
Abstract
The cortical auditory evoked potential (CAEP) is a change in neural activity in response to sound, and is of interest for audiological assessment of infants, especially those who use hearing aids. Within this population, CAEP waveforms are known to vary substantially across individuals, which makes detecting the CAEP through visual inspection a challenging task. It also means that some of the best automated CAEP detection methods used in adults are probably not suitable for this population. This study therefore evaluates and optimizes the performance of new and existing methods for aided (i.e., the stimuli are presented through subjects’ hearing aid(s)) CAEP detection in infants with hearing loss. Methods include the conventional Hotellings T2 test, various modified q-sample statistics, and two novel variants of T2 statistics, which were designed to exploit the correlation structure underlying the data. Various additional methods from the literature were also evaluated, including the previously best-performing methods for adult CAEP detection. Data for the assessment consisted of aided CAEPs recorded from 59 infant hearing aid users with mild to profound bilateral hearing loss, and simulated signals. The highest test sensitivities were observed for the modified T2 statistics, followed by the modified q-sample statistics, and lastly by the conventional Hotelling's T2 test, which showed low detection rates for ensemble sizes <80 epochs. The high test sensitivities at small ensemble sizes observed for the modified T2 and q-sample statistics are especially relevant for infant testing, as the time available for data collection tends to be limited in this population.
Introduction
Approximately 1 in 1000 infants are born each year with permanent bilateral hearing loss (Davis et al., 1997; Fortnum et al., 1997). When left untreated, hearing loss has been associated with a cascade of long-lasting detrimental effects (Hogan et al., 2014; Idstad et al., 2019; Moeller 2007; Ramkalawan & Davis, 1992; Stevenson et al., 2015; Theunissen et al., 2014; Yoshinaga-Itano et al. 1998). It is therefore important that hearing loss is diagnosed and treated (e.g., by fitting a hearing aid) at a young age, ideally within the first 3 months of life (Ching et al., 2013; Yoshinaga-Itano et al., 1998). However, this poses some challenges, as behavioral hearing tests cannot be reliably performed until a developmental age of 7–9 months (Widen, 1993). Early audiological intervention procedures have therefore been built around objective measures of hearing that do not require voluntary responses, such as auditory evoked potentials (AEPs).
AEPs are defined as changes in brain activity in response to acoustic stimuli (Picton, 2011). They are typically recorded non-invasively using the electroencephalogram (EEG), and comprise a series of peak and trough voltage amplitudes falling within the first ∼1 s interval following stimulus onset. The AEP can also be sub-categorized into various components based on the underlying neural generators along the auditory pathway. These components can be identified by the latencies (time following stimulus onset) of various peaks and troughs; thus the cochlear microphonic, the auditory brainstem response (ABR), the mid-latency response, and the cortical auditory evoked potential (CAEP) have been defined (e.g., Picton 2011), in order of their peak and trough latencies.
For evaluating hearing function in infants, the most commonly used AEPs are the ABR and the CAEP (Lightfoot et al., 2016; Lightfoot et al., 2019). A potential advantage for the ABR over the CAEP is that it can be reliably recorded during sleep (e.g., Jewett & Williston, 1971) and is unaffected by attention (Picton & Hillyard, 1974). The drawback is that it cannot be reliably recorded in some patients, such as those with auditory neuropathy spectrum disorder (Roush et al., 2011). Furthermore, when testing patients with their hearing aids on, results may not reflect patients’ hearing, as the hearing aids do not respond well to the rapid presentation rate of ABRs which confuse noise reduction algorithms. It might also be argued that the ABR provides a limited assessment of the integrity of the auditory pathway, as it represents neural activity generated by just the early components of the pathway. This contrasts with the CAEP which represents neural activity generated by thalmo-cortical brain regions.
Early audiological assessment using CAEPs is a challenging procedure, both in terms of evoking the CAEP, and in accurately detecting it within clinically acceptable test times. In terms of signal-to-noise ratios (SNRs), the CAEP has typical peak amplitudes in the 5–10 µV range (e.g., Munro et al., 2020; Picton 2011), whereas the background activity tends to be in the ∼50 µV range after pre-processing and artefact rejection. It is therefore common practice to record an ensemble of CAEPs following repeated stimuli, and to average the recorded waveforms to reduce “noise.” Clinicians are then given the task to visually inspect the waveforms, and to determine whether a CAEP is absent or present. This is especially challenging for hearing-impaired infants, as waveforms can vary substantially across individuals due to different degrees of hearing-impairment (Oates et al., 2002) and/or lack of maturation of the auditory system (Ponton & Eggermont, 2007). As such, it is not always clear to the examiners what to look for in the displayed waveforms. Various objective methods have therefore been proposed to assist the clinicians with this task, and improve the accuracy and efficiency of the test. However, the challenges for visual CAEP inspection arising from the variability in infant responses also impact objective detection methods: infant responses can be considerably different from adult responses, and template matching methods that performed best in adults (Chesnaye et al., 2021a) are unlikely to work well in this young population.
Perhaps the most commonly used objective method for CAEP detection is the Hotelling's T2 (HT2) test, applied in the time domain (Golding et al., 2009). The HT2 test was previously shown to have a test sensitivity similar to experienced clinicians when detecting CAEPs in infants (Carter et al., 2010), and has some desirable properties in terms of statistical power (Anderson, 2003). A drawback for the HT2 test, however, is that it is known to suffer from low test sensitivities at relatively small sample sizes. The latter is also known as the “large p small n” problem (Li et al., 2017) or the “effect of high dimension,” and has been hypothesized to be due to poor estimates of the feature covariance matrix (Bai & Saranadasa, 1996), which is a key component in calculating the T2 statistic. The low test sensitivity for the HT2 test was previously also observed for CAEP detection in adults with normal hearing where it was outperformed by various alternative detection methods for ensemble sizes of ∼40 epochs or less (Chesnaye et al., 2021a). Note that high test sensitivities for small ensemble sizes are of particular interest for infant CAEP detection as the time windows for high quality data collection tend to be limited.
The present study aims to overcome the low test sensitivity of the HT2 test by exploiting the correlation structure underlying the data to allow improved feature covariance matrix estimation (section “Modified T2 statistics”). The T2 statistics with modified covariance matrices were compared against the conventional HT2 test, along with various alternative detection methods from the literature. To keep this work concise, results are presented for just the best-performing methods from the literature, which were the modified q-sample uniform scores statistics from Stűrzebecher et al. (1999) and Cebulla et al. (2006). Methods that were excluded from the results section are instead considered in the Discussion. This includes the previously best-performing adult CAEP detection method, that is, a template-based dynamic time warping (DTW) approach (Chesnaye et al., 2021a) and some of its variations. Comparisons were also drawn with visual inspection results from three experienced audiologists. Finally, test significance was evaluated using a recently developed frequency-domain bootstrap approach (Chesnaye et al., 2021b), and the assessment was carried out using aided CAEP measurements from 59 infant hearing aid users, as well as simulated signals.
Methods
This section describes the infant CAEP data and the objective detection methods, after which the procedures for evaluating test performance are described, which include an assessment of specificity, sensitivity, and reliability.
CAEP Data
Aided CAEP measurements were previously recorded from 103 infants (aged 3–7 months) with mild to profound bilateral hearing loss. Standard otoscopy and tympanometry examinations were carried out, and hearing aids were checked to confirm that these were working as intended. For the CAEP examination, the infants were seated in a soundproof booth on their caregiver's lap, approximately 1.1 m directly in front of an Eminence Alpha-6A 8 Ω loudspeaker (Eminence Speaker LLC, Eminence, KY). CAEPs were then evoked using 70 ms duration synthetic speech tokens with 10 ms duration raised-cosine onset and offset ramps, presented at a rate of approximately 0.9 Hz. These synthetic stimuli comprised either harmonics 6–11 of a tone with a 140-Hz fundamental—henceforth denoted as the mid-frequency stimulus, or MF—or an inharmonic series of closely-spaced tones spanning 2800–4500 Hz, to produce a fricative-like phoneme—henceforth denoted as the mid-high frequency stimulus, or HF. The levels of the individual components in each stimulus were chosen so as to produce a uniform excitation of the cochlea in a bandwidth that was at least the width of four normal auditory filters (Glasberg & Moore, 1990). The relative levels of the stimuli were referenced to the power contained within the same bandwidth of the International Speech Test Signal (ISTS, Holube et al., 2010) compared to the overall level of the full-bandwidth level of the ISTS. The relative levels were −14.5 and −20.6 dB for the MF and HF signals, respectively, compared to the full-bandwidth level. For clarity, we reference the presentation levels of each stimulus to the full bandwidth level of the ISTS from which they would have been derived, and label this the “Speech Reference Level” (SpRefL). So, for the MF stimulus presented at 65 dB SpRefL, the actual level of the stimulus during its steady-state portion was (65–14.5) = 50.5 dB SPL. A more extensive description and rationale for the design of the stimuli is described in Stone et al. (2019).
The stimuli were presented at 65 dB SpRefL (for 66 infants), 75 dB SpRefL (29 infants), and either 79 dB SpRefL (MF stimulus, 8 infants) or 85 dB SpRefL (HF stimulus, 8 infants). Throughout the CAEP test, an experienced paediatric audiologist aimed to keep the infant's attention facing towards the loudspeaker by using a selection of silent toys. The stimuli were then presented repeatedly until 20 artefact-free epochs had been recorded using an artefact rejection threshold of ± 110 μV and a band-pass filter of 1–100 Hz. A total of four blocks for the MF stimulus and four for the HF stimulus were presented using an interleaved approach. This procedure was then repeated, with the stimulus order reversed, giving 160 artefact-free epochs, per stimulus (although in some recordings there were 159 epochs). The full CAEP test procedure was repeated within seven days. If the repeat session was on the same day, a break of at least 1 h was given before starting the next session. Finally, CAEP measurements were made using electrodes placed at the high forehead (Fpz; active electrode), the right mastoid (reference electrode), and the left mastoid (ground electrode), and were recorded at a sampling rate of 30 kHz (downsampled to 500 Hz for further analysis) using the Eclipse system (Interacoustics, Middelfart, Denmark). Data were filtered offline from 1 to 15 Hz using 3rd-order Butterworth filters. Ethics approval was obtained from the North West National Research Ethics Service Ethics Committee (reference 15/NW/0736).
Visual Reinforcement Audiometry
To determine the audibility of the stimuli presented during the CAEP sessions, aided behavioral hearing thresholds to the same stimuli were estimated using visual reinforcement audiometry (VRA; BSA, 2014). As VRA requires behavioral conditioning, it was performed several months after the CAEP sessions. Infants were aged between 7.4 and 21 months, with a mean age of 10.8 months. VRA was performed by two experienced pediatric audiologists who followed the British Society of Audiology recommended procedure as a guideline (BSA, 2014). During the VRA sessions, stimuli were presented at a rate of 4 Hz using the same set-up previously described for the aided CAEP sessions. Infants were first conditioned at a high test level with simultaneous presentation of a visual reinforcer. An adaptive procedure was then used to find threshold in 5 dB step sizes. One audiologist kept the child's quiet attention in the room, and the other controlled the sounds from the observation room, and judged when a response was present. Intermittent control trials and long gaps were included to judge for false responses, but the tester was not blind to these. At the VRA session, standard hearing aid checks, otoscopy examinations, and tympanometry examinations were again carried out. If hearing aid settings had changed since the CAEP sessions, the VRA was performed while wearing temporary hearing aids of the same model as used during the CAEP session and set to their previous settings. Hearing aid settings were also checked in a test box for consistency between the CAEP and VRA sessions. The decibel Sensation Level (dB SL) was estimated as CAEP presentation level minus the aided VRA-estimated behavioral threshold, both recorded in dB SpRefL in the sound field.
Which Participants to Include
To accurately evaluate the performance of the detection methods, it is important that the estimated audibility of the CAEP stimuli is accurate. Participants were therefore excluded if the dB SL of the CAEP stimulus could not be accurately estimated. More specifically, the criteria for exclusion were: (i) middle ear dysfunction during CAEP or VRA test sessions, which could affect the recorded sensation level, (ii) progressive or fluctuating hearing loss between the sessions, and/or (iii) unreliable or missing behavioral thresholds. Additionally, one infant was excluded who was not aided at the time of the CAEP test, and another who used a bone conduction hearing aid. This resulted in a total of 59 and 57 infants with reliable dB SL estimates for the MF and HF stimuli, respectively (Table 1). Two recordings were available per participant giving a total of 118 recordings from 59 participants for MF, and 114 recordings from 57 infants for HF.
An overview of the number of recordings available for the analysis, per dB SL category and per stimulus type.

Objective detection methods
All objective detection methods were applied to the 700 ms windows following stimulus onset, as some infants had relatively late and/or long-lasting responses (see also Figure 1). For the frequency-domain detection methods, all 700 ms windows following stimulus onset were transformed to the frequency domain using the fast Fourier transform (FFT), giving a spectral resolution of ∼1.43 Hz. Note that the FFT was applied to the individual epochs, and not to their coherent average data.

All 45 CAEP template waveforms where a CAEP was deemed present by all three audiologists. Each panel shows waveforms from a single infant, and includes waveforms evoked by either the mid frequency (MF) or the mid-high frequency (HF) stimulus from sessions one or two, giving a maximum of four waveforms per infant. These waveforms were used to emulate CAEPs in simulations for the sensitivity assessment. Note that these waveforms were obtained by averaging across ensembles of 160 epochs, whereas the audiologists were originally reviewing coherent average replicates of 80 epochs.
The one-sample Hotelling's T2 test
The one-sample Hotelling's T2 (HT2) test is the multivariate equivalent to Student's one-sample t-test (Hotelling, 1931), and is one of the more commonly used methods for CAEP detection (e.g., Carter et al., 2010; Chang et al., 2012; Chesnaye et al., 2021a; Golding et al., 2009; Van Dun et al., 2012). When applied in the time domain, features consist of mean voltages, taken across short time intervals within epochs, henceforth referred to as “voltage means.” Extracting Q voltage means from an ensemble of N epochs gives an NxQ-dimensional matrix of features, say 
Frequency Domain Features for T2Freq
When the HT2 test is applied in the frequency domain—henceforth referred to as “T2Freq”—features are the real and imaginary parts of the Fourier components of W spectral bands (e.g., Chesnaye et al., 2018), and form the Nx2W-dimensional feature matrix
Evaluating Test Significance
Statistical inference on the T2 statistic was carried out using conventional F-distributions, which can be derived from theory based on the assumption that epochs are independent, and that data are stationary and normally distributed. The T2 statistic is transformed into an F-statistic using
Modified T2 statistics
The aim for the modified T2 statistics is to prevent low HT2 test sensitivities at small sample sizes by exploiting prior knowledge of the correlation structure underlying the data, which allows an improved estimate of the feature covariance matrix. In the time domain, data is assumed to follow a Toeplitz covariance structure, whereas in the frequency domain, independence between spectral bands is assumed.
Time Domain Modification T2Toep
A time series with Toeplitz covariance implies that the expected covariance between any two data points is dependent only on their time difference (Mukherjee & Maiti, 1988), which is satisfied for random stationary signals. When Toeplitz covariance is met, then the covariance matrix of the voltage means (previously denoted by
In what follows, note the distinction between voltage means extracted from the epochs, and the voltage means extracted from the continuous recording. For the voltage means extracted from the continuous recording, Toeplitz covariance implies the following property:
When Toeplitz covariance (Equation 2) is met, then covariance matrix 

Note that the number of unknown parameters in 
The degrees of freedom for this modified version of HT2 test differ from the conventional HT2 test, which prevents the convenient use of the F-statistic usually employed with HT2, but the bootstrap approach provides a simple, albeit computationally intensive, alternative (section “Frequency Domain Bootstrap”).
Frequency Domain Modification T2Diag
For the frequency domain HT2 modification, the asymptotic independence between spectral bands and real and imaginary components, expected from theory for stationary signals, is exploited. This leads to all covariances being zero, giving the following diagonal covariance matrix:
Additional analysis presented in the Supplemental Digital Content shows that the SNR was not equal across spectral bands, which suggests that it may be beneficial to include band-specific weights, with larger weights being placed on the high SNR bands relative to the low SNR bands. The weighted T2 statistic is then given by:
Modified q-sample uniform scores test
The original q-sample uniform scores test (Mardia, 1972) can be used to test whether the phases of multiple spectral bands share the same underlying distribution. The modifications proposed by Sturzebecher et al. (1999) and Cebulla et al. (2006) consider the amplitudes of the spectral bands, in addition to the phases. The modifications are furthermore applied either to the actual values, or to the ranks of the phases and amplitudes, where the ranking is performed across all spectral bands and all epochs, that is, rank values (for either the phases or the amplitudes) range from 1 to N·W, where W is the number of frequency bands included in the analysis. The current study includes four variations: (i) QMod V1, applied to phase ranks and amplitude values, (ii) QMod V2, applied to phase ranks and amplitude ranks, (iii) QMod V3, applied to phase values and amplitude ranks, and (iv) QMod V4, applied to phase values and amplitude values. The test statistic, say QMod, is given by (Cebulla et al., 2006):
Where
Frequency Domain Bootstrap
The frequency domain bootstrap (FDB) is an approach for generating many additional recordings, or “surrogates” (Chesnaye et al., 2021b; Dahlhaus & Janas, 1996). By applying the adopted detection method to a large number of surrogate recordings that satisfy the null hypothesis (i.e., no response present), a distribution of test statistics can be generated, henceforth the “bootstrapped distribution.” It is assumed that the bootstrapped distribution approximates the true null distribution underlying the test statistic. In order to obtain a good approximation, it is important that the surrogate recordings are representative of data under the null hypothesis, which requires certain data characteristics to be emulated, such as power and serial correlation between samples in each recording. In particular, for a given recording, say Estimate the power spectral density (PSD) underlying Generate random surrogate PSDs by adding random variation to the estimated PSD through: Transform the random surrogate PSDs to magnitudes, and assign a random phase to each frequency bin where the phases are randomly sampled from a uniform distribution on the [−π, π] interval. For the time domain detection methods, take the inverse FFT to obtain time-domain surrogates. Analyze the random surrogates with the detection method to generate a distribution of test statistics, which can be assumed to approximate the recording-dependent null distribution underlying the test statistic.
A crucial parameter underlying the performance of the FDB is the length of the sliding window within Welch's method, applied to
Visual Inspection by Audiologists
The infant CAEP data were first evaluated by three experienced audiologists who determined whether a CAEP was present or absent in accordance with guidelines provided by the British Society of Audiology (Lightfoot et al., 2016). Data were presented to the audiologists as two replicates of the coherently averaged epoch where each replicate was obtained by averaging 80 epochs. The coherent average replicates were presented from −150 to + 750 ms relative to stimulus onset, with the y-axis fixed at −15 to + 15 μV. The examiners then made the decision of either (i) response present, (ii) response absent, or (iii) ambiguous. The ambiguous option was included to more accurately represent real-world test conditions where clinician's similarly have the choice to remain undecided, and potentially collect more data to resolve any ambiguities (Lightfoot et al., 2016). Data were furthermore presented to the examiners randomly, with no knowledge of subject ID or stimulus level, and with no knowledge of the output of the statistical detection methods. The aim for the visual inspection was to obtain a score to compare the performance of the objective detection methods against. Audiologists’ assessments also formed the basis for constructing a sample of CAEP waveforms, which were later used to emulate CAEP signals in simulations, as described in section “Test Sensitivity”.
Test Specificity
The specificity of the detection methods was evaluated using false-positive rates (FPRs), defined as the rate at which H0 is rejected when H0 is true. Ideally, the FPR should equal the significance level of the test, also known as the nominal α-level, set here to 0.01. Data for the specificity assessment consisted of the inaudible (<0 dB SL) CAEP recordings, as well as simulated data to provide a more powerful assessment using a large number of tests where the ground truth of response absence was known.
Simulations
Data for the simulations consisted of stationary, Gaussian-distributed colored noise with spectral content similar to the inaudible (<0 dB SL) infant CAEP recordings. The colored noise was generated by filtering Gaussian white noise with all-pole filters, where the poles of the filters were given by the parameters of 20th-order autoregressive (AR) models. The AR parameters were estimated using the Yule-Walker approach (Hayes, 1996) with a new model being fitted to the EEG signals of each inaudible CAEP recording (44 in total). The resulting colored noise was then processed in a manner similar to the recorded EEG signals, that is, band-pass filtered from 1 to 15 Hz using a 3rd-order Butterworth filter, and structured into ensembles of either N = 20, N = 40, N = 80, or N = 160 approximately 1111 ms long epochs, corresponding to an approximately 0.9 Hz stimulus rate. The initial 700 ms windows of the ensembles were then analyzed with the detection methods. A total of 10,000 ensembles were simulated, per ensemble size.
Infant CAEP Data
The inaudible CAEP recordings were structured into ensembles of N epochs, where N again took values of either 20, 40, 80, or 160 epochs, to probe specificity with clinically more desirable small numbers of epochs. As the stimuli were deemed inaudible (<0 dB SL), no distinction was made between data from the MF and HF stimuli, nor between test sessions. There were sufficient data to assemble 347, 171, 83, and 44 ensembles, for N = 20, 40, 80, and 160 epochs, respectively. The 700 ms post-stimulus windows of the ensembles were analyzed with the objective detection methods. For the visual assessments, FPRs were evaluated for the N = 160 test condition, that is, 44 waveforms were visually inspected by each examiner.
Post-hoc Analysis
To determine whether the FPRs deviated significantly from the 0.01 α-level, 99% confidence intervals were constructed using binomial distributions. A binomial distribution represents the distribution of m “successful” Bernoulli trials out of M total trials performed. For the current analysis, a successful Bernoulli trial is defined as a false-positive, and hence has a theoretical probability equal to the nominal α-level of 1%. The total number of Bernoulli trials M is furthermore given by the total number of tests performed, and equals 10,000 for the simulations, which resulted in 99% confidence intervals of [0.0076, 0.0127] for α = 0.01. For the infant CAEP recordings, there were sufficient data for 44 tests (N = 160), 83 tests (N = 80), 171 tests (N = 40), and 347 tests (N = 20), giving 99% confidence intervals of [∼0, 0.081], [∼0, 0.055], [∼0, 0.038], and [∼0, 0.028], respectively.
Test Sensitivity
Test sensitivity was evaluated using the true-positive rate, defined as the rate at which H0 is rejected when H0 is indeed false. Test sensitivity should ideally be as high as possible, albeit for a fixed FPR and ensemble size N. Test sensitivity was evaluated using the audible (≥0 dB SL) CAEP recordings and simulated signals.
Simulations
Data for the simulations consisted of simulated colored noise for representing the EEG background activity (generated as described in the specificity assessment above) and CAEP template waveforms for simulating a response. The CAEP templates were given by the coherently averaged waveforms where all three audiologists agreed that a clear CAEP was present, that is, a relatively strict criterion was used. This helps to ensure that the simulated CAEPs are indeed CAEPs, as opposed to background activity. A total of 45 CAEP template waveforms were available for the simulations, presented in Figure 1. For each ensemble of colored noise, a CAEP was simulated by randomly selecting one of the 45 templates, rescaling the template to obtain a certain SNR, and adding it to all epochs within the ensemble in question. The SNRs for the simulated CAEPs furthermore ranged from −20 to −8 dB, which covered the range of SNRs estimated from the infant CAEP recordings. The SNR was estimated using:
Infant CAEP Data
The audible CAEP recordings were divided into three categories, including the 0–10 dB SL, the 10.1–20 dB SL, and the >20 dB SL categories. A distinction was now also made between the MF and HF stimuli, but no distinction was made between test sessions. The recordings were again structured into ensembles of size N = 20, 40, 80, or 160 epochs, and the 700 ms post-stimulus intervals were analyzed with the objective detection methods.
Post-hoc Statistical Analysis
Post-hoc analysis was carried out to test whether the detection rates of the methods differed when considered across all audible dB SL conditions, stimuli, and test sessions, but per ensemble size. For each detection method, the total number of detections (using α = 0.01) and non-detections were counted, after which Fisher's exact test (Fisher 1922; Fisher 1932) was used to test whether the number of detections and non-detections differed between methods, per ensemble size. The same approach was used when drawing comparisons between the detection methods and the examiners, except that there was now just a single ensemble size, equal to N = 160.
Test Reliability
This section evaluates intra- and inter-test reliability for the examiners and the objective detection methods. For CAEP detection, intra-test reliability—also known as test-retest reliability—is the extent to which a detection method or an examiner tends to reach the same conclusion in two separate recordings, where both recordings were obtained under the same test conditions, that is, the same test subject, the same stimulus type, stimulus rate, pre-processing parameters, etc. Inter-test reliability, on the other hand, is the extent to which detection methods and/or examiners agree on whether a CAEP is indeed present or not in any given recording. Both intra- and inter-test reliability were evaluated using Cohen's kappa statistic (Cohen, 1960; McHugh, 2012), further described below. In what follows, all “ambiguous” test outcomes for the examiners were treated as non-detections, giving a binary “CAEP detected” versus “no CAEP detected” test outcome. This facilitates the comparison between the examiners and the detection methods, as the detection methods similarly give a binary “H0 rejected” (CAEP detected) or “H0 not rejected” (no CAEP detected) test outcome.
Intra-Test Reliability

Tables that were constructed when calculating Cohen's kappa statistic for the intra- and inter-test reliability assessment.
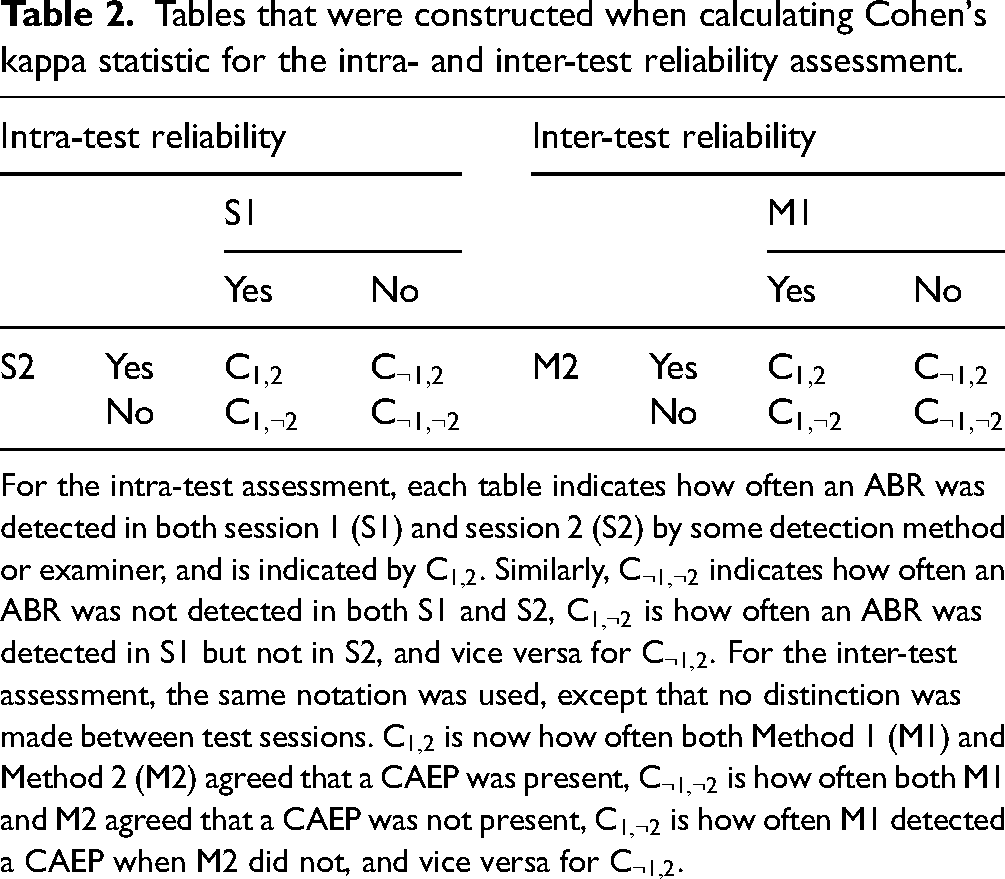
For the intra-test assessment, each table indicates how often an ABR was detected in both session 1 (S1) and session 2 (S2) by some detection method or examiner, and is indicated by




Inter-Test Reliability
Data for the assessment again comprised the infant CAEP recordings, except that no distinction was made between test sessions. For the inter-test assessment, Cohen's kappa represents the extent to which detection methods and/or examiners agreed on whether a CAEP was present or not. It is again helpful to first construct Table 2 (right panel); Note that
Post-hoc Statistical Analysis
To help interpret the estimated 
Results
This section presents the results from the specificity, sensitivity, and reliability assessments. Within the interest of remaining concise, results were not presented for all four q-sample modifications. Instead, just the best-performing modification was presented, which was QMod V3 (applied to phase values and amplitude ranks). The performance between all 4 q-sample modifications was, however, quite similar, and can be seen in Figure A.2. in the Supplemental Digital Content.
Examiner Results
The visual inspection results from the examiners are presented as stacked bar plots in Figure 2, which show the rates at which (1) a clear response (CR) was detected, (2) a response was deemed absent (response absent, or RA), or (3) the waveform was deemed ambiguous in terms of CR or RA. Results are presented for all three examiners (indicated by E1, E2, and E3), per dB SL category, and per stimulus type (i.e., MF or HF). Note that for the <0 dB SL category, no distinction was made between stimuli. If it is assumed that the inaudible recordings were indeed inaudible and did not contain a CAEP, then results show true-negative rates (TNRs; it is correctly concluded that a CAEP was absent) ranging from ∼0.3 (for E3) to ∼0.8 (for E1). For the audible test conditions, non-detection rates ranged from 0 to ∼0.55. Whether these non-detections can be considered as false-negative (i.e., it is concluded that a CAEP was absent when a CAEP was in fact present) is not clear—see also the Discussion. Detection rates for the inaudible recordings (assumed to be FPRs) were 0.068 for E1 and 0 for both E2 and E3. For the audible recordings, detection rates ranged from ∼0.15 to ∼0.65.

Results from the visual inspection by audiologists, presented as stacked-bar plots. Each bar represents the rates at which a clear response (CR) was detected, a response was deemed absent (response absent, or RA), and the waveform was deemed ambiguous in terms of CR or RA. Results are presented per dB SL category, for both the mid-frequency (MF) and the mid-high frequency (HF) stimulus, and for all three examiners, indicated by E1, E2, and E3. Note that for the <0 dB SL condition, no distinction was made between the MF and HF stimuli, as the stimuli were deemed inaudible.
Test Specificity
Simulations. The FPRs of the detection methods (Table 3) mostly fell within the 99% confidence intervals for α = 0.01. The exception was QMod V3, which showed a liberal (FPR > α = 0.01) test performance at N = 40. In general, FPRs show a small bias towards a liberal test performance for the bootstrapped test statistics at small ensemble sizes of N = 20 and N = 40, which decreases for increasing N, and can likely be attributed to variance in the power spectral density estimates (
False-positive rates (FPRs) for the objective detection methods in simulations (left panel) and for the inaudible (<0 dB SL) infant CAEP recordings (right panel).

Significant (p < .01) deviations from α = 0.01 are indicated by an asterisk to ensure that the comparison in test sensitivity in subsequent analyses were fair, the nominal α-levels were adjusted, per detection method, such that their FPRs equal 0.01 (middle panel). The (b) indicates that test significance was evaluated using the frequency domain bootstrap.
Infant data. The FPRs of the detection methods for the inaudible infant CAEP recordings are also shown in Table 3 (right panel). All FPRs fell within the expected 99% confidence intervals for α = 0.01. However, it is worth emphasizing that there was relatively little data for the assessment, which resulted in wide confidence intervals for α = 0.01. This may have prevented small deviations from the α-levels from being detected.
Test Sensitivity
Simulations. The detection rates using the adjusted α-levels are shown in Figure 3 for N = 20, 40, 80, and 160. Results show that detection rates for the conventional HT2 test were relatively poor for N = 20 and N = 40 (panels A and B, respectively), but improved for larger ensemble sizes: For N = 80, similar detection rates were observed for HT2 and QMod V3, whereas for N = 160, HT2 outperformed QMod V3. The highest detection rates were consistently observed for the modified T2 statistics.
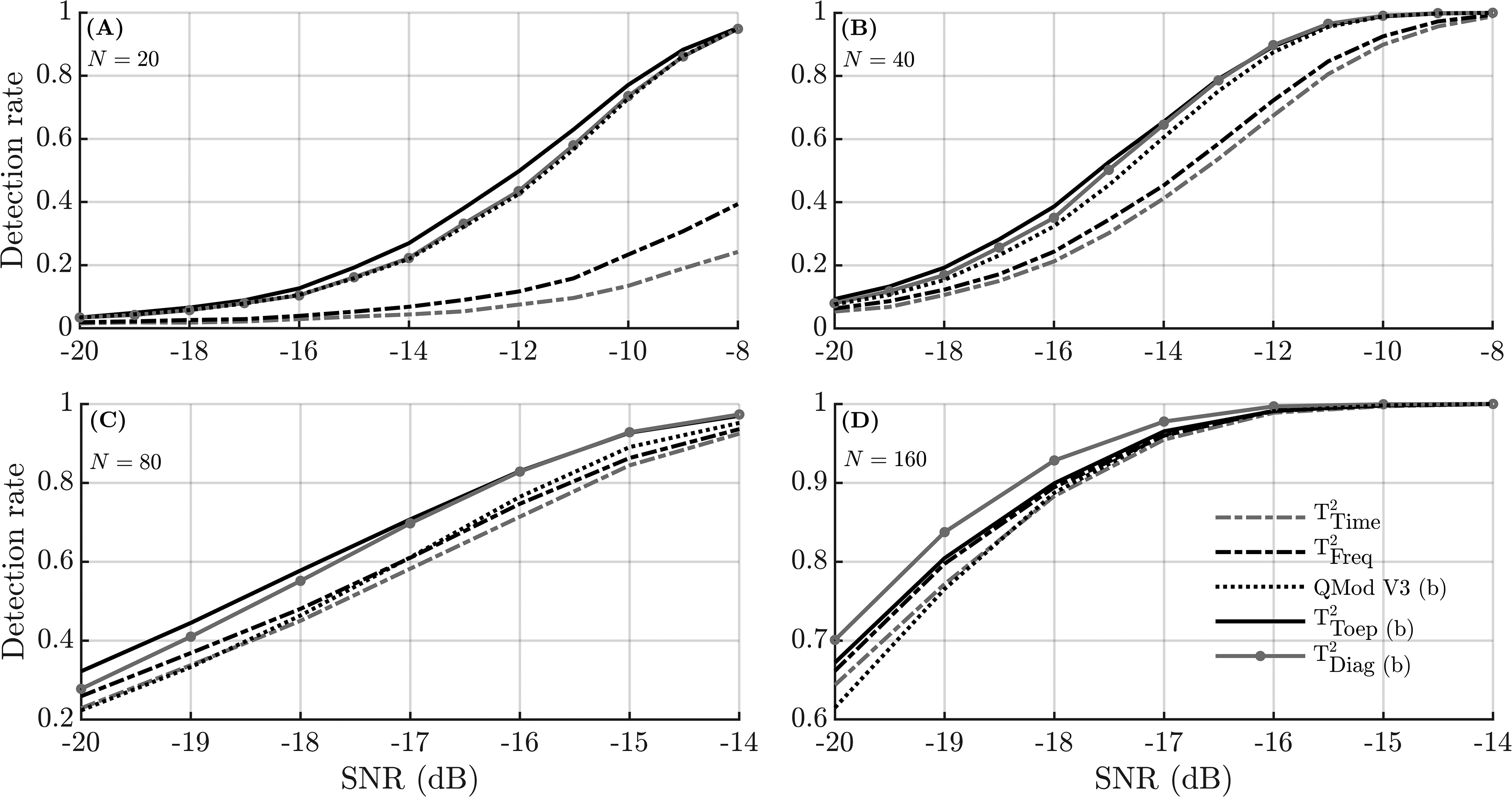
Simulation results showing the detection rates as a function of the SNR for different ensemble sizes N. To ensure a fair comparison between methods, the detection rates were generated using adjusted α-levels (Table 3). Note that the y-axis and x-axis for panels (C) and (D) are on a different scale than panels (A) and (B). The (b) in the legend indicates that test significance was evaluated using the frequency domain bootstrap.
Infant data. The detection rates for the objective detection methods are presented per dB SL category and per ensemble size in Figure 4, for both the MF stimulus (top panels) and the HF stimulus (bottom panels). For the smaller ensembles sizes of N = 20 and N = 40, results again suggest that the modified T2 statistics and QMod V3 outperformed the conventional HT2 test (i.e., T2Time and T2Freq), which was confirmed by results from the post-hoc statistical analysis, shown in Table 4. For N = 80, T2time was also significantly (p < .05) outperformed by both QMod V3 and T2Diag, whereas for N = 160, no significant differences between the detection rates were observed (p > .05).

Detection rates for the audible infant CAEP recordings for both the objective detection methods and the examiners. Results are presented for the mid-frequency (MF) stimuli (top panels) and the mid-high frequency (HF) stimuli (bottom panels), per dB SL category. The numbers associated with each dB SL category indicate how many ensembles were tested.
Results from the post-hoc statistical analysis for the sensitivity assessment, i.e., the p-values generated by Fisher's exact test (section “Test Sensitivity”) when comparing the detection rates amongst objective detection, and between detection methods and examiners.

This analysis considered all audible (≥0 dB SL) CAEP recordings simultaneously and made no distinction between sessions or stimulus type. All pair-wise comparisons with significantly (p < .05) different detection rates are indicated by an asterisk. Results show that T2Time and T2Freq were significantly outperformed by T2Toep, T2Diag, and QMod V3, primarily at N = 20 and 40. The (b) indicates that test significance was evaluated using the frequency domain bootstrap.
To help facilitate the comparison between the examiners and the detection methods (at N = 160), examiner detection rates from Figure 2 were also included in Figure 4 (right panels). Examiner detection rates ranged from ∼0.15 to ∼0.4 for the HF stimulus, and from ∼0.3 to ∼0.65 for the MF stimulus. For the best-performing detection methods (i.e., the modified T2 statistics and QMod V3), detection rates for N = 160 were in the ∼0.2 to ∼0.65 range for the HF stimuli, and in the ∼0.3 to ∼0.8 range for the MF stimuli. Results from the post-hoc statistical analysis (Table 4) confirm significantly higher detection rates for QMod V3, T2Diag, and T2Toep relative to the examiners.
Finally, increasing the α-level to 0.05 for the objective detection methods resulted in detection rates ranging from ∼0.45 to ∼0.75 for the HF stimuli, and from ∼0.45 to ∼0.9 for the MF stimuli. Additional analysis (details not presented) also demonstrate similar detection rates when using both the adjusted and the non-adjusted α-levels. Results in Figure 4 were generated using the non-adjusted α-levels.
Test Reliability
Results from the reliability assessment are presented in Table 5, and show Cohen's kappa values for the intra- and inter-test reliability assessments. For the intra-test reliability assessment (i.e., test-retest reliability),
Cohen's Kappa values from the intra- and inter-test reliability assessments.

For the intra-test reliability assessment,
Discussion
This study evaluated various new and existing objective methods for aided CAEP detection in infants with hearing loss, and aimed to improve the accuracy and efficiency of CAEP measurements in this population. Results firstly confirm the “large p small n” problem (Li et al., 2017) for the HT2 test, which was previously hypothesized to be due to poor estimates of the feature covariance matrix (Bai & Saranadasa, 1996). Indeed, improved test sensitivities were obtained by replacing the conventional feature covariance matrix with either the Toeplitz (Equation 4) or the diagonal (Equation 5) covariance matrix.
Some alternative modifications for preventing low HT2 test sensitivities have previously also been proposed in the literature. These have been categorized by Dong et al. (2016) as: (1) the “unscaled T2 statistics” where the feature covariance matrix is removed from the T2 statistic (e.g., Bai & Saranadasa, 1996; Zhang & Xu, 2009), (2) the “regularized T2 statistics” where a regularization factor is applied to the feature covariance matrix (Chen et al., 2011), and (3) the “diagonal T2 statistics” where all covariances are set to zero, giving a diagonal covariance matrix (e.g., Witten & Tibshirani, 2011). The T2Diag statistic proposed in the current work falls in the third category, but is specifically justified for the frequency domain HT2 test due to statistics of the Fourier Transform coefficients from stationary signals. The T2Toep statistic falls outside this classification scheme, but is again based on prior knowledge (or the assumption) of signal stationarity.
Alternative Detection Methods
Other detection methods published in the literature were initially also included in the assessment, but were removed from the final results to remain concise. These include various alternative modified q-sample statistics from Cebulla et al. (2006), the Fsp (Elberling & Don, 1984), the Fmp (Martin et al., 1994), the “mean power” statistic (Lv et al., 2007), the DTW approach (Chesnaye et al., 2021a), and the diagonal HT2 test from Bai and Saranadasa (1996).
Starting with the diagonal HT2 test (Bai & Saranadasa, 1996), this approach—not previously evaluated for CAEP detection—is essentially the conventional time domain HT2 test where the feature covariance matrix is replaced with the diagonal covariance matrix, that is, covariances between all voltage means are set to zero. The approach also includes a rescaling factor for transforming the modified T2 statistic into a standard normally-distributed random variable, after which the asymptotic (for
In a previous study on CAEP detection in adults with normal hearing, the best-performing method was a DTW approach, which correlates the (time-warped) ensemble coherent average to an a priori assumed CAEP template (Chesnaye et al., 2021a). Due to the wide variation in CAEP waveforms across infants (Figure 1), the DTW approach was not expected to perform optimally in this young population. Indeed, detection rates for the DTW approach were around 0.4 or lower in the infant data, even at N = 160, and detailed results were excluded from the results section. We also attempted a range of template matching variants, such as using a database of templates, but none provided encouraging results.
Test Specificity, Sensitivity, and Reliability
Results from visual inspection by examiners show good test specificities but relatively low test sensitivities, that is, detection rates (using N = 160) for the audible (≥0 dB SL) CAEP recordings were in the ∼0.3 to ∼0.65 range for the MF stimuli, and in the ∼0.15 to ∼0.4 range for the HF stimuli. The low test sensitivity for visual inspection appears potentially problematic for clinical decision making with aided CAEP. For the best-performing objective detection methods, detection rates for N = 160 were slightly higher, for example, T2Toep had detection rates in the ∼0.25 to ∼0.65 range for the HF stimulus, and in the ∼0.3 to ∼0.8 range for the MF stimulus. Increasing the
Detection rates in this study were approximately in the same range as those observed in previous studies. For example, Van Dun et al. (2012) observed detection rates (using the conventional HT2 test) for aided CAEPs in hearing-impaired infants of ∼0.53 for the 0–9.9 dB SL category, ∼0.67 for the 10–19.9 dB category, and ∼0.77 for the 20 + dB SL category. Similarly, Chang et al. (2012) observed detection rates (using the conventional HT2 test) of ∼0.63 for the >0 dB SL category, ∼0.68 for the >10 dB SL category, and ∼0.69 for the >20 dB SL category, for aided and unaided CAEP detection in hearing-impaired infants. Note that these studies used an
With respect to intra-test reliability (or test re-test reliability), relatively low
For the inter-test reliability assessment,
Finally, inter-test reliability scores for the examiners were lower than those of the objective detection methods (
Study Limitations and Future Work
This study aimed to provide a fair comparison between aided CAEP detection methods, and therefore carried out feature optimizations (presented in the Supplemental Digital Content) prior to the main assessments. Feature optimizations prevent some methods from having an unfair advantage over others due to sub-optimal feature sets, but have a potential risk in that some methods have more capacity to be optimized than others, that is, some methods may have been overfitted to the sample of CAEP recordings. Although results in the Appendix suggest that test performance was relatively robust across a range of test parameters, it is important that results are confirmed using alternative data sets in future work.
An additional limitation for this work is that there were relatively few inaudible (<0 dB SL) CAEP recordings available for the specificity assessment. As a result, statistical power was low, which may have resulted in small biases in the FPRs of the detection methods going undetected. The large sample of simulated signals overcomes this limitation to some extent, but does not fully emulate real-world recordings, and was not carried out for visual inspection due to the substantial load on the clinicians. In future work, it may be necessary to estimate FPRs for the detection methods and examiners using a much larger sample of no-stimulus recordings.
It should also be noted that any longitudinal studies that compare tests on children at different ages (in this case CAEP testing at 3–7 months followed by VRA testing at mean age 10.8 months), and where the tests have some source of variability, have inherent limitations. Both VRA and CAEP have some test variability due to the attention of the child and measurement noise resulting from child movement, that is, neither test is entirely a gold standard measurement of audibility. Although the current study strived to reduce sources of variability in measurements—e.g., by (1) carrying out otoscopy and tympanometry examinations to rule out variations due to conductive elements, (2) excluding infants with progressive or fluctuating hearing loss, and (3) testing hearing aids using a test box prior to the examinations—data should be treated with some caution.
Finally, the detection methods in this study made no distinction between epochs within an ensemble, and therefore implicitly assumed that the CAEP was a deterministic response, unchanging throughout the examination. However, the CAEP is known to be affected by habituation (Özesmio et al., 2000) and subjects’ drowsiness or state of alertness (e.g., Celesia & Puletti, 1971; Johnson & Yonovitz, 2007), thus rendering significant trial-to-trial variations plausible. Indeed, Johnson & Yonovitz (2007) observed gradual changes in CAEP amplitudes and latencies over the course of a 90-min test paradigm and found these changes to be associated with fluctuations in alertness and attentiveness. Further work is required to explore these variations in infants with hearing loss, quantify their impact on CAEP detection methods, and test potential solutions.
Conclusion
The overall best-performing methods to detect CAEPs in this study were the modified T2 statistics, which outperformed QMod V3 in simulations, and the conventional HT2 test in both simulations and aided CAEP recordings from 59 hearing-impaired infants. The reduced test sensitivity for the conventional HT2 test was primarily for small ensemble sizes, and was attributed to the “small n large p” problem underlying HT2. For larger ensemble sizes of 80 epochs or more, the low test sensitivity was less pronounced. With respect to the visual inspection results of the examiners, good test specificities were observed, but relatively low test sensitivities, which could be problematic for clinical applications. Finally, results from the reliability assessment suggest that some audible CAEP recordings might not have contained clear CAEP waveforms. Future developments in CAEP detection might therefore aim to optimize CAEP test paradigms for efficiently and reliably evoking CAEPs in infants with hearing loss, and to further improve objective CAEP detection methods to assist clinicians with interpreting the CAEP waveforms.
Supplemental Material
sj-docx-1-tia-10.1177_23312165231154035 - Supplemental material for Modified T2 Statistics for Improved Detection of Aided Cortical Auditory Evoked Potentials in Hearing-Impaired Infants
Supplemental material, sj-docx-1-tia-10.1177_23312165231154035 for Modified T2 Statistics for Improved Detection of Aided Cortical Auditory Evoked Potentials in Hearing-Impaired Infants by Michael Alexander Chesnaye, Steven Lewis Bell, James Michael Harte, Lisbeth Birkelund Simonsen, Anisa Sadru Visram, Michael Anthony Stone, Kevin James Munro and David Martin Simpson in Trends in Hearing
Footnotes
Acknowledgments
The authors would like to thank the families for taking part, and the audiologists and teachers of the deaf for helping to recruit to the study. The authors would also like to thank Jo Brooks, Caroline Hudson, Amber Roughley, and Rhianon Morgan for data collection.
Author Contributions:
M.A.C., D.M.S., S.L.B, and J.M.H. contributed toward algorithm design and data analysis. A.S.V., L.B.S., K.J.M., and S.L.B. contributed towards data acquisition and/or data interpretation. All authors contributed toward project conception, experiment design, and towards the drafting and critical revision of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number PB-PG-0214-33009). K.J.M. and M.A.S. were supported by the NIHR Manchester Biomedial Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. This work was funded by the William Demant Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.