
Abstract
The COVID-19 pandemic has disproportionately affected the health of people of color in the United States. In this study, we use national survey data (n = 1,844) to examine racial-ethnic variation in people’s worries about COVID-19 mortality and the mechanisms that underlie these differences. Consistent with stress theory, we find that Black and Latinx respondents are more likely than Whites to worry about the possibility that they, a romantic partner, or a child will die from the virus. Black and Latinx respondents are also more likely to report prior COVID-19 infection, to know someone who has tested positive for the virus, to work in essential jobs, to live in more densely populated counties with higher infection rates, and to contend with more same-race COVID-19 infections at the national level. Across these different layers of social context, however, only prior COVID infection and knowing someone who has tested positive for the virus are linked to greater worry about COVID-related mortality. Mediation analyses indicate the greater prevalence of prior infection among Black and Latinx respondents explains little of the gap in anticipatory stress, whereas approximately one-fifth of the Black-White and Latinx-White discrepancy in worries about COVID-19 mortality are attributable to the greater social connectivity of Black and Latinx respondents to family and friends who have been affected by the virus. We outline the implications of these findings for future scholarship.
The COVID-19 pandemic has thrown into sharp relief longstanding fissures in American society that place members of structurally disadvantaged groups at greater risk of poor health. Since its arrival in the United States, marginalized groups have borne the brunt of the virus, with Black, Latinx, and Indigenous people comprising a disproportionate number of those who have been hospitalized or killed by COVID-19 (Bassett, Chen, and Krieger 2021; Rubin-Miller et al. 2020). These stark, racialized patterns of morbidity and mortality are rooted in systemic racism (Bonilla-Silva 2022). People of color are more likely than Whites to reside in neighborhoods with fewer testing centers, to experience more barriers to treatment, and to receive medical care after the virus has progressed to its more acute stages (Artiga, Corallo, and Pham 2020; Lieberman-Cribbin et al. 2020; Rubin-Miller et al. 2020). These trends mirror persistent racial-ethnic disparities found across a broad spectrum of health outcomes over time, such that racism has been classified by social scientists as a fundamental cause of disease (Phelan and Link 2015).
Beyond its consequences for physical health and longevity, the COVID-19 pandemic has also ushered in a wave of mental health concerns across the United States (Czeisler et al. 2020; McGinty et al. 2020). The social antecedents of mounting rates of depression and anxiety are legion, including a combination of social isolation (Bierman and Schieman 2020), economic insecurity (Donnelly and Farina 2021), and uncertainty about the virus, among other factors. The findings of several recent studies suggest that concerns about contracting the virus also contribute to declining mental health (Cobb, Erving, and Byrd 2021; Zheng et al. 2021). Prior research indicates these types of future-oriented worries, or anticipatory stressors, are not only inimical to mental health, but also more concentrated among incumbents of disadvantaged social statuses (DeAngelis 2020; Grace 2020; Hicken et al. 2014). To date, it remains unclear why members of structurally disadvantaged groups are more likely to experience anticipatory stressors. Prominent scholars have speculated about the social origins of these group differences, proposing that exposure to stressors via social networks and media consumption represents key mechanisms driving discrepant patterns of anticipatory stress (Pearlin and Bierman 2013). To test these ideas, and to further expand the scope of social domains considered in relation to ruminative stress, we examine whether and how worries about COVID-19 mortality vary by race-ethnicity, and subsequently, the extent to which microlevel (e.g., health status, prior COVID infection), mesolevel (e.g., the presence of COVID-19 in social networks, working an essential job, living in an area with a higher infection rate), and macrolevel social contexts (e.g., racial-ethnic disparities in infection nationally) contribute to differences in anticipatory stress. Our findings contribute to a growing literature on status variation in anticipatory stressors and have broader implications for understanding the mental health burden of the pandemic for members of marginalized racial-ethnic groups.
Background
The Stress Process and Racial-ethnic Differences in Anticipatory Stressors
The stress process paradigm offers a guiding framework to understand how structural arrangements impinge on mental health and wellbeing (Pearlin et al. 1981). Stressors are the environmental insults that tax a person’s adaptive capacity and necessitate social and psychological readjustment. In recent years, a burgeoning literature has examined a novel category of stressor: those which are future-oriented, or anticipatory, in nature (Pearlin and Bierman 2013). Anticipatory stressors are social domain or role-specific worries that people have about the future, whether they are ever realized. These imagined futures operate on mental health by prompting continuous psychological arousal oriented toward monitoring and attempting to avert potential threats (D. Williams 2018). Consistent with the effects of other forms of stressors on mental health, research indicates that a range of anticipatory stressors including worries about discrimination, economic insecurity, goal-striving stress, and fears of victimization are associated with poorer mental health outcomes (Alang, McAlpine, and McClain 2021; DeAngelis 2020; Grace 2020).
A central proposition of the stress process model is that social statuses—including race-ethnicity, gender identity, and social class—stratify the variety and severity of stressors to which a person is exposed (Erving, Satcher, and Chen 2021; Pearlin and Bierman 2013). Although racial categories are biologically meaningless, they are imbued with social meaning. Scholars contend that race is a multidimensional concept capturing a group’s unique sociopolitical history and corresponding schemas of superordination and subordination that structure access to the social and material resources required to secure good health (Ray 2019; D. Williams 2012). Racial-ethnic patterns of stress exposure have been extensively documented by social scientists over the past several decades. This body of empirical knowledge provides evidence that people of color experience more chronic stressors (Turner and Avison 2003), traumatic events (Louie and Wheaton 2019), instances of major and day-to-day discrimination (Kessler, Mickelson, and Williams 1999), and death events (Turner and Avison 2003) than Whites. A similar racial-ethnic gradient can be observed with respect to pandemic-related strains (Perry, Aronson, and Pescosolido 2021).
Although the COVID-19 pandemic can be conceptualized as a macrostressor (Wheaton et al. 2013) affecting all members of society, to date, its consequences have disproportionately affected Black, Indigenous, and people of color in the United States. Administrative data indicate hospitalization rates for Black and Hispanic patients are three and four times higher, respectively, compared to Whites, whereas the death rate for both groups is twice that of White patients (Rubin-Miller et al. 2020). Further compounding racial-ethnic disparities in mortality, Black and Latinx people die at younger ages from COVID-19 than their White counterparts (Bassett et al. 2021). These racialized patterns of morbidity and mortality can be traced to structural racism, and, the corresponding, unequal distribution of both risks and resources across racial-ethnic groups (Bonilla-Silva 2022). In terms of the former, Black and Latinx people are more likely than Whites both to work in public-facing “essential” jobs that place them at greater risk of contracting the virus (Rogers et al. 2020), and to live in multiple-unit residential structures where it transmits more rapidly (Gould, Perez, and Wilson 2020; Gould and Wilson 2020). With respect to resources, in a study conducted using New York City coronavirus data, researchers found the number of tests administered increased with the proportion of White residents in a neighborhood (Lieberman-Cribbin et al. 2020). Yet, at the same time, demand for testing has been higher in predominantly Black and Hispanic neighborhoods, a circumstance which likely contributes to longer wait times found in these areas (Artiga et al. 2020). Longer wait times stemming from neighborhood disparities in test availability may be implicated in the finding that Black and Hispanic patients require more acute care (e.g., oxygen or ventilation) than White patients at the time they test positive for the virus (Rubin-Miller et al. 2020).
In their theoretical elaboration of anticipatory stressors, Leonard Pearlin and Alex Bierman (2013) speculate that individuals belonging to less advantaged status groups—including marginalized racial-ethnic groups—may be more vulnerable to this class of stressor. Research to date has borne out this proposition, as seen for instance, in the finding that racism-related vigilance is more common among Black and Latinx people than Whites (Hicken et al. 2014), or that future-oriented worries about economic security and exposure to traumatic events are elevated among members of marginalized racial-ethnic groups (Grace 2020). In the present context, research suggests that concerns about the pandemic are similarly more prominent among Black and Latinx Americans relative to Whites. A November 2020 survey by Pew Research Center revealed that Black and Hispanic respondents were more likely than Whites to indicate they were either somewhat or very concerned they would “get coronavirus and require hospitalization” (Funk and Tyson 2020). Subsequent research has further substantiated these racial-ethnic patterns, revealing that Black and Latinx individuals are significantly more likely than Whites to express concern about COVID-19 (Lin and Liu 2022), and to report the virus represents a threat to both their personal health and the health of their family (Niño et al. 2021). Consistent with this research, we expect to replicate these findings:
The Social Antecedents of Anticipatory Stress
In theorizing how anticipatory stressors emerge and take shape, Pearlin and Bierman (2013) use the example of an economic recession. They write that, “as economic hardships begin to affect relatives, friends, neighbors, or coworkers and are daily subjects of media reports, the misfortunes of others can result in anxiety and apprehension among those who have not directly experienced such strain” (p. 238). Whereas Pearlin and Bierman’s (2013) exposition points to social network and media exposure as the key factors generating anticipatory stress, it is plausible that any social domain which renders a person vulnerable to a stressor might enhance their worries about its occurrence in the future.
To this end, in the present study, we integrate Pearlin and Bierman’s (2013) theorizing with the “stress universe” (Wheaton and Montazer 2010; Wheaton et al. 2013), and its emphasis on different levels of social context. This model asserts that stressors operating at the microlevel, mesolevel, and macrolevel undermine people’s mental health and wellbeing. We extend this framework to posit that social factors nested across these different levels of social organization similarly propagate anticipatory stress, in this specific case, fostering greater concern about COVID-related mortality.
Microlevel context
The most fundamental unit of analysis in the stress universe is the microlevel, with its focus on individual lives and subjective perception. As people evaluate their susceptibility to different stressors, they may weigh how their own unique combination of status characteristics and personal behaviors put them at risk for different forms of stress. Individuals may draw upon available information regarding risk factors to form a cognitive model of the stressors they might probabilistically expect to face (Grace 2020). With respect to COVID-19, people with underlying conditions and those in poorer health are more likely to develop severe forms of illness and die (Emami et al. 2020; Rabin 2020). It follows that individuals with more pessimistic views of their health may have a greater propensity to ruminate on their risk of dying from the disease. Even among those who have previously contracted and cleared the virus, worries about COVID-19 mortality may linger. The weight of evidence suggests COVID-19 has enduring effects on health, as the virus has been linked to lung damage, heart attack, stroke, and multiple organ failure (Del Rio, Collins, and Malani 2020). Accordingly, one might worry that even if they or a loved one survive an initial bout with COVID-19, they may nevertheless succumb to secondary ailments caused by the virus. Thus, we hypothesize:
Mesolevel context
Perhaps the most expansive social dimension in the stress universe is the mesolevel. According to Blair Wheaton and colleagues (2013:307), this stratum contains “all levels of social reality ranging from those levels in which we are immediately embedded such as family, neighborhood, and workplace, to levels circumscribed by community or social boundaries, such as networks.” Pearlin and Bierman (2013) contend that as macrolevel threats begin to affect primary and secondary group members, individuals may begin to contemplate their own vulnerability to it. Mapping this hypothesis onto the COVID-19 pandemic, one would expect that individuals more intimately tied to significant others who have contracted the virus will experience greater trepidation about their own susceptibility. Affirming this point, research indicates that concerns about the pandemic are more acute among those who have lost someone to the virus (Lin and Liu 2022).
Two mesolevel factors long identified as fundamental sources of stress in American society are the workplace (Schieman, Milkie, and Glavin 2009) and neighborhoods (Boardman et al. 2001). In the case of the COVID-19 pandemic, we posit that individuals working in essential jobs, and those who reside in denser communities with higher rates of COVID-19 transmission, will be more likely to worry that they or a family member will die from the virus. In the wake of the pandemic, many jobs abruptly shifted from in person to remote work arrangements. Whereas many white-collar workers were able to continue working from the safety of their homes, essential workers—or those employed in front line occupations considered vital to the continuing function of the economy—were compelled to work in person as a condition of their employment. Though some essential workers are more economically advantaged (e.g., doctors), most are employed in lower wage occupations including those in food and cleaning services, manufacturing, and agriculture (Blau, Koebe, and Meyerhofer 2020; Rogers et al. 2020). The unifying characteristic of these occupations, however, is that their public-facing nature places individuals at greater risk of infection and premature mortality. An analysis of decedents during the early part of the pandemic indicates that excess mortality was markedly higher among people working in occupations categorized as “essential” relative to those working in other sectors of the economy (Y.-H. Chen et al. 2021). Given their heightened risk of exposure, individuals working in these positions may reasonably be more concerned about the prospect that they will become infected by the virus, and, in turn, pass it on to romantic partners, children, and other family members.
Stress research on neighborhood and community contexts typically examines how ambient stressors including noise pollution, toxins, and overcrowding erode mental health (T. Hill and Maimon 2013). With respect to the pandemic, some communities have been more affected than others in terms of the concentration of cases, hospitalizations, and deaths (Khanijahani and Tomassoni 2021; Torrats-Espinosa 2021). We suspect that just as media exposure to macrolevel crises can prompt individuals to reflect on their own susceptibility to an event (Pearlin and Bierman 2013), people may similarly be attuned to the issues unfolding in their local geographic region. As such, we posit that individuals living in more densely populated counties, characterized by higher levels of viral transmission, may be more vigilant about the presence of the virus, and, as a corollary, concerned about their vulnerability to it. Guided by these ideas, we hypothesize:
Macrolevel context
The macrolevel encompasses national and global events (Wheaton et al. 2013). At the outset of the pandemic, there was a great deal of uncertainty about primary vectors of transmission, or how to effectively treat the virus. Indeed, prior to the advent of a vaccine, the period between symptom onset and death for COVID-19 decedents was a mere two-and-a-half weeks (Zhou et al. 2020). As the first wave of the pandemic crashed into metropolitan areas in March and April 2020, over 1,000 Americans died each day from the virus (New York Times 2020). This prodigious loss of life, and the existential threat posed by the pandemic, weighed on many people’s minds. International research suggests that individuals more attuned to information about the pandemic report greater anxiety about dying from COVID-19 (X. Chen et al. 2022). In view of these insights regarding the effects of macrolevel trends on individual worries about the virus—and due to its relevance to understanding racial-ethnic disparities in anticipatory stress—we contend that higher levels of COVID-19 infection among members of one’s racial-ethnic group at the national level may similarly foster concerns about COVID-related mortality. Specifically, we hypothesize:
Racial-ethnic Differences in Contextual Factors and Corresponding Worry about COVID-related Mortality
The foregoing exposition highlights several possible mechanisms that contribute to anticipatory stress about the COVID-19 pandemic. Following from these arguments, in this study we examine whether and how racial-ethnic differences across microlevel, mesolevel, and macrolevel contexts contribute to greater worry among members of marginalized racial-ethnic groups that they or a family member will die from the virus.
Individual risk
Black and Latinx Americans are more likely to report individual-level risk factors that predispose people to more severe COVID outcomes including worse health, a greater burden of preexisting conditions, and prior infection. Racial-ethnic differences in morbidity and premature mortality are longstanding features of the epidemiological landscape. Due to economic marginalization and unequal healthcare access, Black and Latinx individuals generally report poorer self-rated health compared to White people (Hummer, Benjamins, and Rogers 2004). In a similar vein, higher rates of COVID infection among Black and Latinx Americans have been evident since release of race-specific data (Eligon et al. 2020; Mays and Newman 2020). As such, we predict:
Networks, work, and neighborhoods
Pearlin and Bierman (2013) maintain that disadvantaged social groups are more vulnerable to anticipatory stressors because members of these groups have a greater propensity to be socially connected to similar others grappling with stressful circumstances. Evidence to date suggests that racial disparities in COVID-19 infection and mortality have translated into racial-ethnic differences in network exposure to the virus. A national survey conducted in November 2020 found that 54 percent of Americans know someone who has either been hospitalized or died from the virus (Funk and Tyson 2020). Further decomposition of this figure, however, reveals striking racial differences. Compared to roughly half of White (49 percent) and Asian American (48 percent) adults, a more considerable 61 percent of Latinx and 71 percent of Black Americans report knowing someone who has become seriously ill or died from the virus. The greater proportion of Black and Latinx Americans who know someone who has been hospitalized or died from the virus is reflective of two interrelated factors: (1) racially homophilous social networks and (2) the disproportionate share of Black and Latinx people among COVID-19 hospitalizations and decedents (Gold et al. 2020). In terms of the former, the racially homogenous networks found in the United States are a function of both institutionalized racism—manifested, in the form of residential segregation—and a tendency among people to form demographically homophilous ties (Smith et al. 2014).
The historic, economic marginalization of Black and Latinx Americans is responsible for their concentration in occupations that place them at elevated risk of infection with the virus. Black and Latinx people are overrepresented in industries deemed “essential” including agriculture, food services, construction, and home healthcare (Rogers et al. 2020; J. C. Williams et al. 2020). The risky nature of these occupations, coupled with governmental failure to provide personal protective equipment to workers, contributes to the elevated rates of COVID-19 infection found in Black and Latinx populations (J. C. Williams et al. 2020). Residential segregation further exacerbates racial disparities in COVID exposure. Redlining policies enacted in the 1930s created predominantly Black and Latinx neighborhoods characterized by multiple-unit housing, greater population density, and unsafe living conditions. The resultant clustering of residents by race-ethnicity in these neighborhoods has led to COVID-19 hotspots marked by higher rates of infection among Black and Latinx residents (Rogers et al. 2020). Based on these findings, we propose:
National trends
At a national level, racial-ethnic disparities in COVID-19 infections, hospitalizations, and deaths have been evident since the beginning of the pandemic (Gold et al. 2020). As a result, we expect that Black and Latinx respondents will contend with higher rates of same-race COVID-19 infections nationally:
To date, few studies have examined how discrepancies in contextual factors give rise to racial-ethnic differences in anticipatory stress about COVID-19. A notable exception, however, can be observed in recent work by Zhiyong Lin and Hui Liu (2022), which finds that greater concerns about COVID-19 among older Black and Latinx Americans are driven in part by a greater likelihood among members of these groups to know someone affected by the virus and, to a lesser extent, by preexisting health status. These findings indicate that both mesolevel and microlevel contexts can contribute to racial-ethnic disparities in anticipatory stress. With respect to the macrolevel, Black and Latinx people who closely follow news about the pandemic are more likely to report psychological distress than Whites (Bauldry and Stainback 2022). Albeit suggestive, these higher levels of distress may be rooted in greater awareness of racial-ethnic disparities in COVID-19 infection among Black and Latinx Americans, widely reported by the media since the early stages of the pandemic (Eligon et al. 2020; Mays and Newman 2020). As such, we suspect that at a national level, higher infection rates among Black and Latinx Americans will lead members of these groups to be more likely than Whites to worry they or a loved one will die from the virus. Extrapolating from both the findings of these studies and Pearlin and Bierman’s (2013) theoretical elaboration of anticipatory stressors, we predict that if Black and Latinx people are more likely to face risk factors across different levels of social context, they will express greater apprehension about COVID-related mortality. Thus, we hypothesize:
Data and Methods
Sample
This study analyzes survey data collected from a national, nonprobability, sample of 2,000 Americans. Data were collected by Qualtrics, a professional survey company, between July 8, 2020 and October 13, 2020. Situating these data historically, this period immediately followed the initial wave of the pandemic and coincides with the virus’ second surge during the summer of 2020 due to the Delta variant. A quota sampling strategy was used to recruit a sample approximating the racial-ethnic, gender, age, and income distribution of the American population based on estimates from the U.S. Census Bureau. Qualtrics maintains a number of online panels comprised of hundreds of thousands of individuals who represent different segments of the population. Respondents are invited to participate in surveys for which they meet study criteria and have the ability to opt in to those of interest to them. Of the 915,048 panel members who were eligible for the survey as residents of the United States and who were at least 18 years of age, a total of 82,354 individuals were contacted to generate a sample of 2,000 respondents. The composition of the sample compares favorably to 2019 Current Population Survey (CPS) Benchmarks (see Supplemental Appendix A). While Qualtrics samples have been prominently featured in recent epidemiological research (Czeisler et al. 2020), the self-selected nature of the sample poses clear limitations to the generalizability of the study, which we address in greater detail in the Discussion section.
For the present analyses, we restricted the sample to include only those respondents who identified as Black, Latinx, or White (n = 1,844). Table 1 presents sociodemographic characteristics for the sample alongside descriptive statistics for key study measures. In terms of race-ethnicity, 67.7 percent of the sample identify as White, 13.5 percent as Black/African American, and 18.8 percent as Hispanic/Latinx. Turning to contextual factors, at the microlevel, approximately 20 percent of respondents report being in poor health, while nearly 7 percent have previously contracted COVID-19. At the mesolevel, over one-quarter of respondents have had a family member or friend test positive for COVID-19, approximately one-quarter identify as essential workers, and, on average, respondents reside in counties where the infection rate is approximately 18.6 people per 100,000 and the average population density is 4,932 (comparable to Cleveland). At the macrolevel, the same-race COVID-19 infection rate in the United States for an average respondent is 352.3 per 100,000.
Descriptive Statistics for Sociodemographic Measures and Key Study Variables (N = 1,844).
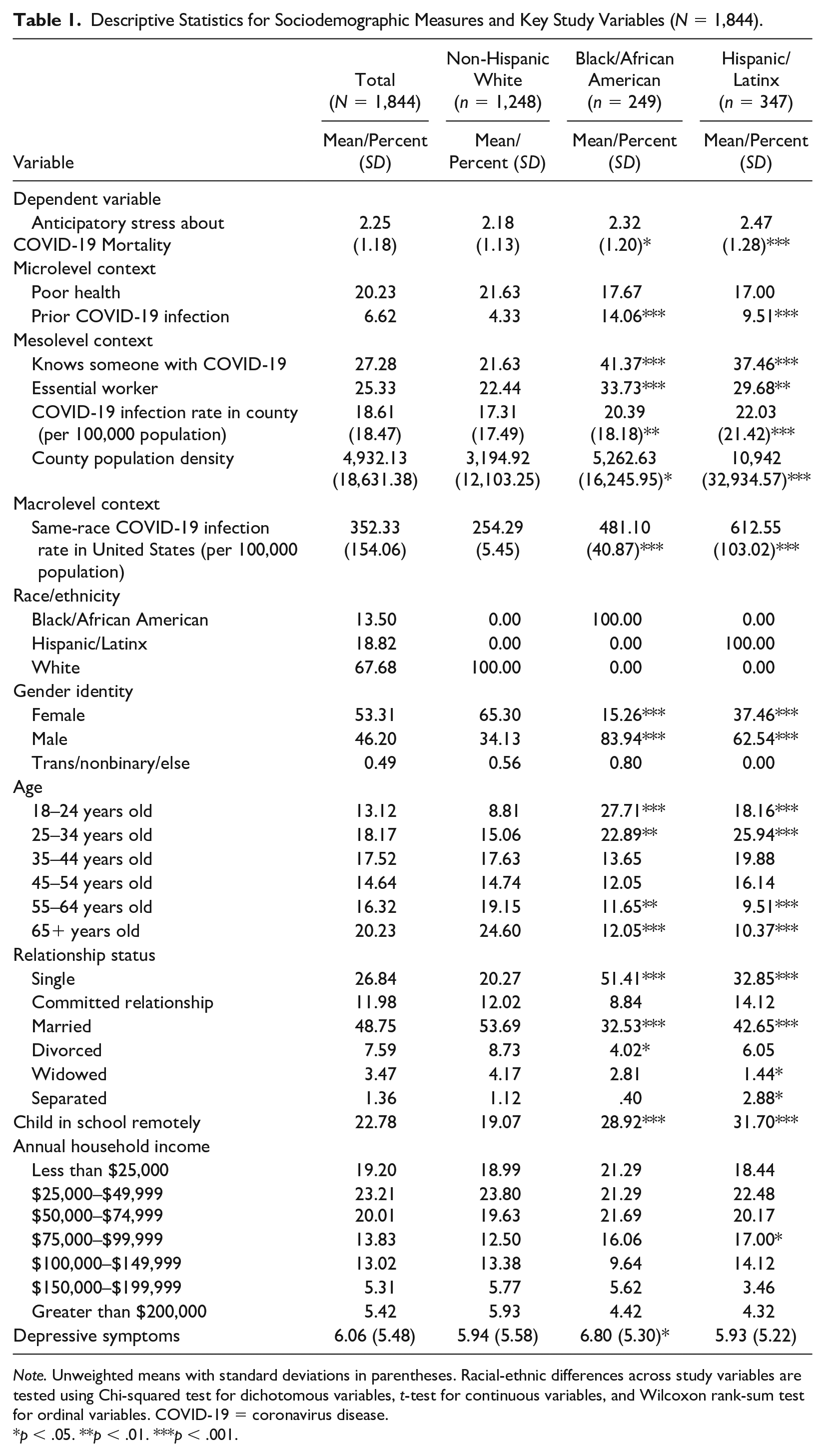
Note. Unweighted means with standard deviations in parentheses. Racial-ethnic differences across study variables are tested using Chi-squared test for dichotomous variables, t-test for continuous variables, and Wilcoxon rank-sum test for ordinal variables. COVID-19 = coronavirus disease.
p < .05. **p < .01. ***p < .001.
Measures
Anticipatory stress about COVID-19 mortality
We assess respondents’ worries about COVID-19 mortality using three items. Respondents were asked, “When you think about the future, how frequently do you worry about the following”: with the three items inquiring about (1) “dying from COVID-19,” (2) “your romantic partner dying from COVID-19,” and (3) “one of your children dying from COVID-19.” Response categories were based on the day-to-day discrimination checklist used in R. Jay Turner and William Avison’s (2003) research and range from 1 = never to 5 = almost always. Responses on these items were used to generate an anticipatory stress about COVID-19 mortality scale by calculating the average for each respondent (α = .86, eigenvalue = 2.36). Higher scores on the scale are indicative of greater worry about COVID-related mortality. Results from a principal-component factor analysis of constituent items can be found in Supplemental Appendix B.
Microlevel context
To ascertain microlevel factors, we include a binary variable for poor health (1 = fair/poor, 0 = excellent/very good/good) based on a measure of self-reported health. In a similar vein, we also include a dichotomous variable for prior COVID-19 infection, derived from a respondent’s self-report of whether they have ever tested positive for the virus (1 = yes).
Mesolevel context
We assess mesolevel context using four different measures. Knows someone with COVID-19 is derived from a combination of three items that ask about the COVID-positive status of significant others in a respondent’s life. Respondents were asked the following: “Has anyone in your immediate family tested positive for COVID-19?,” “Has anyone in your extended family tested positive for COVID-19?,” and “Have any of your close friends tested positive for COVID-19?” Responses across these items were used to create a binary variable where respondents who replied affirmatively to any one of these queries were coded 1 = yes. Essential worker status is self-reported in response to the question “Are you considered an essential worker?” (1 = yes). We created a measure of COVID-19 infection rate for the county in which a respondent resides based on the rolling seven-day average of new cases per 100,000 in a respondent’s home county on the date they participated in the survey (mean = 18.61, SD = 18.47). Population density is calculated by dividing the population of a respondent’s home county by its area in square miles (mean = 4,932.13, SD = 18,631.38).
Macrolevel context
We include one macrolevel factor: same-race COVID-19 infections in the United States. This measure was created by assigning the value for the infection rate of a respondent’s racial-ethnic group at the national level (per 100,000 population) during the month they participated in the survey (mean = 325.33, SD = 154.06).
Race-ethnicity
Respondents’ race-ethnicity (self-reported) is measured using a set of dichotomous indicators where Black/African American (=1) and Hispanic/Latinx (=1) respondents are compared to Whites (=0).
Controls
In multivariable models we adjust for factors that might otherwise confound the association between race-ethnicity and COVID-19 anticipatory stress. Gender identity is measured as female (=1), trans/nonbinary/else (=1), or male (=0). Age is measured using a set of dichotomous variables where respondents 65 years of age and older (=0) are compared to those between 18 to 24 years old (=1) and 55 to 64 years old (=1). Information about respondents’ relationship status is used to compare respondents who are single (=0) with those who are in a committed relationship (=1), married (=1), divorced (=1), widowed (=1), or separated (=1). The presence of a child in school remotely was assessed by an item which asked, “Have you had to homeschool your children due to COVID-19?” (1 = yes). Annual household income (self-reported) is measured using a set of binary variables where respondents making less than $25,000 (=0) are compared to those making between $25,000 to $49,999 (=1) and $200,000+ (=1). Finally, depressive symptoms are measured using the Center for Epidemiological Studies of Depression (CES-D) Scale (Levine 2013) seven-item short form. CES-D items ask about symptoms experienced over the course of the past week (e.g., feeling depressed, restless sleep), with response categories ranging from 0 = rarely or none of the time to 3 = most or all of the time. Responses were summed as per convention to create a scale of depressive symptoms (α = .91, range = 0–21).
Analytic Plan
Our analysis proceeds in several stages, addressing each hypothesis in turn. To discern racial-ethnic differences in worries about COVID-19 mortality (H1), as well as the associations between microlevel, mesolevel, and macrolevel contexts and this outcome (H2–H4), we estimate a series of ordinary least squares (OLS) models where COVID-19 anticipatory stress is regressed on race-ethnicity and contextual variables. Next, we regress contextual variables on race-ethnicity to assess racial-ethnic differences across microlevel, mesolevel, and macrolevel factors (H5–H7). To gauge the extent to which racial-ethnic differences across disparate levels of social context contribute to group-level variation in worries about COVID-19 mortality (H8), we use a multiple mediation method (Breen, Karlson, and Holm 2013) that allows us to parse the unique contributions of each mediator when considering all mediational pathway simultaneously. One other adjustment requires comment. Although the composition of sample largely approximates demographics from the 2019 CPS, there are several discrepancies between the analytic sample and the population, most notably with respect to gender identity, age, and household income. To account for these differences, all regression models use poststratification weights to ensure the analytic sample reflects the demographic composition of the American population (Bergmann 2011).
Results
Racial-ethnic Differences in Anticipatory Stress about COVID-19 Mortality
Table 2 presents results from OLS models where anticipatory stress about COVID-19 mortality is regressed on race-ethnicity and contextual variables. Consistent with Hypothesis 1, estimates from Model 1 indicate Black (β = .19, p < .05) and Latinx (β = .29, p < .001) respondents are significantly more likely than Whites to worry about the possibility that they, a romantic partner, or a child will die from COVID-19. Net of controls, the difference between Black and White respondents is nearly one-fifth of a standard deviation on the anticipatory stress scale, whereas the discrepancy between Latinx and White respondents is closer to one-quarter of a standard deviation on this outcome.
OLS Regressions of Anticipatory Stress about COVID-19 Mortality on Race-ethnicity and Contextual Factors (n = 1,844).
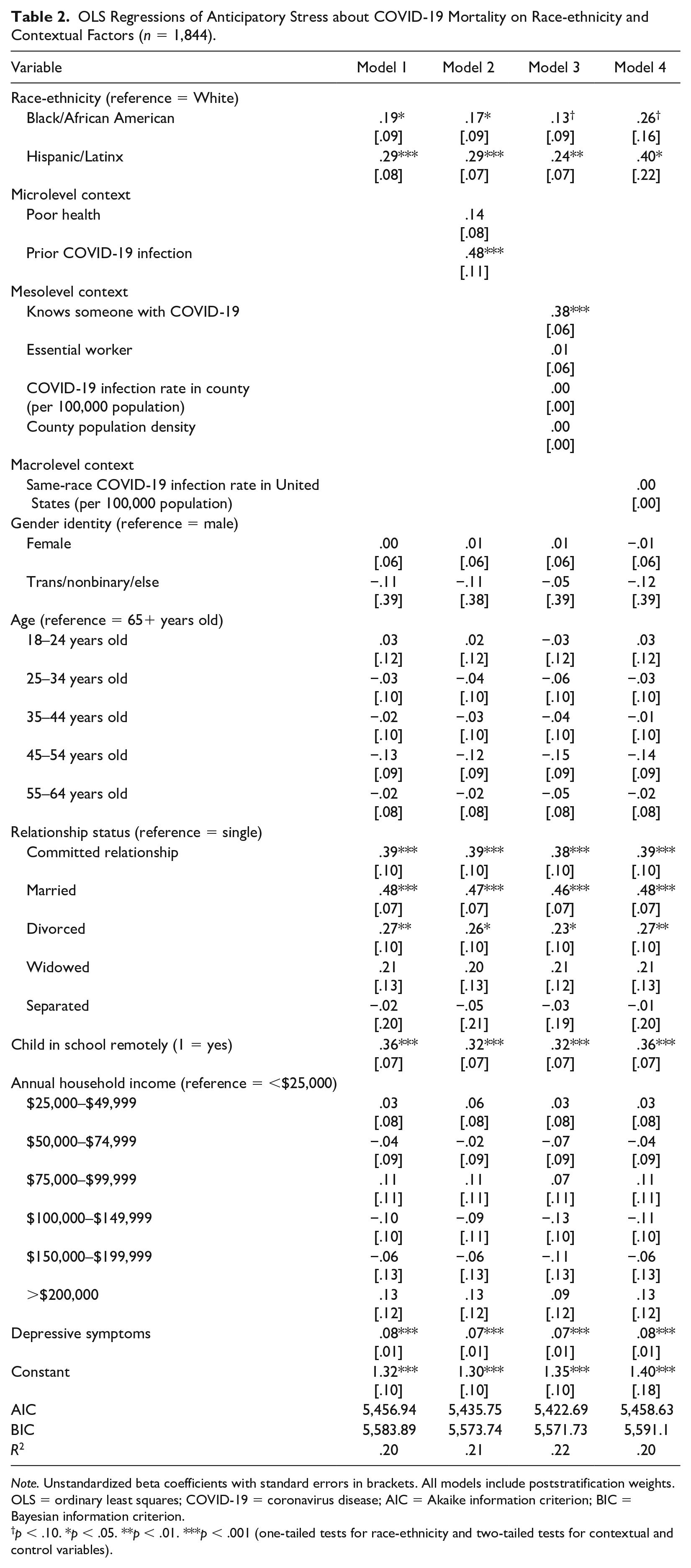
Note. Unstandardized beta coefficients with standard errors in brackets. All models include poststratification weights. OLS = ordinary least squares; COVID-19 = coronavirus disease; AIC = Akaike information criterion; BIC = Bayesian information criterion.
p < .10. *p < .05. **p < .01. ***p < .001 (one-tailed tests for race-ethnicity and two-tailed tests for contextual and control variables).
Turning to other key predictors, relative to those who are single, respondents who are in a committed relationship (β = .39, p < .001), married (β = .48, p < .001), or divorced (β = .27, p < .01) are more likely to express concern that they, a romantic partner, or child will succumb to the virus. In a similar vein, respondents with a child in school remotely have anticipatory stress levels that are almost one-third of a standard deviation larger than those without a child in school remotely (β = .36, p < .001). Respondents who are more depressed (β = .08, p < .001) are also more inclined to worry about COVID-related mortality.
Associations of Contextual Factors with Anticipatory Stress about COVID-19 Mortality
Table 2 also features the associations between contextual factors and respondents’ level of worry that they or a family member will die from the virus. Providing partial support for Hypothesis 2, in Model 2 respondents with a prior COVID infection are over one-third of a standard deviation more likely than those who have not been infected to worry about COVID-19 mortality (β = .48, p < .001), whereas poor health is not significantly associated with this outcome.
Moving to mesolevel factors in Model 3, respondents who have had a family member or friend infected by COVID-19 report levels of anticipatory stress that are approximately one-third of a standard deviation higher than among those without such connections (β = .38, p < .001). Although ancillary analyses without controls suggest that essential worker status is associated with significantly higher levels of anticipatory stress about COVID-19 mortality, as depicted in Model 3, this relationship is not robust to adjustment for basic sociodemographic factors. In a similar vein, neither the COVID-19 infection rate of a respondent’s home county nor its population density is significantly associated with worries about COVID-19 mortality. Cumulatively, these results provide limited evidence to support Hypothesis 3.
With respect to macrolevel context, in Model 4 there is a negligible association between the prevalence of same-race COVID-19 infections at the national level and respondents’ worries about COVID-19 mortality. This null finding fails to provide support for Hypothesis 4.
Racial-ethnic Differences in Microlevel, Mesolevel, and Macrolevel Contexts
Table 3 presents average marginal effects (AMEs) for race-ethnicity from a series of regression models that examine the associations between race-ethnicity and contextual factors. Contrary to expectations, there are no significant racial-ethnic differences in poor health (Model 1). More consistent with Hypothesis 5, however, Black respondents have a seven-percentage point higher probability of prior COVID infection relative to White respondents (AME = .07, p < .001), whereas Latinx respondents have a five-percentage point higher probability of prior infection compared to Whites (AME = .05, p < .01).
Average Marginal Effects from Regressions of Social Context Variables on Race-ethnicity (n = 1,844).
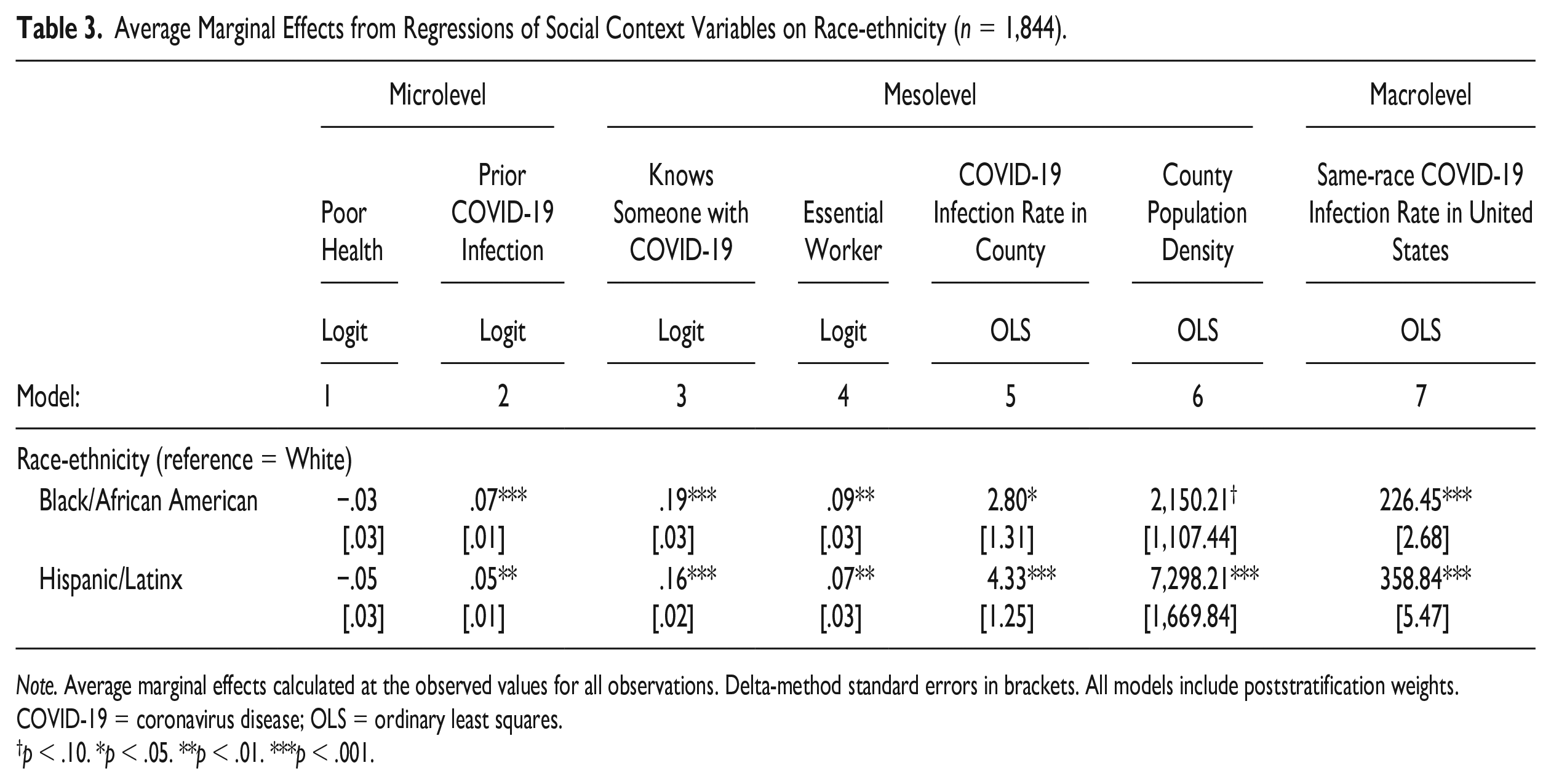
Note. Average marginal effects calculated at the observed values for all observations. Delta-method standard errors in brackets. All models include poststratification weights. COVID-19 = coronavirus disease; OLS = ordinary least squares.
p < .10. *p < .05. **p < .01. ***p < .001.
At the mesolevel, Black respondents hold a 19-percentage point higher probability of having a family member or friend test positive for COVID-19 compared to White respondents (AME = .19, p < .001). Analogously, this probability is 16 percentage points higher among Latinx respondents (AME = .16, p < .001). Similarly aligning with expectations, Black respondents have a nine-percentage point higher probability of being an essential worker relative to Whites (AME = .09, p < .01), while Latinx respondents have a seven-percentage point higher probability of working in a job considered essential (AME = .07, p < .01). Both Black and Latinx respondents live in counties with significantly higher COVID-19 infection rates (respectively, AME = 2.80, p < .05 and AME = 4.33, p < .001) compared to White respondents and, similarly, reside in more densely populated counties (respectively, AME = 2,150.21, p < .10 and AME = 7,298.21, p < .001). In total, these results fully support Hypothesis 6.
Moving to macrolevel context, in support of Hypothesis 7, same-race COVID-19 infections in the United States are higher among Black (AME = 226.45, p < .001) and Latinx respondents (AME = 358.84, p < .001) relative to White participants.
Mediating Effects of Social Context on Racial-ethnic Differences in Anticipatory Stressors
Table 4 presents the results of multiple mediator tests that examine the extent to which differences in contextual factors contribute to racial-ethnic variation in anticipatory stress about dying from the virus. Although there were significant racial-ethnic differences across all contextual variables with the exception of poor health (see Table 3), only prior infection and knowing someone with COVID-19 were associated with anticipatory stress about COVID-related mortality (see Table 2), and thus able to serve as mediators.
Mediation Tests for Racial-ethnic Differences in Anticipatory Stress about COVID-19 Mortality.
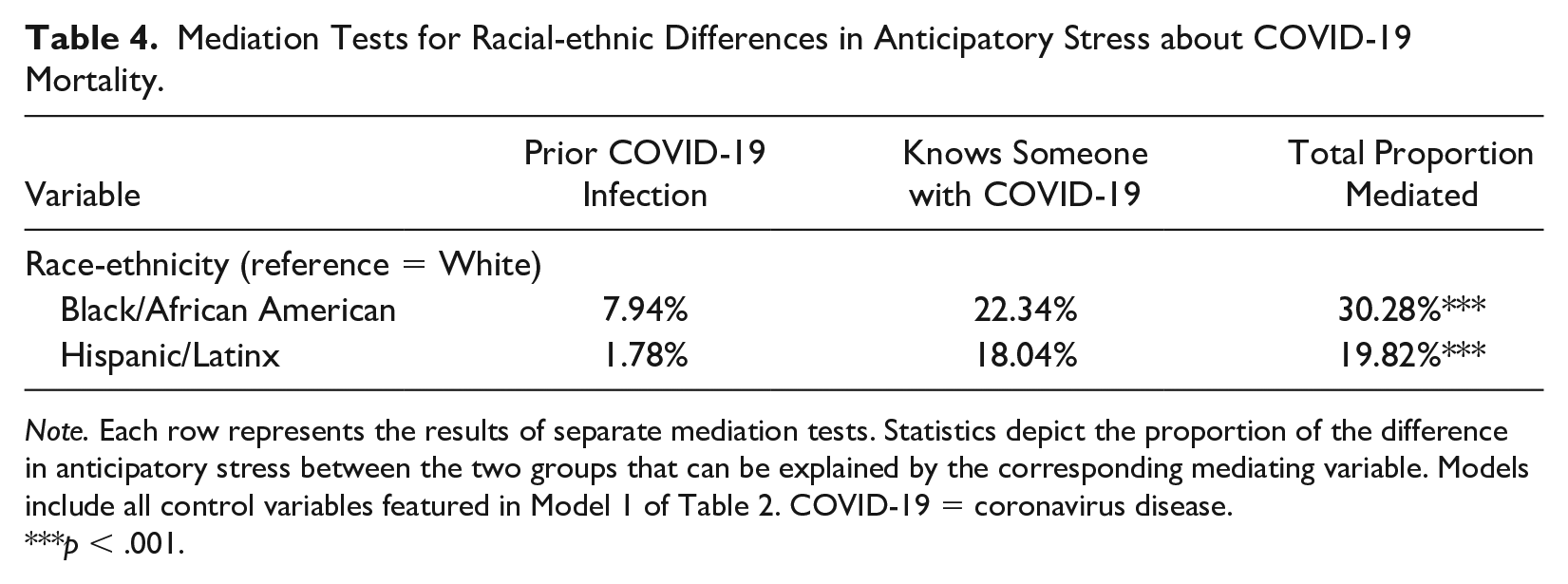
Note. Each row represents the results of separate mediation tests. Statistics depict the proportion of the difference in anticipatory stress between the two groups that can be explained by the corresponding mediating variable. Models include all control variables featured in Model 1 of Table 2. COVID-19 = coronavirus disease.
p < .001.
Turning first to the Black-White gap in worries about COVID-19 mortality, a greater prevalence of prior infection and elevated likelihood of having a family member or close friend test positive for the virus among Black respondents significantly mediate the difference between these groups (p < .001), explaining 7.9 percent and 22.3 percent, respectively, of the higher levels of anticipatory stress found among Black respondents. Moving to the discrepancy in worries about COVID-19 mortality between Latinx and White respondents, a similar pattern unfolds. A greater prevalence of prior infection among Latinx participants explains a more trivial 1.8 percent of the gap in anticipatory stress between these groups, compared to greater network exposure to the virus among Latinx respondents, which explains 18 percent of the gap in worries about COVID-19 mortality (p < .001). Jointly, the findings provide partial support for Hypothesis 8.
Discussion
Future-oriented worries, or anticipatory stressors, are more frequently experienced by marginalized racial-ethnic groups. Yet, it remains unclear what social mechanisms contribute to these disparities. Scholars posit that exposure to a stressor via one’s social network represents one potential mechanism underlying discrepancies in the experience of anticipatory stress (Pearlin and Bierman 2013). Using the case of the COVID-19 pandemic and data collected as part of a national survey, we expand on this hypothesis to examine how microlevel, mesolevel, and macrolevel contexts shape racial-ethnic variation in the concerns people have about COVID-related mortality. Our findings offer two principal contributions to understanding racial-ethnic differences in anticipatory stressors.
Foremost, our study contributes to a mounting evidentiary base that documents a clear social gradient in the experience of anticipatory stressors. Our findings echo those of other recent studies, which identify more frequent rumination on potential threats among members of marginalized racial-ethnic groups (Alang et al. 2021; DeAngelis 2020; Grace 2020). Against a backdrop of striking racial-ethnic disparities in COVID-19 hospitalizations and deaths, we found that Black and Latinx respondents reported greater concern than Whites that they, their romantic partner, or a child would die from the virus. These differences held even after extensive adjustment for a host of factors including demographic characteristics and socioeconomic standing. Our findings broadly cohere with recent evidence indicating that Black and Latinx Americans are more concerned about the pandemic (Lin and Liu 2022) and view COVID-19 as a greater threat to their personal health (Niño et al. 2021) than Whites. Such worries about the future represent yet another cognitive encumbrance that disproportionately affects the health of people of color in the United States.
Our second key finding sheds light on the social factors that spawn racial-ethnic disparities in anticipatory stressors. Black and Latinx respondents in our study were disadvantaged with respect to nearly every indicator of COVID-19 risk and exposure. These respondents were considerably more likely than Whites to have a history of prior COVID-19 infection, to have a family member or friend test positive for the virus, to be employed in jobs considered essential, to live in densely populated communities with higher infection rates, and to contend with higher rates of same-race COVID infections at the national level. However, because essential worker status, county-level factors, and national disparities in infection rates were not predictive of worries about COVID-19 mortality, we failed to find evidence these mechanisms meaningfully contribute to racial-ethnic differences in anticipatory stress. By contrast, our analyses indicate that higher rates of previous COVID infection among Black and Latinx respondents modestly contribute to racial-ethnic discrepancies in worries about COVID-19 mortality. More robust support was found for the contention that social networks are a critical explanatory factor behind the higher levels of anticipatory stress found among structurally disadvantaged groups. Pearlin and Bierman (2013:328) assert that members of marginalized social groups “are more likely to have more numerous and stronger social connections with individuals who are already struggling with” stressful circumstances. Consonant with national estimates (Funk and Tyson 2020), Black and Latinx respondents in our study were significantly more likely than White participants to have someone in their immediate family, a member of their extended family, or a close friend test positive for COVID-19. Approximately, one-fifth of Black-White and Latinx-White differences in worries about COVID-related mortality were explained by Black and Latinx respondents’ greater connectivity to significant others with the virus. Beyond joining with other recent work (Lin and Liu 2022) corroborating Pearlin and Bierman’s (2013) network exposure hypothesis, by adjudicating the relative contributions of different contextual factors to racial-ethnic differences in anticipatory stressors, our findings signal that events transpiring in a person’s network are more salient when it comes shaping their worries about the future than either individual health considerations, workplace and community factors, or macrolevel trends. These findings may have broader implications for understanding how other tumultuous, large-scale events including economic recession, climate change, and man-made disasters generate disparities in anticipatory stress that weigh on members of structurally marginalized groups.
It is worth considering why social networks matter more than individual health status when it comes to explaining racial-ethnic differences in COVID-related ruminative stress. We speculate that corporeal experience matters to a lesser degree than network connectivity insofar as prior infection connotes survival. While the long-term sequelae of the virus are worrisome for many, previous infection nevertheless suggests that a person has successfully combatted the virus, rendering it less menacing in the near term. By contrast, pervasive COVID infection circulating within one’s social network may induce a specter of uncertainty and foreboding sense of dread that an individual or their family could be struck by the virus at any moment. This dynamic would explain heightened vigilance and elevated worry about COVID-related mortality among Black and Latinx respondents. Broadly speaking, our findings imply that more proximal mesolevel factors—namely, vicarious exposure to hardships unfolding within kin and friendship networks—more substantially contribute to status differences in anticipatory stress than either individual risk-calculus, macrolevel trends, or more distal mesolevel features related to one’s workplace or community. As such, we argue that social networks merit greater empirical scrutiny in research focused on identifying the social foundations of status group variations in anticipatory stressors.
The null associations between worries about COVID-related mortality and other mesolevel and macrolevel factors also warrant discussion. Although it is not immediately apparent why neither community infection nor national trends in racial disparities were linked to anticipatory stress, these more distal factors may only matter insofar as people are actually aware of them. While our analyses incorporated racial disparities in infection at the national level, more fitting measures of macrocontext may have included items that inquired about respondents’ relative knowledge of these trends, or the extent to which they have consumed media in relation to them. In a study using data collected early in the pandemic, Kevin Stainback, Brittany Hearne, and Monica Trieu (2020) found the positive association between consumption of pandemic-related news stories and psychological distress was partially mediated by perceptions of COVID-19 threat. Given that media reports about racial-ethnic inequities in COVID-19 were first published by major news outlets in early April 2020 (Eligon et al. 2020; Mays and Newman 2020), it is plausible that a variable capturing media consumption might better explain the higher levels of concern about dying from COVID-19 found among Black and Latinx respondents.
A number of study limitations require comment. Foremost, the measurement of several key variables might be responsible for the patterning of results. To focus on respondents’ worries about their most intimate ties, anticipatory stress items were limited to a small subset of relationships including romantic partners and children. However, nearly 80 percent of COVID-19 deaths involve individuals 65 years of age or older (Centers for Disease Control and Prevention 2021). By not asking respondents to report their concerns about the potential death of a parent or grandparent due to COVID-19—social relations at elevated risk of premature mortality—we have likely underestimated respondents’ overall levels of anticipatory stress about the virus. This decision also overlooks the vital role that close friendships and fictive kin play in people’s lives. Relatedly, the network exposure variables rely on broad categorizations (i.e., immediate or extended family) rather than specific relationships (e.g., parent/sister or aunt/cousin). Aside from providing an incomplete portrait of people’s overall exposure to the virus, this measurement issue also precludes the ability to gauge how the total number of people infected in a person’s network might have differential effects on anticipatory stress.
In the absence of a survey item gauging the presence of children in the household, we included a measure of whether or not a respondent had homeschooled their child due to the pandemic in our analyses. While this measure is a useful proxy, it overlooks both children who are too young to attend school and adult children who live with their parents. As a result, the magnitude of the association between worries about COVID-19 and family composition in our study may be artificially reduced. Our measure of essential worker status similarly lacks granular detail that may help to explain why it was not associated with worries about COVID-related mortality net of study controls. Essential workers are a diverse group, encompassing occupations with highly divergent risks of COVID exposure (e.g., healthcare workers vs. postal workers) and varying ability to work remotely (e.g., teachers vs. grocery store clerks). By collapsing these individuals into a monolithic group absent such distinctions, we may be obscuring what is in fact a more robust association between frontline personnel and worries about COVID-19 mortality.
Other limitations relate to both generalizability and representation. Although we augmented our quota sampling approach with poststratification weights to approximate the demographic composition of the United States, these data should not be viewed as nationally representative. Notably, respondents in this study elected to take part because the topic was of some substantive interest to them. Given declining response rates found in studies that rely on random probability samples (Kohut et al. 2012), there is reason to suspect that people who purposively seek out participation in survey research are qualitatively different from the general population in ways that cannot be assessed here. We also neglect two groups that have been profoundly impacted by the virus: Indigenous people and Asian Americans. Indigenous people have at various points throughout the pandemic recorded the highest COVID-19 infection and death rates of any group (L. Hill and Artiga 2022), whereas Asian Americans have been subject to rampant xenophobia, hate crimes, and violence (Tessler, Choi, and Kao 2020). Unfortunately, due to the small segment of the American population comprised of each group, they correspondingly compose only a small portion of the sample. Because we were unable to form empirically grounded conclusions about these groups, they were ultimately removed from the analytic sample. Regrettably, this tactic is consistent with a recurring trend of omission due to undersampling when it comes to the representation of these racial groups in epidemiological reports (Holland and Palaniappan 2012). This systemic exclusion jeopardizes the health and wellbeing of members of marginalized groups. In view of our study’s shortcomings, we encourage future research to more thoughtfully oversample racial-ethnic groups underrepresented in the population.
The COVID-19 pandemic has generated loss and suffering on a scale unseen in the United States in over a century. The totality of this human suffering will leave psychological scars that endure well beyond widespread vaccination and economic recovery. Our findings demonstrate that worries about succumbing to the virus, or losing a child or partner to it, are more concentrated among Black and Latinx individuals. Furthermore, we find evidence that the reach of the virus in people’s social networks represents a key determinant of disparities in COVID-19 anticipatory stressors, with elevated worries about COVID-19 mortality among Black and Latinx people driven, in part, by their greater network exposure to the virus. As COVID-19’s collateral damage is evaluated in the coming years, it will be vital to consider the uneven stress burden introduced by the virus across different racial-ethnic groups. This accounting must also include the toll of chronic worry on mental health during the COVID era.
Supplemental Material
sj-docx-1-sre-10.1177_23326492231184837 – Supplemental material for Racial-ethnic Differences in Anticipatory Stress about COVID-19 Mortality: An Evaluation of Multiple Mechanisms
Supplemental material, sj-docx-1-sre-10.1177_23326492231184837 for Racial-ethnic Differences in Anticipatory Stress about COVID-19 Mortality: An Evaluation of Multiple Mechanisms by Matthew K. Grace and Ashley M. García in Sociology of Race and Ethnicity
Supplemental Material
sj-docx-2-sre-10.1177_23326492231184837 – Supplemental material for Racial-ethnic Differences in Anticipatory Stress about COVID-19 Mortality: An Evaluation of Multiple Mechanisms
Supplemental material, sj-docx-2-sre-10.1177_23326492231184837 for Racial-ethnic Differences in Anticipatory Stress about COVID-19 Mortality: An Evaluation of Multiple Mechanisms by Matthew K. Grace and Ashley M. García in Sociology of Race and Ethnicity
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for research, authorship, and/or publication of this article: The authors acknowledge support for this study from Hamilton College through an early career faculty grant.
Ethical Approval
This study was approved by the Institutional Review Board at Hamilton College: Protocol No. S20-105.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.