
Abstract
Internet-delivered mindfulness and relaxation training were compared with each other and a no-treatment control on stress, coping, and mindfulness measures. Participants (n = 114) were assessed before and after treatment, and their compliance with the intervention they received was tracked. The treatments were received at a time, place, and computer of the participants’ choosing with the proviso that three exercises be completed during each of three successive weeks. Both mindfulness and relaxation reduced stress, but only mindfulness training increased mindfulness and reduced emotion-focused coping.
Keywords
Universities have increasingly pursued universal prevention efforts to promote student wellness and inoculate against stress (CAS Professional Standards for High Education, 2012), with special attention paid to cost-effective methods (Springer & Phillips, 2006). Mindfulness-based interventions have received accelerating attention in the popular and professional literatures for both prevention and the treatment of physical and psychological ailments. Preliminary evidence suggests that they benefit healthy young adults as well as those experiencing distress by enhancing coping, reducing negative affect, and supporting physical vitality (Baer, 2003; Baer et al., 2008; Grossman, Neimann, Schmidt, & Walach, 2004; Segal, Williams, & Teasdale, 2002). Additional evidence that mindfulness training improves attention and test performance (Mrazek, Franklin, Phillips, Baird, & Schooler, 2013), retention of lecture material (Ramsburg & Youmans, 2014), and decision making under stress (Hafenbrack, Kinias, & Barsade, 2013) argues for its use as a universal intervention on college campuses. Online training—both inexpensive and accessible—is an attractive possibility.
Mindfulness has been described as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgementally to the unfolding of experience moment by moment” (Kabat-Zinn, 2003, p. 145). It is cultivated through meditation and attending to one’s experience in detail (Hanh, 1991). Practitioners are instructed to observe their thoughts, feelings, and sensations with acceptance and appreciation; refrain from elaborating mentally beyond their simple experience of the moment; and refocus on their immediate, subjective experience when their attention strays (Bishop et al., 2004; Kabat-Zinn, 2003).
In-person mindfulness training is the norm and, as one might expect, has been found to increase mindfulness (Baer et al., 2008). It also reduces anxiety (Shapiro, Brown, & Biegel, 2007; Shapiro, Schwartz, & Bonner, 1998) and stress in the short term, albeit less consistently in the long term (Chiesa & Serretti, 2009). Furthermore, mindfulness training increases empathy (Shapiro et al., 1998) and self-compassion (Neff, 2003) as well as improves self-control (Astin, 1997) and sleep quality (Klatt, Buckworth, & Malarkey, 2009; Wolever et al., 2012). All of the foregoing studies used wait-list controls. The active comparison group used most often in mindfulness research is relaxation training. Mindfulness and relaxation appear to have similar effects on stress and self-reported spiritual experiences; however, mindfulness decreases rumination and increases positive states of mind more effectively than does relaxation (Jain et al., 2007; Zautra et al., 2012).
Mindfulness training delivered to clients on an individual basis is a labor-intensive enterprise, so these interventions are usually presented in group formats such as in mindfulness-based stress reduction (MBSR; Kabat-Zinn, 1982) and mindfulness-based cognitive therapy (MBCT; Segal et al. 2002), incorporated into individual therapy models like acceptance and commitment therapy (Hayes, Strosahl, & Wilson, 1999), or have used a mix of group and individual work as with dialectical behavior therapy (DBT; Linehan, 1993). Although in-person delivery of mindfulness training may be effective, there are impediments to widespread dissemination. For example, few practitioners are adequately trained, and those who achieve competence are required to make a significant career commitment. Dimidjian and Linehan (2003) note that many of these therapies require trainers to keep a daily meditation or mindfulness practice (e.g., MBSR and MBCT) or attend regular treatment team meetings (DBT). In addition, university counseling center staff and resources are limited. Thus, mindfulness outreach interventions must compete with traditional group and individual offerings for space and time.
Internet delivery of mindfulness training may be a viable alternative if an evidence base can be established. It can be self-paced, less costly, and more accessible while additionally allowing for participant anonymity. Many clients may prefer this mode to a public venue, especially if the latter context implies a treatment for psychopathology or is in any way viewed negatively by the participant’s social network (Lau, Colley, Willett, & Lynd, 2012).
Several evaluations of Internet-delivered mindfulness have appeared in the literature. Some combine mindfulness with other treatments that address specific clinical conditions. Meyer et al. (2009), for example, used it in conjunction with cognitive restructuring and social skills training and found statistically and clinically significant reductions in depression. Thompson et al. (2010) similarly addressed depression and epilepsy, and Ljóttson et al. (2010) targeted irritable bowel syndrome. Improvements on key variables in these and similar studies do not permit teasing out the role of mindfulness from other treatment ingredients. More recently, pure mindfulness trainings, presented over the Internet, have conferred positive effects on psychological variables, such as depression and anxiety, though few have been conducted with college students or used active control conditions (Cavanagh, Strauss, Forder, & Jones, 2014).
Online mindfulness interventions may also involve differing levels of interaction with therapists and/or other participants, which can confound the effect of mindfulness practice per se with that of interpersonal support. Thompson et al. (2010), for example, used weekly conference calls and web-based discussion groups, and Ljóttson et al. (2010) employed student therapists for providing content clarification and encouragement. Zautra et al.’s (2012) intervention involved automated phone calls after an initial in-person training session, rather than Internet training. In contrast, Herzberg et al. (2012) reported strong positive effects from a curriculum that excluded any interpersonal interaction.
Certainly, the addition of interpersonal interaction might improve the outcomes of an exclusively Internet-delivered mode. Such deltas, if they are found to exist, would need to be viewed through the bifocals of cost benefit and cost-effectiveness (O’Connell, Boat, & Warner, 2009). Only one study has compared in-person and online mindfulness training. Over the course of 12 weeks, participants in Wolever et al. (2012) received 14 hours of training either in a traditional live group or in a synchronous (real-time) online mode. Both conditions produced similar benefits on measures of perceived stress, mindfulness, and sleep quality in comparison to a wait-list control condition. The online participants, however, showed additional improvement on heart rate variability and had lower attrition. Similarly, Lappalainen and colleagues (2014) found slightly superior effects from an online (vs. in-person) acceptance and commitment therapy curriculum on measures of depression, general health, and life satisfaction. In both cases, the common presumption of interpersonal factors leading to enhanced outcomes did not occur.
We chose to evaluate Internet-delivered mindfulness training, exclusively and without fortification with interpersonal elements, on outcomes commonly found in the mindfulness literature, in new college students. Relaxation training was selected as a high-demand control because it too is amenable to online delivery and focuses on similar outcomes (Beatty & Lambert, 2013; Devineni & Blanchard, 2005; Vincent & Lewycky, 2009). A head-to-head comparison of online mindfulness and relaxation training has not been attempted before. Relaxation training is already an established treatment, so it poses a difficult challenge for demonstrating the potential superiority of mindfulness training. We also used a no-treatment control to provide a reference point for comparing the two active treatments.
Our outcome battery also permitted us to examine experimental construct validity considerations as well as explore mindfulness change processes (Cook & Campbell, 1979; McNamara & Horan, 1986). Only mindfulness training, for example, should produce changes on mindfulness, or the theoretical basis for any changes relative to controls would be open to challenge. Moreover, mindfulness practice should not only lower stress but do so by providing a specific set of mental skills to cope with life’s challenges. Specifically, we hypothesized that participants in the mindfulness condition, who are taught ways of tolerating distress, would show reduced use of emotion-focused and avoidance coping strategies and increased task-oriented coping over and above participants in other conditions.
Method
Participants
Undergraduate students (n = 157) from a large Southwestern university in the United States were recruited using extra course credit as an incentive. Two-thirds were women, none older than 24, with the majority (81%) being 18 or 19. Half identified as White, 17% as Hispanic, 10% Asian American, 7% African American, 5% multiracial, 1% Native American, with 10% not responding.
Measures
The Perceived Stress Scale (PSS; Cohen, Kamark, & Mermelstein, 1983) is a 14-item Likert device that asks individuals to rate themselves on 5-point scales anchored by never to very often. Responses to items such as “In the last month, how often have you felt nervous and stressed?” are summed, with high scores indicating high stress. The device is frequently used to assess changes resulting from mindfulness practice (Klatt, Buckworth, & Malarkey, 2009; Shapiro, Brown, & Biegel, 2007) and shows good concurrent validity (Cohen et al., 1983). We found pretest internal consistency on all participants to be .87; test-retest reliability using pre-post scores of the no-treatment controls over the course of a three-week interval yielded a Pearson r of .60.
The Five Facet Mindfulness Questionnaire (FFMQ; Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) is a 39-item self-report device measuring the dimensions of observing, describing, acting with awareness, nonjudging of inner experience, and nonreactivity to inner experience; in combination, the five scales address the overarching construct of mindfulness. Though some mindfulness scales emphasize certain facets over others, the FFMQ purportedly provides a balanced measure of each aspect and thus a clearer picture of one’s overall level. The developers report good concurrent validity; we found the full scale score to have strong internal consistency (.86) and test-retest reliability (.71).
The Coping Inventory for Stressful Situations (CIIS; Endler & Parker, 1999) assesses three dimensions. In task-oriented coping, individuals act directly to resolve a stressful situation. Emotion-oriented coping taps self-centered and reactive behavior aimed at improving one’s mood. Finally, avoidance coping targets maladaptive mechanisms involving distraction or social diversion. Each scale contains 16 items in a 5-point Likert format anchored by not at all to very much. Respondents endorse how often they use a particular strategy to cope with stressful events (e.g., “Focus on the problem and see how I can solve it”). Its developers report that each subscale has strong psychometric properties in a college student population. We found internal consistencies of the CISS subscales to be .83 (task-oriented), .84 (emotion-oriented), and .71 (avoidance), with test-retest reliabilities of .75, .63, and .53, respectively.
Procedures
Participants were given a URL and created their own login code; all instructions and assessments were completed online. Assignment to treatment occurred in the order that they registered online (with the first assigned to mindfulness, the second to relaxation, the third to control). This unintentional cycling threat to randomness derived from a programming error; however, it appeared inconsequential since registration occurred evenly over a four-day period, attrition from the active treatments was relatively low and comparable, and all conditions showed pretreatment equivalence on all measures.
All exercises were presented over the Internet. Participants were allowed to complete exercises at a time and place of their choosing. To track participant compliance in the mindfulness and relaxation conditions, users were required to click on a link after listening to each exercise and were reminded to do so at the end of each exercise. This link appeared only after the exercise finished playing, and participants were unable to fast-forward or see the amount of time remaining in the exercise. Further, if not clicked within five minutes, the link disappeared.
At the completion of the three-week intervention, participants were directed to a debriefing page along with all intervention exercises and resources used in the study. Information on all treatments follows.
Mindfulness training derived from homework exercises used in Kabat-Zinn’s (1982) mindfulness-based stress reduction curriculum. Three guided meditations were provided to participants in the form of audio clips over the course of the three-week intervention with one new exercise being provided each week. Participants were instructed to perform the appropriate exercise on at least three different days during the week. The first exercise led participants to become aware of their sensations, including sights, sounds, and somatic sensations. In week two, participants performed the body scan, an exercise involving focusing one’s awareness on sensations occurring throughout the body and sequentially relaxing those areas. In week three, participants were led to observe their physical sensations, thoughts, and emotions without reaction or judgment. Exercises ranged from 12 to 20 minutes in length, with an average duration of 16 minutes. Brief introductions were given for each exercise, as well as ideas for practicing the skills learned.
Relaxation training used in the current study was Goto’s (2006) progressive muscle relaxation training derived from Jacobson’s (1925) original work. Participants in this condition were provided with guided audio instructions and were asked to practice three times each week. The relaxation audio clip lasted about 17 minutes. A text introduction and ideas for daily practice were provided as in the mindfulness condition.
No-Treatment Control Condition
Participants in this condition were instructed to return to the website after three weeks had passed to fill out posttest assessments. There were no requirements to complete any exercises.
Results
Preliminary Analyses
Statistical Power
Meta-analyses suggest that mindfulness training in comparison to a control condition leads to standardized differences of about Cohen’s d = .3 for stress and d = .4 for mindfulness (Carmody & Baer, 2009; Grossman et al., 2004; Sedlmeier et al., 2012). Analysis using G*Power 3.1 (Faul, Erdfelder, Lang, & Buchner, 2007) indicated that this study’s final participants who provided complete data yielded sufficient power (i.e., >.8) to detect effects (Cohen’s d = .35) at an alpha level of .01.
Attrition
Of 157 pretested participants, 114 (73%) completed all assigned treatment exercises and posttesting. Dropout rates in the active treatments were essentially equivalent (37% from relaxation and 38% from mindfulness). No-treatment control participants had no responsibilities other than pre- and posttesting and showed minimal attrition (5%).
To explore the possibility of systematic differences between dropouts and completers, pretest scores of participants who provided posttest data were compared with those of participants who dropped out prior to posttesting. Univariate ANOVAs showed no differences on any measure, and participants did not differ on any demographic variable assessed. In addition, univariate ANOVAs were conducted within each treatment condition to determine if participants remaining in a condition differed from those attriting from it. Again, no differences were found on any variable.
Of 43 dropouts, 34 attrited soon after beginning treatment while 9 did not complete all posttesting. The initial 34 participants provided little information from which to extrapolate posttest scores, and we deemed it most appropriate to listwise delete their data. For the remaining study, participants missing data ranged from a low of 0% for the variable stress to a high of 7% for mindfulness. To determine if data were missing at random (MAR) or missing completely at random (MCAR), a dummy variable representing missingness was computed and correlated with other study variables. No significant correlations were found, suggesting that omitted posttest data were MCAR. Missing data constituted less than 10% of total study data, an amount unlikely to bias results (Bennett, 2001), and were thus listwise deleted. Listwise deletion leads to a loss of power, but the remaining 114 participants provided sufficient power to detect significant effects.
Pretreatment Equivalence
ANOVAs were run on the pretest scores of all participants who provided posttest data, and no differences were found on any measure. Participants in each condition were thus equivalent at the outset of the study.
Treatment Effects
The means and standard deviations of each condition at pre- and posttest are presented in Table 1. Univariate analyses of covariance (ANCOVAs) were performed on posttreatment outcome measures of stress, mindfulness, task-oriented coping, emotion-oriented coping, and avoidance coping, using pretreatment scores as covariates. All slope assumptions were individually checked and met. Bonferroni adjustments were made to control for family-wise error, resulting in required obtained significance levels of .01 for omnibus tests and .016 for least squares difference post hoc tests to claim significance at the .05 level.
Mean Scores and Standard Deviations on Perceived Stress, Mindfulness, and Coping Scales Across Treatment Condition
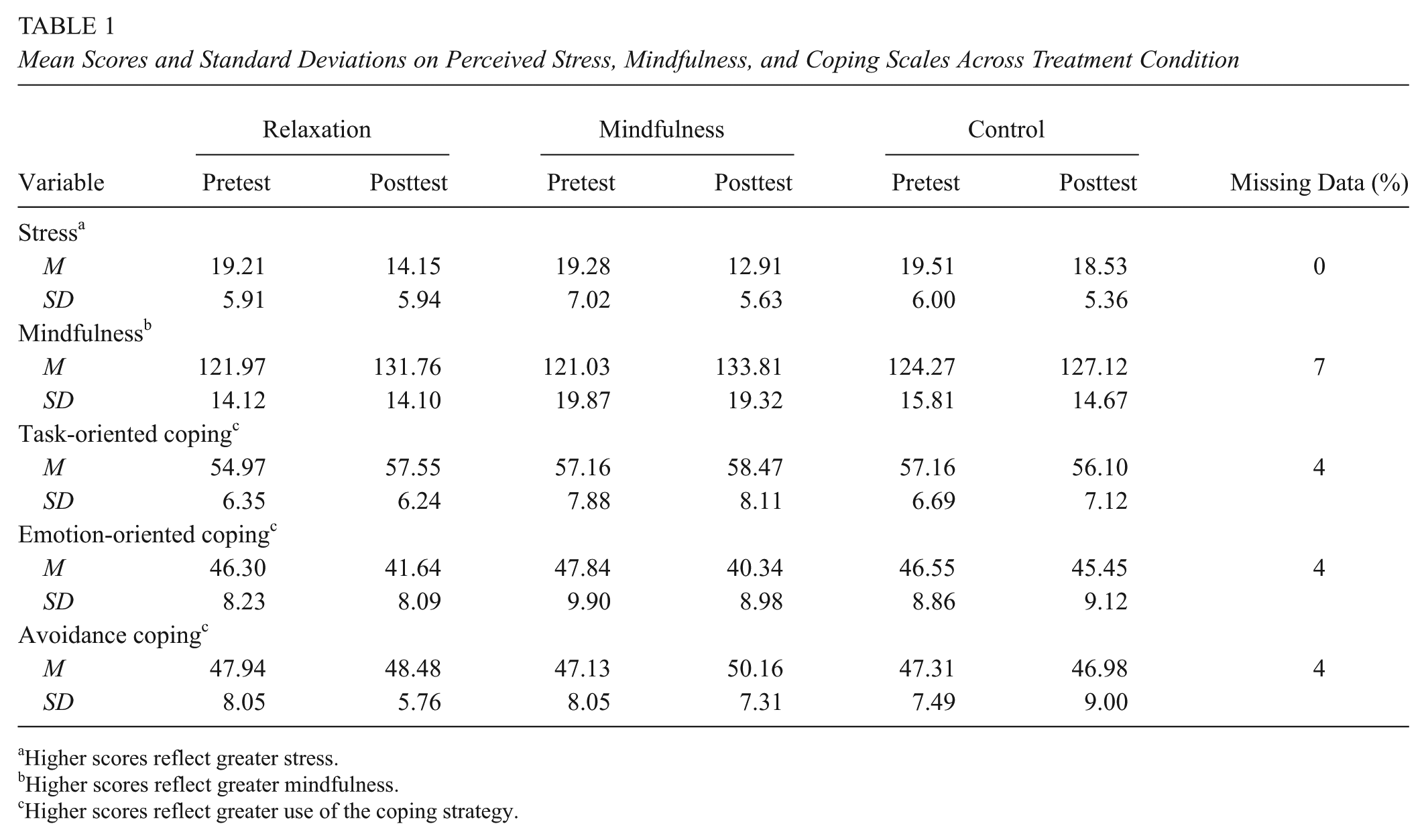
Higher scores reflect greater stress.
Higher scores reflect greater mindfulness.
Higher scores reflect greater use of the coping strategy.
Consistent with this study’s hypothesis, a significant treatment effect was found on stress F(2, 110) = 14.71, p < .001. Post hoc comparisons revealed that participants in both the mindfulness and relaxation conditions experienced lower stress than those in the control condition, p < .001, d = .99, and p < .001, d = .73, respectively (adjusted mean ± standard error, 12.94 ± .86 mindfulness, 14.22 ± .85 relaxation, 18.46 ± .69 control). Differences between the mindfulness and relaxation conditions were not significant.
A significant treatment effect was also observed on emotion-oriented coping, F(2, 110) = 6.93, p = .001. Mindfulness training led to significant decreases in emotion-oriented coping when compared to the control condition, p < .001, d = .70, while relaxation training did not, p = .023 (adjusted mean ± SE, 39.77 ± 1.26 mindfulness, 41.92 ± 1.24 relaxation, 45.62 ± 1.02 control). The mindfulness and relaxation conditions did not differ significantly from each other on this type of coping. No differences between conditions were observed on task-oriented coping, F(2, 110) = 3.18, p = .045, or avoidance coping, F(2, 110), p = .11.
Finally, a significant treatment effect was also observed on mindfulness, F(2, 110) = 4.43, p = .01. Participants in the mindfulness condition showed greater increases in mindfulness than those in the control condition, p = .006, d = .59, while relaxation participants did not, p = .049 (adjusted mean ± SE, 134.73 ± 2.33 mindfulness, 132.16 ± 2.29 relaxation, 126.26 ± 1.89 control). Differences between the mindfulness and relaxation conditions were again not significant.
On the Robustness of Treatment Differences
Two reviewers of this article noted that relaxation training approached significance on measures of mindfulness, emotion-oriented coping, and task-oriented coping, and in the absence of Bonferroni corrections, the superiority of mindfulness training would be less profound. Of course, the issue of family-wise error cannot be ignored; however, the similarities between the active treatments warrant further investigation.
Discussion
This study has shown that mindfulness can be taught online and that doing so is effective in reducing stress and aiding coping for university students. Our primary goal was to determine whether online mindfulness training could reduce stress. It did indeed do so but was not superior to relaxation training. Mindfulness and relaxation training both reduced stress with large effect sizes, suggesting clinically meaningful change, and did so across stress levels, suggesting utility for healthy students as well as those in acute distress. Although mindfulness training does not directly foster relaxation, it does teach nonreactivity to thoughts and feelings that might otherwise initiate a stress response (Sedlmeier et al., 2012; Selye, 1993). This broader focus could produce additional benefits.
Mindfulness training did lead to improved coping, for example, whereas relaxation did not. However, mindfulness was not demonstratively impressive here. We specifically hypothesized that mindfulness would enhance task-oriented coping while lowering both emotion-focused and avoidant coping. Relaxation training, lacking the relevant instructional foci, would presumably not affect coping. Although mindfulness did reduce emotion-oriented coping, no changes were observed on the other two dimensions. Since mindfulness increases empathy for oneself and others (Neff, 2003; Shapiro et al., 1998), perhaps it may reduce emotion-oriented coping without necessarily increasing proactive coping or reducing avoidance.
Moreover, since mindfulness training sequentially focuses on managing thoughts and feelings before taking thoughtful action, our intervention may have been too brief to produce later benefits. Future research might clarify process of change in longer training programs.
As might be expected, mindfulness training improved mindfulness in the absence of a similar effect from relaxation training. This finding may be viewed either as an additional outcome or as an independent variable manipulation check. Regardless, it supports the experimental construct validity of this study and the theoretical basis of mindfulness training. The effect size here (d = .59) falls in the medium-high range of what has been reported by in-person interventions (Carmody & Baer, 2009; Grossman et al., 2004; Sedlmeier et al., 2012), which is noteworthy given that it required negligible resources to achieve and is vastly more scalable.
Previous research has suggested that the effects of brief mindfulness training rival those of prolonged training (Carmody & Baer, 2009; Vettese, Toneatto, Stea, Nguyen, & Wang, 2009). Although our data arguably concur, we would rather advocate continuing use of constructive research designs wherein additional length or treatment elements would prove their worth in traditional evidence-based fashion. Our operational definition of mindfulness training did not incorporate other treatment modalities such as cognitive restructuring or yoga. Thus, our findings derive from a “pure” version of mindfulness training (extremely rare, on or off the Internet) and thus provides a non-confounded test of its effects. It would be very easy to evaluate the incremental effects (if any) of community support (see Herbert & Cohen, 1993), for example, delivered live or online via a simple constructive evaluation strategy.
The direct comparison of live versus online delivery is more complicated. Wolever et al. (2012) and Lappalainen et al. (2014) are the only studies attempting to do so. Apart from the need to deploy identical curricula, other methodological challenges abound. For example, many previous studies use small group samples that can easily violate an ANOVA’s independence-of-observation assumption, or use participants from clinical populations in settings that preclude random assignment, or are not delivered in even single- much less double-blind fashion, or exclusively use wait-lists controls that do not rule out nonspecific effects (see Chiesa & Serretti, 2009). Internet-based curriculum research need not be hampered by such until offline comparisons become involved.
Our findings have important implications. Online mindfulness training is a convenient and cost-effective wellness intervention. Such training can be provided universally, to all incoming students, or to select student groups in need. In addition, mindfulness training can be an additional ingredient employed by therapists or health center staff addressing complex client problems. If found effective generally, online mindfulness training could be tailored to address specific clinical conditions, further enhancing efficacy.
Stress contributes to both chronic and acute illness (Herbert & Cohen, 1993), is psychologically taxing (Glass & Singer, 1972), and has been found to negatively impact relationships (Repetti, 1989) and quality of life (Bolger, DeLongis, Kessler, & Schilling, 1989). In university students, stress has been found to contribute to risk behaviors and unhealthy coping (Paspaliaris & Hicks, 2010; Sun, Buys, Stewart, & Shum, 2011; Wilcox & Fawcett, 2012). Online mindfulness training has the potential to positively impact health outcomes for an entire campus community.
Finally, in regard to the robustness of treatment differences between this study’s relaxation and mindfulness trainings, Benson, Beary, and Carol (1974) note that many types of meditation involve similar autonomic training, and interventions teaching body awareness, such as progressive muscle relaxation, appear to increase mindfulness somewhat (Sedlmeier et al., 2012). In addition, relaxation training is commonly prescribed for the management of anger (Deffenbacher, Oetting, & DiGiuseppe, 2002) and anxiety (Park et al., 2013). Resulting improvements in coping are therefore not unwarranted. While both interventions may benefit coping, the pathway through which this effect is exercised may differ (e.g., reduction of arousal vs. insight into and tolerance of distress), conferring greater or lesser benefit depending on the situation. We look forward to future research clarifying the similar and distinct effects of these two treatments.
Footnotes
Authors
DAVID MESSER is a doctoral candidate in counseling psychology at Arizona State University, focuses his research on stress and coping in at-risk populations with an emphasis on mindfulness-based interventions.
JOHN J. HORAN is a professor of counseling psychology at Arizona State University. His research has always focused on the experimental evaluation of counseling interventions, but in more recent years he has concentrated on the construction, delivery, and evaluation of evidence-based resources via the internet.
WESLEY TURNER writes software and extracts value from data. His research focuses on machine learning techniques for board game analysis and play.
WANDA WEBER is a faculty member at Arizona State University. Her research focuses on excellence in teaching and learning in higher education.