
Abstract
This study aimed to preliminarily investigate the associations between performance on the integrated Digit-in-Noise Test (iDIN) and performance on measures of general cognition and working memory (WM). The study recruited 81 older adult hearing aid users between 60 and 95 years of age with bilateral moderate to severe hearing loss. The Chinese version of the Montreal Cognitive Assessment Basic (MoCA-BC) was used to screen older adults for mild cognitive impairment. Speech reception thresholds (SRTs) were measured using 2- to 5-digit sequences of the Mandarin iDIN. The differences in SRT between five-digit and two-digit sequences (SRT5−2), and between five-digit and three-digit sequences (SRT5−3), were used as indicators of memory performance. The results were compared to those from the Digit Span Test and Corsi Blocks Tapping Test, which evaluate WM and attention capacity. SRT5−2 and SRT5−3 demonstrated significant correlations with the three cognitive function tests (rs ranging from −.705 to −.528). Furthermore, SRT5−2 and SRT5−3 were significantly higher in participants who failed the MoCA-BC screening compared to those who passed. The findings show associations between performance on the iDIN and performance on memory tests. However, further validation and exploration are needed to fully establish its effectiveness and efficacy.
Keywords
Introduction
The cooccurrence of hearing loss (HL) and cognitive decline is a common phenomenon in older adults, frequently observed in clinical practice (Shen et al., 2020). Significantly, HL is associated with accelerated cognitive decline in this demographic (Conceição Santos de Oliveira et al., 2023; Irace et al., 2022; Lau et al., 2022; Lin et al., 2013; Loughrey et al., 2018; Taljaard et al., 2016; Uchida et al., 2019). Importantly, both conditions adversely affect speech understanding.
In primary care settings, clinicians such as general practitioners, occupational therapists, and geriatricians without training in administering and interpreting relevant cognitive tests often face challenges in diagnosing cognitive decline in older adults (Bradford et al., 2009; Langa & Levine, 2014; Yang et al., 2015), especially when its interaction with HL is ambiguous (Dawes et al., 2023; Füllgrabe, 2020). In audiological clinical practice, assessing cognitive function in older adults exhibiting signs of potential cognitive decline may be appropriate (Shen et al., 2016). Specialists such as ear, nose, and throat doctors, audiologists, and other hearing care professionals frequently encounter older adults whose speech understanding difficulties surpass what their degree of HL would suggest. The causes of this have been attributed to declines in suprathreshold auditory processing (Humes et al., 2013; Pichora-Fuller et al., 2017; Vinay & Moore, 2007), and may also involve declines in cognitive processing during speech understanding (Pichora-Fuller et al., 2016; Pronk et al., 2013, 2019; Rönnberg et al., 2019). Without a clear understanding of the individuals’ cognitive status, challenges in speech understanding or hearing aid (HA) usage may be inadequately addressed (Shen et al., 2016). The traditional approach of evaluating cognitive and hearing functions in isolation prevents clinicians from discerning the interactive effects of both. In recent years, tests that can simultaneously measure speech understanding and cognitive function, primarily working memory (WM) function, have been developed. Examples include The Sentence-final Word Identification and Recall test (Lunner et al., 2016; Ng et al., 2013, 2015), the Word Auditory Recognition and Recall Measure test (Smith et al., 2016, 2020), and The Repeat-Recall Test (Kuk et al., 2020a, 2020b, 2023).
Furthermore, cognitive testing in individuals with HL can present unique challenges. HL can complicate test administration due to potential misunderstandings of instructions and difficulties in speech recognition, causing an overestimation of cognitive decline, and resulting in false positive findings (Dupuis et al., 2015; Füllgrabe, 2020; Jorgensen et al., 2016). While specialized versions of cognitive assessments, like the hearing or vision impairment versions of the Montreal Cognitive Assessment (MoCA; Dawes et al., 2019, 2023; Lin et al., 2017), have been developed to lessen the impact of hearing or vision impairments on test outcomes by using only visual or auditory test signals, these adaptations could not address the needs of individuals with concurrent hearing and vision impairments, as a specific version cannot simultaneously address the effects of both hearing and vision impairments on test results. To address these challenges, this study proposes and preliminarily evaluates the integrated Digit-in-Noise Test (iDIN) for memory performance evaluation. This innovative test was designed to measure and screen speech perception in noise, while simultaneously indicating memory performance.
iDIN Test
DIN test, employing a three-digit sequence (Smits et al., 2004, 2013) has long been utilized to measure speech reception threshold (SRT), defined as the signal-to-noise ratio (SNR) level that yields 50% recognition of the digit sequence. The effectiveness and application of the three-digit DIN for hearing screening have been demonstrated in multiple languages (Van den Borre et al., 2021). The SRT of DIN is believed to primarily indicate bottom-up speech perception in noise, due to its limited digit corpus that comprises 10 monosyllabic digits, and the lack of linguistic and contextual information (Smits et al., 2013). In individuals with HL, the SRT is significantly worse compared to the SRT of those with normal hearing. Consequently, with an appropriate cut-off, the DIN can effectively differentiate between individuals with normal hearing and those with HL. This versatility of the test is enhanced by its compatibility with various platforms, including telephones, laptops, tablets, and smartphones, facilitating widespread hearing screening (Akeroyd et al., 2015; Smits et al., 2013; Van den Borre et al., 2021).
The iDIN for Indicating Memory Performance
Building upon the three-digit DIN framework, we developed the iDIN, which utilizes sequences of two-, three-, four-, and five-digit sequences (Wang & Wong, 2023). Similar to the DIN, shorter digit sequences in the iDIN, such as two-digit and three-digit, predominantly measure speech perception in noise ability. Conversely, longer sequences such as the five-digit SRT in the iDIN are theorized to encapsulate a combined measure of speech perception in noise ability and memory performance. Our research indicated that the SRTs of the iDIN exhibited a slight increase as the length of the sequences increased, and the difference in SRTs between two-digit and five-digit sequences was 1.09 dB SNR for young adults and 1.69 dB SNR for older HA users. A significant correlation was observed exclusively between the five-digit SRT and WM capacity, as measured using auditory digit span test (DST) and reading span test in older HA users (Wang & Wong, 2023).
Cognitive functions, especially WM, play a vital role in speech understanding in noisy environments. The ease of language understanding (ELU) model delineates the role of WM in speech understanding (Rönnberg et al., 2013, 2019, 2021, 2022). According to the model, speech inputs are rapidly and automatically integrated as phonological representations (RAMBPHO) in an episodic buffer. Here, WM serves two functions: prediction and postdiction. The predictive role involves priming and pretuning the RAMBPHO buffer, alongside focusing attention. Postdiction, on the other hand, is activated when a phonological mismatch occurs, utilizing WM for inferential processes to identify the target speech. Thus, speech processing inherently involves an auditory-cognitive process, with cognitive load differing based on whether the listening conditions are favorable (implicit and fast processing) or nonfavorable (explicit and slow processing). In scenarios where digit inputs are clear and undistorted, such as listening in quiet conditions with normal hearing function, the RAMBPHO rapidly and implicitly matches lexical representations in the semantic long-term memory (LTM), facilitating effortless speech understanding. Conversely, in cases of distorted digit inputs, like in the presence of HL or noise masking, a mismatch arises between RAMBPHO and LTM representations. This necessitates the activation of top-down, explicit processing which is more effortful and demands greater WM involvement to resolve the mismatch and interpret suboptimal speech inputs. Consequently, individuals with lower WM are anticipated to face challenges in recognizing and recalling longer digit sequences. In addition to the ELU model, the framework for understanding effortful listening (FUEL) is another well-accepted model that also highlights varying cognitive resource demands under different speech recognition conditions with disparate difficulty levels (Pichora-Fuller et al., 2016). The FUEL offers a holistic perspective on the elements influencing the exertion of effort in listening activities. Central to the FUEL approach are concepts of cognitive load and available cognitive resources, which are crucial in cognitive theories related to attention. As a vital aspect of cognitive functioning in speech understanding, WM serves as a marker of a person's capacity for verbal WM capacity. Although it doesn’t directly assess effortful listening, it aids in elucidating the outcomes of individuals with lower WMC when faced with tasks that require a high degree of cognitive effort.
We propose utilizing the difference in WM load demand associated with shorter and longer digit sequences, when listening in noise, as an indicator of memory performance. In low WM load demand conditions, such as the two- and three-digit sequence conditions, SRT is primarily determined by the individual's hearing level. It is important to note that this does not imply the absence of WM resource involvement in digit recognition and recall in these scenarios. Rather, it suggests that the majority of individuals possess sufficient WM resources to meet the cognitive demands at this level. Thus, reduced memory performance may not significantly impact SRT in these conditions (Wang & Wong, 2023). Conversely, in greater WM resource demand conditions, exemplified by five-digit or longer sequences, individuals with some level of memory performance decline may find their available WM resources inadequate to meet the demands required for digit recognition and recall. In such instances, listeners require a better SNR to achieve successful digit recognition and recall. As WM resource demands increase across conditions, the influence of memory performance on SRT becomes more pronounced. Therefore, subtracting the SRT in a low WM resource demand condition (e.g., the two-digit SRT) from that in a high WM resource demand condition (e.g., the five-digit SRT) could potentially indicate WM function decline.
However, in Wang and Wong (2023), while a significant correlation was observed between the five-digit SRT and the WM test, the difference in SRTs between the five-digit and other digit sequences was not substantial. The potential reason for this could be that the variability in participants’ WM capacity was limited, with the majority exhibiting relatively normal levels of WM function. Alternatively, the recognition difficulty of the five-digit sequence conditions might not have been sufficiently challenging, and the amount of WM resources required for the five-digit sequence condition could have been well within the capabilities of most participants. Therefore, in this study, we aim to build upon the foundation laid by Wang and Wong (2023) by recruiting a larger number of older HA users with potential cognitive decline to explore the aforementioned hypotheses.
Aims of the Study
The aim of the current study is to preliminarily explore the following question: whether the difference in SRTs obtained using five-digit sequences (high WM resource demand conditions) and two- or three-digit sequences (low WM resource demand conditions), denoted as SRT5−2 and SRT5−3, is associated with performance on measures of WM in older HA users with a wide range of memory performances.
Method
Participants
Participants for this study were recruited from the Shengkang Hearing Center in Beijing, China. A total of 226 HA users who met the following inclusion criteria were invited via telephone calls to participate. They were (a) diagnosed with bilateral sensorineural HL, (b) native Mandarin speakers residing in Beijing, and (c) aged 60 years or older. HA users were recruited and their aided SRT were measured. To capture a broader range of cognitive and memory performances among participants, we purposefully also recruited participants who seemed to have a poor cognitive function, as noted in patient records of this hearing center. Ultimately, 81 native Mandarin-speaking older adult HA users consented to participate in the study. The cohort consisted of 62 males and 19 females, with ages ranging from 60 to 95 years (M = 72.51, SD = 7.57, Mdn = 72). The participants’ average years of formal education was 8.3 years (SD = 3.14, Mdn = 9), and the mean duration of HA use was 7.32 years (SD = 5.84, Mdn = 6). Figure 1 presents the mean pure-tone audiometric thresholds of participants.

Mean pure-tone audiometric thresholds with SDs as error bars for the better and worse ears among older adult hearing aid users.
Materials and Test Equipment
Speech Perception in Noise Tests
The Mandarin version of the iDIN was utilized to measure SRTs in noise, defined as the SNR levels at which 50% of the digit sequences are correctly recognized in noise. This was achieved using a one-up, one-down adaptive procedure, where the noise was fixed at 65 dB A and the speech stimuli were either reduced by 2 dB after a correct repetition or increased by 2 dB following an incorrect repetition. A digit sequence was considered correctly recognized only if all digits within the sequence were identified accurately. A long-term average speech-spectrum-shaped noise, generated based on the test material, was employed during the tests. Participants were instructed to repeat out loud the digit sequences they understood. The Mandarin iDIN was developed in accordance with the International Collegium of Rehabilitative Audiology recommendations for DIN development (Akeroyd et al., 2015). Besides the standard three-digit sequences, two-, four-, and five-digit sequences were also used. The average duration of the digits was 560 ± 72 ms (ranging from 427 to 665), and a 200 ms silent interval was inserted between each digit within a sequence. Noise was presented only during the presentation of each digit sequence, starting 500 ms before the digit sequence and ending 500 ms after. For each test session, a unique list of 24-digit sequences was randomly created from a fixed-digit sequence corpus comprising 120 sequences (90 in the two-digit sequence condition). SRTs measured on the Mandarin iDIN were found to correlate well (r = .90, p < .01) with speech perception in noise measured on the Mandarin Hearing In Noise Test and the Mandarin Chinese Matrix sentence test in older HA users (Wang & Wong, 2023).
Cognitive Function Tests
The Chinese version of the MoCA-Basic (MoCA-BC; Chen et al., 2016), which evaluates overall cognitive functions including attention and concentration, executive functions, memory, language, visuoconstructional skills, conceptual thinking, calculations, and orientation, was administered to group participants. Considering the generally lower education levels among older adults in Mainland China (Chen et al., 2016; Julayanont et al., 2015), the cut-off scores were education-adjusted: 19 for individuals with less than 6 years of education, 22 for those with 7–12 years, and 24 for individuals with more than 12 years of education (Chen et al., 2016). Since the iDIN is hypothesized to be associated with performance on measures of memory, the score of the delayed memory item in the MoCA was also extracted for additional analysis.
The DST and the Corsi Block-Tapping Task (CBTT) were employed to evaluate WM capacity and attention. The DST is a widely used measure of short-term memory, attention, executive function, and WM capacity. It assesses the individual's ability to recognize and recall the longest sequence of digits in both forward and backward orders under quiet conditions (Hale et al., 2002; Rosenthal et al., 2006). The CBTT was used to measure visuospatial WM capacity (Kessels et al., 2008; Smyth & Scholey, 1994).
For this study, the forward and backward DSTs were sourced from the Chinese version of the Wechsler Adult Intelligence Scale (Gong, 1992). Participants were required to listen to and repeat a series of digit sequences delivered by a female speaker, in both forward and backward orders. Sequence lengths varied from 3 to 12 digits for the forward task and 2–10 digits for the backward task. Testing ceased when a participant failed to accurately repeat a sequence of the same length twice. Scores were calculated by totaling the longest number of correctly repeated digits for both tasks. Before administering the DST, digits were played to the participants, and the presentation level was adjusted based on each participant's feedback regarding listening comfort and clarity, achieving a listening intensity that satisfied the participants.
The CBTT, akin to the DST, is a commonly used tool in clinical and research settings for assessing visuospatial WM capacity (Kessels et al., 2000). The version employed in this study was developed by the PsyToolkit (Stoet, 2010, 2017). During the test, participants would see nine purple squares scattered across the screen, with a certain number of squares changing from purple to yellow in a specific order. Upon the cue “go,” they were asked to select the blocks in either forward or backward order using a mouse. For those who felt uncomfortable manipulating a mouse, a touch screen option was available for indicating the target blocks. Since the CBTT does not incorporate response time in its scoring, the use of either method does not affect the test results. The test started with two squares changing color, with up to nine squares changing color. The forward test was conducted first, followed by the backward test. The test continued with an increasing number of blocks until the participant failed to reproduce the sequence accurately twice in both orders. Scoring was based on the sum of the highest number of blocks successfully recalled in both forward and backward orders.
Test Equipment
All measurements were conducted in a sound-treated booth under aided conditions. The CBTT was administered using an external AOC 27-inch, 4 K, 60 Hz refresh rate monitor connected to a laptop. Sound stimuli were delivered through JBL Control 25-1 loudspeakers, which were connected to a TASCAM US-2 × 2 soundcard attached to a laptop.
Procedures
An otoscopy was performed to rule out the presence of any debris or outer ear disorders that could potentially impact the test results. This was followed by pure-tone audiometry to assess the hearing levels of participants. The hearing devices were fit according to the manufacturer prescriptive methods and adjusted according to patient preferences. After pure-tone audiometry, audiologists at the hearing center met each participant to inquire about their HAs and use conditions, and performed some fine-tuning of the HAs, if requested by the participants. For participants requiring acclimatization after HA fine-tuning, 30 min to 1 h was allotted for short-term acclimatization. Participants were given the option to walk on the streets and/or chat with staff or family at the hearing center. Once the HAs were confirmed to the satisfaction of the participants, they proceeded to the next phase of testing with the researchers. All participants were instructed to wear their HAs during the subsequent tests. The sequence of tests began with the MoCA-BC, followed by the DST and CBTT, conducted consecutively. Prior to the formal DST, the Mandarin digits one to nine were played back to familiarize them with the digit stimuli used in the DST. Participants were asked to provide feedback on whether the tester needed to change the volume setting to achieve optimal digit recognition and a comfortable listening level. The researcher adjusted the volume using the laptop volume control based on the participants’ feedback. No vision and dexterity assessments were conducted before the CBTT. All participants reported no vision problems with glasses on. Before the formal test, participants were allowed to adjust the distance of the display screen to optimize readability. No participants reported having to strain to see or had problems completing the test due to visual acuity. Following these tests, the iDIN was conducted in a sound field environment. To familiarize the participants with the test stimuli and procedures, 15 sequences of each of the four-digit sequences (two-, three-, four-, and five-digits) in noise were administered adaptively as practice. The iDIN tests were carried out sequentially, starting from the two-digit and progressing to the five-digit sequences. During both practice and formal testing sessions, participants were asked to repeat the digits they understood as accurately as possible. The researcher determined the correctness based on the participants’ responses; a sequence was only considered correct if all digits within it were repeated accurately. There was no time limit imposed on participants for their responses. The noise level was fixed at 65 dBA, and test stimuli were presented from a loudspeaker located 1 m away from the center of the participant's head, at 0° azimuth. Participants were allowed breaks upon request or when they showed signs of fatigue. Ethical approval for all procedures was granted by the Faculty Research Ethics Committee at the University of Hong Kong.
Results
Cognitive Function Test Results
Out of the 81 participants, 21 failed the MoCA-BC screening. All participants successfully completed the DST and the CBTT. The mean scores for the MoCA-BC, delayed memory item score of MoCA-BC, DST, and CBTT among the older participants were 22.14 ± 3.37, 2.26 ± 1.09, 10.04 ± 1.77, and 7.25 ± 1.61, respectively. After Shapiro–Wilk normality tests to assess the distribution of data, subsequent correlation analyses were performed using Pearson's correlation for data that were normally distributed and Spearman's rank-order correlation for data nonnormally distributed. Spearman's rank-order correlation analyses revealed significant correlations between MoCA-BC and DST (rs = .692, p < .001), MoCA-BC and CBTT (rs = .580, p < .001), and DST and CBTT (rs = .667, p < .001). With a p-value set at .005 due to multiple comparisons, scores from all three cognitive function tests showed significant and negative correlations with age (rs = −.382 to −.257, p < .02), and significant and positive correlations with years of education (rs = .387 to .537, p < .001; see Table 1).
Coefficients (Spearman's r) of Correlations Between Cognitive Measures and Age, Education Level (N = 81).
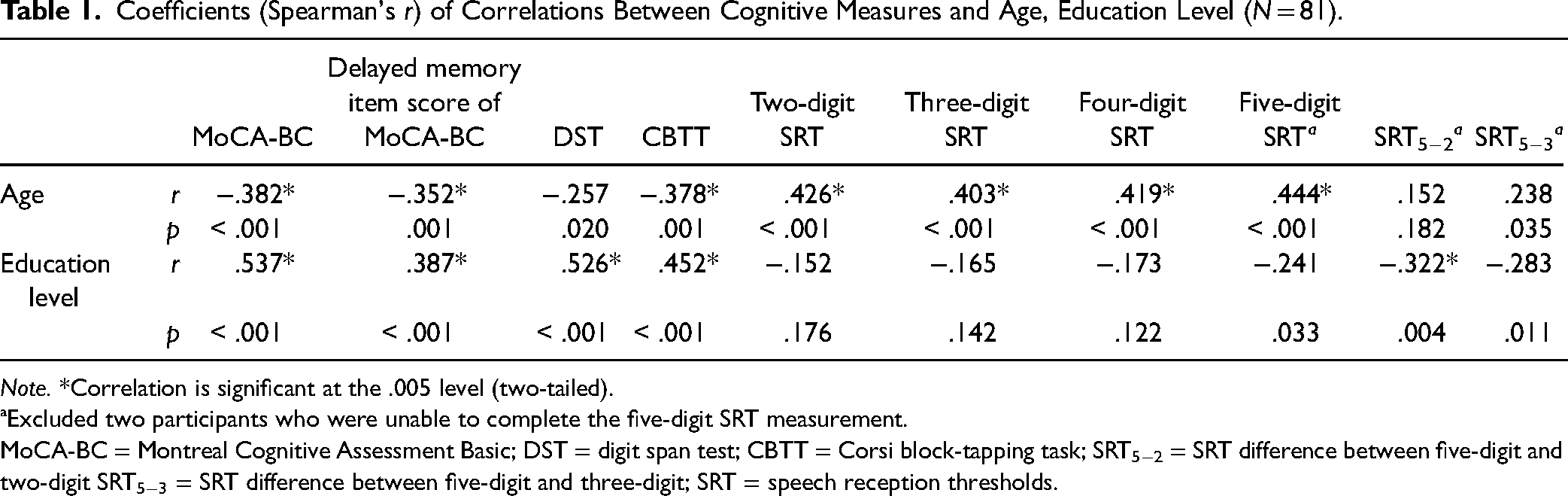
Note. *Correlation is significant at the .005 level (two-tailed).
ªExcluded two participants who were unable to complete the five-digit SRT measurement.
MoCA-BC = Montreal Cognitive Assessment Basic; DST = digit span test; CBTT = Corsi block-tapping task; SRT5−2 = SRT difference between five-digit and two-digit SRT5−3 = SRT difference between five-digit and three-digit; SRT = speech reception thresholds.
Digit Perception in Noise Test Results
All participants successfully completed the two-, three-, and four-digit iDIN. However, two participants could not complete the test, meaning that they were unable to successfully repeat five digits at any SNR. Among the 79 older participants who completed all iDIN, the SRTs for the two-, three-, four-, and five-digit iDIN tests were −1.30 ± 3.47, −0.97 ± 3.45, −0.67 ± 3.48, and 0.94 ± 4.30 dB SNR, respectively. The differences in SRTs between short (i.e., two- and three-digits) and long-digit sequences (i.e., five-digit) were calculated. Mean SRT5−2 and SRT5−3 were 2.23 ± 1.90 and 1.91 ± 1.81, respectively. A Wilcoxon Signed-Ranks Test indicated significant differences between SRT5−2 and SRT5−3, Z = −4.304, p < .001. The SRTs measured with iDIN digit sequences showed significant correlations with age, with correlation coefficients ranging from rs = .403 to .444 (p < .001); and with hearing level, with coefficients ranging from rs = .430 to .449 (p < .001). No correlation was observed between the SRTs of iDIN and years of education when the p-value was set at .005 due to multiple comparisons. Correlation analysis revealed a significant association between five-digit SRTs and years of education without considering multiple comparisons (rs = −.241, p = .033). However, when accounting for the potential influences of memory and cognitive functions (controlling for DST, CBTT, and MoCA-BC scores separately) through partial correlation analysis, this correlation ceased to be significant (ps > .05).
Relationship Between iDIN Results and Memory Test Results
Significant Spearman's rank-order correlation was noted between the SRTs obtained using all digit sequences and the scores on the three cognitive function tests. Notably, the SRTs measured in the five-digit iDIN displayed the highest correlation coefficients among the digit sequences (see Table 2). When the potential influences of age, years of education and hearing level were accounted for in partial correlation analysis, their correlations with two- to four-digit SRTs, were no longer significant; while the correlation with five-digit SRT remained significant.
Correlation Coefficients (Spearman's r) Between Results on the iDIN Tests and Cognitive Function Tests (MoCA-BC, DST, and CBTT) Among Participants Who Completed All iDIN Test Conditions, n = 79.

*Correlation is significant at the .005 level (two-tailed).
MoCA-BC = Montreal Cognitive Assessment Basic; DST = digit span test; CBTT = Corsi block-tapping task.
As suggested in Table 3, Spearman's rank–order correlation analyses revealed that both SRT5−2 and SRT5−3 were significantly correlated with results on the MoCA-BC (rs = −.632 to −.603, p < .001), delayed memory item score of MoCA-BC (rs = −.455 to −.442, p < .001), DST scores (rs = −.705 to −.654, p < .001) and CBTT scores (rs = −.529 to −.528, p < .001).
Spearman's r Correlations Coefficients Relating SRT5−2 and SRT5−3 to Results on Standardized Cognitive Function Tests, n = 79.

*Correlation is significant at the .005 level (two-tailed) speech reception thresholds
MoCA-BC = Montreal Cognitive Assessment Basic; DST = digit span test; CBTT = Corsi block-tapping task; SRT5−2 = SRT difference between five-digit and two-digit SRT5−3 = SRT difference between five-digit and three-digit; SRT = speech reception thresholds.
When accounting for the potential influences of age, years of education, and hearing level in partial correlation analysis, the correlation coefficients for the comparisons above slightly decreased and remained significant (see Table 3). Table 1 also shows that SRT5−2 correlated significantly with participants’ education level (rs = −.322, p = .004).
iDIN Results and MoCA-BC Pass/Fail Results of Participants
Among the 79 participants who completed all iDIN SRT measurements, 60 passed and 19 failed MoCA-BC MCI screening. Their demographic characteristics, including age, better ear pure tone average at 0.5, 1, 2, and 4 kHz (BE4PTA), years of education, and iDIN SRTs, are detailed in Table 4. A two-way ANOVA was performed to evaluate the effects of the number of digits in sequences and participants who passed or failed the MoCA-BC on iDIN SRTs. The results revealed a significant main effect for the number of digits in sequences, F(3, 308) = 8.232, p < .001, partial η2 = .074; significant main effect for participants who passed or failed the MoCA-BC, F(1, 308) = 5.361, p = .021, partial η2 = .017; and no significant interaction between the number of digits in sequences and whether participants passed or failed the MoCA-BC, F(3, 308) = 2.465, p = .062, partial η2 = .023. Post hoc testing using Tukey's HSD indicated that only the five-digit SRT significantly differed from the other digit sequence SRTs (ps ≤ .030). Figure 2 compares their pure-tone audiometric thresholds. Independent samples t-tests revealed that participants who failed the MoCA were significantly older than those who passed, t(77) = −2.180, p = .032); although participants who failed the MoCA exhibited slightly higher levels of HL at high frequencies (2–8 kHz), the difference in BE4PTA was not statistically significant, t(77) = −.699, p = .487. Furthermore, a Mann–Whitney U test showed that participants who failed the MoCA had significantly fewer years of education compared to those who passed, Z = −2.980, p = .003.

Mean pure-tone audiometric thresholds with SDs as error bars, participants were grouped based on whether they passed the MoCA-BC.
Age, Better Ear Four-Frequency Pure-Tone Average Hearing (BE4PTA), Two-Digit SRT, Five-Digit SRT, SRT5−2, and SRT5−3 Based on Whether Participants Passed the MoCA-BC.

ªExcluded two participants who were unable to complete the five-digit SRT measurement and failed the MoCA-BC.
MoCA-BC = Montreal Cognitive Assessment Basic; SRT5−2 = SRT difference between five-digit and two-digit SRT5−3 = SRT difference between five-digit and three-digit; SRT = speech reception thresholds; SNR = signal-to-noise ratio.
*p < .05 (two-tailed); **p < .01 (two-tailed).
Figure 3a compares digit SRTs between the two groups of participants. An independent-sample t-test indicated statistically significant differences in five-digit SRT, t (77) = −3.135, p = .002. Figure 3b displays SRT5−2 and SRT5−3 results from older HA users, compared to young adults with normal hearing, from Wang and Wong (2023). A one-way ANOVA revealed significant differences in SRT5−2, F(2, 110) = 52.474, p < .001, η2 = 0.488 and SRT5−3, F(2, 110) = 49.017, p < .001, η2 = 0.471 among the three groups. Tukey post hoc analysis identified significant differences in SRT5−2 and SRT5−3 between older participants who failed the MoCA-BC and the two other groups exhibiting normal cognitive function, regardless of age (p < .001). No significant differences were found in SRT5−2 and SRT5−3 between the other two groups with normal cognitive function (p > .05).

Comparison of SRTs in four-digit sequences (a) and SRT5−2 and SRT5−3 (b) in young listeners with normal hearing (data from Wang & Wong, 2023) and older participants who passed or failed the MoCA-BC. Standard deviations are represented by error bars.
As a preliminary analysis of how well DST, SRT5−2, and SRT5−3, compare to results from the MoCA-BC in the classifications of individuals with potential MCI, receiver operating characteristic (ROC) curves were utilized to assess the discriminatory capacity of these measures. The area under the roc curve (AUC) was calculated for each measure to compare diagnostic performance. The optimal cut-off scores for identifying individuals with potential MCI were determined using the Youden index (J) method. The DST, SRT5−2, and SRT5−3 showed high AUCs of 0.866, 0.934, and 0.931, respectively (refer to Figure 4), indicating their potential utility in screening for cognitive function in HA users with potential MCI. The optimal cut-off scores for DST, SRT5−2, and SRT5−3 were established as 8.5 (sensitivity: 0.867; specificity: 0.714), 3.15 (sensitivity: 0.905; specificity: 0.933), and 2.95 (sensitivity: 0.81; specificity: 0.905), respectively.

Receiver operating characteristic curve analysis of SRT5−2, SRT5−3, and the DST for MCI screening. Note. DST = digit span test; SRT5−2: SRT difference between five-digit and two-digit SRT5−3: SRT difference between five-digit and three-digit; MCI = mild cognitive impairment; SRT = speech reception thresholds.
Discussion
This study introduces the iDIN not only as a widely accepted hearing screener but also as a potential indicator of memory performance in older adults. The following will discuss our exploration into the use of the iDIN, specifically SRT5−2 and SRT5−3, in indicating memory performance.
Cognitive Function and Its Relationship With Age and Education Level
Our study revealed that the performance on the three cognitive function tests was negatively correlated with age and positively associated with education level. These findings are consistent with previous literature, confirming that cognitive function tends to decline with advancing age, a relationship that is well-established and expected (Archer et al., 2018; McNab et al., 2015; Pliatsikas et al., 2019; Zuber et al., 2019). On the other hand, individuals with higher educational attainment often demonstrate better cognitive function, suggesting education seems to serve as a form of cognitive reserve and education level should be accounted for when interpreting results from cognitive function tests (Archer et al., 2018).
Additionally, individuals with higher levels of educational attainment typically occupy higher-status professions and enjoy a higher socioeconomic status, better access to personal health care, more proactive health behaviors, and fewer comorbid conditions (e.g., diabetes), all of which potentially relate to slower progression of cognitive decline (Kujawski et al., 2018). Although not a focus of the study, education seems to have a more pronounced impact on auditory WM as compared to visuospatial WM in older adults as education exhibited a stronger correlation with the DST compared with the CBTT. This could potentially be attributed to the effects of education on the enhancement of the phonological auditory processing loop within WM (Conant et al., 2003). However, given the modest differences in correlation coefficients and the lack of statistical evidence to confirm significant differences between these correlation strengths, this conclusion remains speculative and requires further exploration in future research. Years of education in adults have been correlated with cognitive functioning and identified as a significant, potentially modifiable risk factor for dementia in early life (Livingston et al., 2020). As such, education has a profound influence not only on cognitive capabilities but also on mitigating the progression of age-related cognitive decline (Lövdén et al., 2020). In our study, a significant correlation was found between education and all cognitive memory test scores.
Digits Perception in Noise and Relationships With Education Level
Our findings, after accounting for multiple comparisons, show that none of the digit sequences (two- to five-digit) in the iDIN significantly correlate with education level. This suggests that the recognition of digit sequences in noise may not be influenced by the level of education attained. Nonetheless, the correlation between five-digit SRT and years of education was the strongest, showing statistical significance without considering multiple comparisons (p = .033). However, considering the simplicity of the test stimuli (i.e., the first 10 digits) and the lack of a relationship between education level and SRTs measured using other digit sequences, we surmise that five-digit SRTs might not be directly influenced by education level, but modulated by factors such as WM capacity or general cognitive function, both also correlated significantly with education. When controlling for DST, CBTT, or MoCA scores, the five-digit SRT no longer shows a significant correlation with education (p < .05). This implies that the cognitive demands of recalling longer digit sequences in noise, as required in the five-digit SRT condition, may also reflect the cognitive capabilities of an individual, which is modulated by educational level. Future studies could further explore this result in young adults without cognitive decline.
The iDIN for Indicating Memory Performance
A pivotal aspect of this study was exploring the hypothesis that SRT5−2 and SRT5−3 can be used to indicate memory performance, after accounting for the effects of hearing in speech understanding. We first demonstrated that five-digit SRTs, but not two- and three-digit SRTs, correlated with cognitive function after controlling for the effects of age and hearing level, thus providing evidence that five-digit SRT is indicative of cognitive function but two- and three-digit SRTs are not. SRT5−2 and SRT5−3 were derived using two-digit and three-digit SRTs as baselines to account for the effects of hearing so that the relationship with memory performance in recognizing five digits can be revealed. Significant correlations were observed between SRT5−2, SRT5−3, and the score of the delayed memory item in the MoCA, two memory tests, indicating that SRT5−2 and SRT5−3 may serve as indicators of memory performance. The correlation coefficients of SRT5−2, SRT5−3, and the score of the delayed memory item in the MoCA were the lowest compared to the other two WM tests. This may suggest that SRT5−2 and SRT5−3 reflect aspects of short-term or WM more than delayed memory. As anticipated, digit SRT correlated more strongly with scores on the DST compared to those on the CBTT. The DST, with its similar structure to the iDIN, evaluates auditory WM and attention capacity and thus relates more closely to speech perception in noise than the visuospatial WM measured by the CBTT (Ng & Rönnberg, 2020).
If being used as an indicator of memory performance, SRT5−2 and SRT5−3 must perform as well as other cognitive function tests. Good relationships with cognitive function measures would also be essential and the current study revealed correlations with auditory-based cognitive function tests (i.e., the MoCA and DST) in the range of −.705 to −.603, suggesting they are measuring domains that are similar but not essentially the same. SRT5−2 and SRT5−3 measurements are also free from the effects of age, as statistically significant differences were not observed between young adults and older adults.
On the other hand, our data demonstrated that performance on the WM test correlated with short-digit sequence SRTs (such as two-digit or three-digit sequences) but the correlation with longer digit sequence SRTs (such as five-digit) is stronger. In other words, WM plays a greater role in recognizing longer digit sequences. While shorter digit sequences such as three digits that are used in the current study (or the conventional DIN), are much less affected by cognitive function, making them ideal for screening bottom-up speech perception or peripheral auditory function. In summary, our data show that comparing the impact of memory performance in high versus low cognitive demand conditions as a means of indicating memory performance is promising. However, whether the response mode (i.e., verbal response used in the current study vs. tapping a number pad on a tablet) would affect test results needs to be evaluated. In this study, participants were asked to verbally repeat digits, instead of entering digits on a keyboard or tablet. This method may, to some extent, reduce the impact of cognitive function or dexterity on test results. Furthermore, in real clinical hearing screenings using DIN, self-testing modes are typically employed.
The Potential of iDIN for Rapid Cognitive Screening
In this study, we conducted a preliminary exploration of using SRT5−2 and SRT5−3 as indicators for distinguishing whether participants passed the MoCA-BC. While recognizing that the MoCA-BC, being a screening test itself, cannot serve as a definitive benchmark to validate another test, we hope that our findings can inform future, more rigorous studies.
In clinical settings, the Mini-Mental State Examination (Arevalo-Rodriguez et al., 2015) and the MoCA (Nasreddine et al., 2005) are widely used for cognitive screening. However, these tools often require specialized training (Nasreddine et al., 2005) and considerable time to administer (e.g., approximately 15 min for the MoCA), making adoption in clinical routines challenging. The test could take longer for individuals with cognitive, sensory, or perceptual impairments, such as hearing or visual loss. When good vision, hand–eye coordination, and auditory comprehension are needed, impairment of these functions could skew test results, overestimating cognitive decline (Dawes et al., 2019, 2023; Dupuis et al., 2015; Füllgrabe, 2020; Reischies & Geiselmann, 1997; Wittich et al., 2010). Adaptations of tests to account for a specific impairment, such as hearing or vision impairment versions of the MoCA (Dawes et al., 2019, 2023), do not address concurrent impairments, nor separate the effects of either. Another issue is the effects of education level on test results, which has been demonstrated in the current and previous studies (Archer et al., 2018; Pliatsikas et al., 2019). For example, in the MoCA, there is a task where participants are asked to replicate a cube by drawing one. For those who have never studied solid geometry, the difficulty of this task increases significantly. At that point, for these individuals, knowledge becomes a major factor affecting scores, rather than purely cognitive function. Low education level is common among older adults, particularly in low- and middle-income countries (Ryan & Bauman, 2016), such as Mainland China where nearly half of the over-60 population has only attained elementary education (Luo et al., 2015).
The iDIN could offer many advantages for rapid cognitive screening. Firstly, it is time-efficient; completing two-digit and five-digit SRT measurements takes only about 5 min in total. This duration could be further reduced for screening purposes by decreasing the number of sequences in the test. Secondly, the test is straightforward for both administrators and participants, requiring no complex training for easy operation and interpretation. Thirdly, in comparison to other cognitive tests, the recognition and recall of digit sequences are likely minimally influenced by the level of education, as illustrated here, making it one of the least educationally biased forms of testing. Fourthly, sensory losses, including hearing and vision loss, are unlikely to significantly affect the iDIN outcomes. Because the test is auditory-based, visual acuity is not a concern and in addition, by comparing five- and two-digit SRTs, we are able to account for the effects of hearing and reveal the additional effects of memory decline on speech understanding. Finally, iDIN also retains its fundamental function as a hearing screening tool, meaning that within approximately 5 min, it can concurrently screen for both hearing and cognitive functions.
However, to use the iDIN for indicating cognitive function, several issues must be addressed. Firstly, the research we have conducted so far has been limited to the evaluation of its relationship with memory performance. In contrast, the MoCA was designed and validated to cover a broader range of cognitive function domains. Further research is thus needed to learn how the outcomes from the iDIN relate to other domains of cognitive functions and their respective measures. Validity of the iDIN in indicating cognitive function should also include evaluation of patients already diagnosed by neuropsychologists. Secondly, theoretically, SRT5−2 and SRT5−3 do not completely negate the influence of an HL on test results. Cognitive resources during digit recognition and recall are mainly expended in two areas: recognizing digits and processing digit information. The cognitive resource consumption of the former is impacted by HL. When using SRT5−2 as an indicator of cognitive/memory performance, the cognitive resources expended due to HL could differ in recognizing five-digit and two-digit sequences. Hence, HL can still influence the cognitive/memory performance indicated by SRT5−2. In our study, we recruited a sample of older HA users whose hearing sensitivity was compensated by HAs, thus minimizing this impact. However, if future tests target older individuals with untreated HL that is more severe, the influence of HL on test results may become apparent. To effectively offset the cognitive resources consumed due to HL when digit sequences of different lengths are used, a theoretically sound solution would be to compare the SRTs obtained using the same digit sequence length (e.g., three-digits) with forward and backward recall. Recalling digit sequences in backward order could theoretically measure WM more effectively (Hilbert et al., 2015).
Conclusions
This study embarked on an exploration of utilizing the iDIN to indicate memory performance in older HA users. SRT5−2 and SRT5−3 were found to be significantly correlated with WM capacity tests and MoCA-BC scores; and are efficient in differentiating older adults who failed the MoCA-BC, with little effects from age and education level. Notably, these results suggest the iDIN sets could potentially be a rapid, simple, and reliable measure of screen memory. The test can be easily self-administered using portable electronic devices such as tablets or smartphones, increasing versatility and accessibility. While this investigation represents only the initial step in exploring the iDIN's potential applications for indicating memory and cognitive function, these promising findings underscore the significant potential the iDIN holds for real-world clinical applications. Our future research endeavors will focus on broadening and validating the application of the iDIN.
Footnotes
Acknowledgments
We would like to thank all the older adults who participated in the study and the audiologists at the Beijing Shengkang Hearing Center who assisted in recruiting participants. We also wish to thank Prof. Bradley McPherson for his feedback on early versions of this manuscript and Prof. John Culling and the two anonymous reviewers for their valuable suggestions on this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.