight to support immigrant youth and families in schools, particularly in areas without an MEP or in underresearched areas with MSF families.
A first specific major contribution of this work is that it showed that a range of non–Migrant Advocate school employees, mostly Latinx women, brokered physical and psychosocial health care access in ways that were more pronounced and direct than in Florida. For instance, this study shows that a variety of Nippawus’ school employees, from a nurse to a social worker to an administrative assistant to FRC staff, played a crucial role in brokering health care access to families. This brokerage included efforts addressing psychosocial health care needs arising from domestic and interpersonal violence situations, similar to previous research (Campbell-Montalvo & Castañeda, 2019). The finding that such a broad range of school employees worked together and prioritized families’ well-being and offered a multipronged approach to supporting families that connected them to medical offices and community organizations extends previous work that focused on specific sets of employees (i.e., Campbell-Montalvo & Castañeda’s [2019] focus on Migrant Advocates; Villarreal Sosa’s [2019] focus on school social workers). Likewise, that school employee brokerage occurred through direct communication, deep connections, and relationships with local clinics is more pronounced here than in earlier research—specifically, the present study showed a more direct provision of care (i.e., dental services at school) and provider communication than that provided in Florida (Campbell-Montalvo & Castañeda, 2019). Through highlighting the deep social relationships staff had with families, this study also replicates that of Viladrich (2021) in which effective health care access brokers were ones that shared a language with, were willing to develop relationships with, and who generally cared about the people they were serving. It also speaks to previous work highlighting the role of Latinx women school employees and especially mothers in the provision of care in schooling contexts (e.g., Gallo & Link, 2015).
Second, this study furthered research on barriers to brokerage, particularly as it highlighted the importance of linguistic accessibility and other factors in school employee gaps in knowledge of MSF health care needs, as well as highlighted the importance of the physical location of the school as close to MSF homes in helping those families with the barrier of lacking transportation to access school resources. Specifically, the barriers to brokerage identified here add nuance and extend Campbell-Montalvo and Castañeda’s (2019) previous work by identifying a gap between families’ needs and school employees’ awareness of families’ needs as additional obstacles. It is likely that the gap between families’ needs and school employee knowledge is more pronounced than shown here, given that only parents accessing school resources were interviewed. The language inaccessibility affecting brokerage, even when many employees were aware of Indigenous Latinx students, showed that school knowledge of families’ languages is important but must be supported by policy and resources to back up access. However, it was not clear the extent to which district officials are aware of this language diversity and need, and given documented issues with accurately recoding student home languages, it is unlikely that school records reflect this language need (Campbell-Montalvo, 2020b). Further, there were no existing procedures to systematically identify migrant students during registration, and doing so could help the school be more aware of the students who could benefit from the documented brokerage. In addition, the impact of lacking transportation on accessing medical appointments is a barrier to brokerage documented here as well as in previous literature for many migrant families (Campbell, 2016; Campbell-Montalvo & Castañeda, 2019). In this case, the location of the school close to many families’ homes helped families access health care brokerage at school (even if they could not always access places farther away), highlighting the ecology of the site as relevant to the facilitation of brokerage.
In terms of potential broader impacts, the present findings, along with the implications of Campbell-Montalvo and Castañeda (2019), support efforts to extend school health broker programs. Focusing such interventions on areas with MSFs and others facing structural vulnerability could potentially significantly affect health and health care access for vulnerable peoples. While states vary on the specific ages at which children start attending school (5–8 years), and the age through which they are required to attend (16–18), attending school is compulsory in the United States (Education Commission of the States, 2010). This means that a school health broker model could offer provision of health needs and health care brokerage at a location nearly all children will access. Nesting a school health broker program within the Whole School, Whole Community, Whole Child Model could be a promising way to help school personnel acknowledge the social factors that affect children’s overall well-being and support their brokerage.
In considering the deployment of a school health broker model, the findings of this work and its predecessor provide insight that can be used to build a model of practices relating to identifying students to serve and increasing capacity to community with MSF families. For instance, like the required screening questions asked in states with MEPs (Campbell-Montalvo & Castañeda, 2019), protocols could be enacted to support the identification of MSF children to promote the provision of services to meet their health needs and well-being. This is especially needed given that MSFs can be a difficult population to reach due to their migratory patterns and possible unauthorized residence in this country. Furthermore, this research shows that coordinated ways of communicating and sharing ideas between school staff and parents is crucial in the school health broker model. Not meeting MSF students and families’ language needs would be detrimental in a national school health broker program. At Nippawus, improvements to meet language needs could include creating school information in the K’iche’ language, having parent nights with K’iche’ speakers, and/or hiring a full-time K’iche’-speaking school employee.
Regarding of limitations and future research, a limitation of this work includes that it excluded participants not speaking English or Spanish, meaning that we were not able to capture the experiences of Indigenous Guatemalan parents who also did not speak Spanish or English. This limitation must be considered when interpreting this work, given that much of the reporting about Indigenous Guatemalan students’ experiences comes from personnel experiences. Future research should gather data directly with Indigenous Guatemalans, investigate how the present findings of brokerage by a vast array of employees who establish deep relationships with the community and medical professionals might exist in other settings, as well as study the effects of a broker model intervention in schools.
Footnotes
Appendix A
Appendix B
Appendix C
Notes
Authors
REBECCA CAMPBELL-MONTALVO is a postdoctoral research associate at the University of Connecticut. She studies K–12 school resource access for linguistic, racial, ethnic, and immigrant/migrant minoritized groups as well as undergraduate STEM educational equity for women, underrepresented racial and ethnic minority, and LGBQTIA+ students.
OXANA SIDOROVA is an MA graduate of El Instituto: Institute of Latina/o, Caribbean, and Latin American Studies at the University of Connecticut. Her research interests include educational opportunities and experiences of bilingual and multilingual students in contexts of cultural and linguistic diversity.
MIRIAM VALDOVINOS is an assistant professor in the Graduate School of Social Work at the University of Denver. She studies gender-based violence experiences in Latina/x families and help-seeking processes for immigrant families engaging in social service programs.
XIAOMEI CONG is a professor and associate dean for research and director of the Biobehavioral Laboratory in the School of Nursing at the University of Connecticut. She studies the impacts of early life experiences on health outcomes in high-risk infants and families, and investigates biobehavioral and genomic mechanisms in managing pain, stress, and related symptoms in vulnerable populations.
RUTH LUCAS is an assistant professor in the School of Nursing at the University of Connecticut. She studies early mother–infant interactions and the biopsychosocial science of breast-feeding.