
Abstract
There is growing evidence linking hearing impairment to higher falls risk through alterations in postural stability, with studies showing mixed results. The primary aim of this systematic review and meta-analysis was to determine the association between hearing impairment and postural instability in older adults, including differences based on severity of hearing impairment. This review was pre-registered in PROSPERO and performed in accordance with PRISMA guidelines across six databases. Primary research on adults aged 60 years and older with hearing loss and an objective measure of postural stability or gait were eligible for inclusion. Methodological quality was assessed using the modified Newcastle-Ottawa Scale (NOS) adapted for cross-sectional studies. Data were analysed using meta-analyses and a narrative synthesis. Inclusion in the meta-analyses required clearly defined audiometrically-assessed hearing impairment, and two subgroups of participants: mild (25–40 dB HL) and moderate to-severe (>40 dB HL) hearing impairment. Twenty-five eligible studies (n = 27,847) were included in the narrative synthesis, with quality ratings ranging from unsatisfactory to very good on the modified NOS. Eight studies were included in the meta-analysis which showed individuals with moderate to-severe hearing impairment were significantly slower on the 5 x sit-to-stand test (mean difference[95%CI] = 0.50 s [0.04, 0.97], p = .03), had a slower gait speed (mean difference[95%CI] = −0.11 s [−0.16, −0.05], p < .001) and had lower total Short Physical Performance Battery scores (mean difference[95%CI] = −0.79[−1.17, −0.41], p < .001) than those with normal hearing. This review provides evidence there is an inverse association between increasing severity of hearing impairment and poorer postural stability across both the meta-analysis and narrative synthesis.
Introduction
Hearing impairment is considered a global public health crisis (Tordrup et al., 2022), affecting approximately 20.3% (1.59 billion people) of the global population (World Health Organisation, 2021). This percentage increases to between 40% and 60% in people aged 60 years and older (Agrawal et al., 2009; Cuda et al., 2021). Hearing loss is the third leading cause for years lived with disability worldwide (Tordrup et al., 2022), affecting factors such as quality of life (Davis & Hoffman, 2019), communication (Kramer et al., 2002), cognition (Lin, 2011) and social participation (Dalton et al., 2003). here is growing evidence that hearing impairment contributes to reduced postural stability, increasing falls risk and hospitalisation rates (Agmon et al., 2017; Bang et al., 2020; Genther et al., 2015), with research noting the odds of a fall in the preceding 12 months increases 1.4 times with every 10 dB HL increase in hearing impairment above 25 dB HL (Lin & Ferrucci, 2012). Globally, falls pose a significant economic burden to the health care system, with a systematic review showing the mean cost of falls ranged from US $3,476 per faller to US $26,483 per fall that requires hospitalisation (Davis et al., 2010).
A common risk factor for falls is reduced postural stability (Pua et al., 2017) essentially, the ability to control the body in space to maintain an upright posture in relation to both postural orientation and equilibrium (Horak, 2006). This is achieved via complex integration of visual, vestibular and somatosensory inputs to drive an appropriate motor response (Chaudhry et al., 2004). There is growing evidence that the auditory system has a role in postural stability. There are currently several potential explanations in the literature for an association between postural instability and hearing impairment in older adults. The first suggests a significant association between hearing impairment and vestibular dysfunction in older adults, specifically abnormalities to otolithic function (Abd El-Salam, 2018; Kurtaran et al., 2016; Todd et al., 2000; Zuniga et al., 2012). Reduced otolith function has been shown to correlate with increased mediolateral postural sway during standing balance tasks (Serrador et al., 2009) which is a known risk factor for falls (Maki et al., 1994; Serrador et al., 2009). Secondly, potential higher-level changes in central integration of postural stability information, thought to occur due to hearing impairment could result in an increased cognitive demand. This in turn may adversely impact postural stability in older adults with hearing impairment when compared with those with normal hearing (Koh et al., 2015; Pichora-Fuller et al., 2015; Wollesen et al., 2018). Thirdly, the association between postural instability and hearing impairment could be related to altered spatial awareness as a result of reduced auditory cues (Keller et al., 1999). During ambulatory tasks, both binaural and monoaural cues are dynamically changing as the person moves. This creates a pattern of auditory information known as acoustic flow that assists to maintain postural stability in motion by creating a representation of the surrounding space to better stabilise the body (Campos et al., 2018; Deviterne et al., 2005; Gandemer et al., 2014; Pichora-Fuller et al., 2016). Finally, both poor hearing and impaired postural stability may be markers of other processes reflective of ageing. Overall, studies have previously shown that the richer the auditory environment, the smaller the degree of postural sway (Gandemer et al., 2017). Thus, older adults with hearing impairment could have increased postural sway as they are less receptive to available auditory information. Regardless in all explanations, it follows that more severe hearing impairment could result in more impaired postural control; however, further exploration into this theory is required.
There have been two previous systematic reviews completed exploring hearing impairment and falls. One examining the association between hearing impairment and falls in any age group (Jiam et al., 2016), and one examining the association between hearing impairment, postural control, and mobility in older adults (Agmon et al., 2017). Jiam et al. (2016) completed the first systematic review and meta-analysis, including 12 eligible studies. They found the odds of falling were 2.39 times greater in those with hearing loss than those with normal hearing. However, several limitations were identified including substantial between-study heterogeneity (Q = 631, p < .05, I2 = 98.1%) including variations in the population studied, how hearing loss was defined, how falls were assessed and whether confounders were considered in the analysis. Odds of falling were calculated based primarily on self-reports by the participants, therefore potentially leading to information or recall bias. A year later, Agmon et al. (2017) included seven studies in their review and found a significant, positive association between hearing impairment and several objective measures of postural control after controlling for major covariates. They too reported limitations relating to inconsistent hearing evaluation methods and between-study heterogeneity.
Since these reviews, several studies have examined the association between hearing impairment postural stability and falls (Bruce et al., 2019a, 2019b; Deal et al., 2017; Gorecka et al., 2018; Huang et al., 2019; Kamil et al., 2016; Martinez-Amezcua et al., 2021; Thomas et al., 2018; Vitkovic et al., 2016; Yévenes-Briones et al., 2021). Findings from these studies continue to report mixed outcomes, therefore a systematic review and meta-analysis that includes the results of these more recent studies is warranted. The primary aim of this review was to comprehensively and systematically answer the research question ‘Is hearing impairment associated with postural stability in older adults?’. A secondary research question was ‘does this association change depending on the severity of the hearing impairment?’.
Methods
Protocol and Registration
This systematic review was prospectively registered with the International Prospective Register of Systematic Reviews (CRD42020155545). Reporting of this study has adhered to the standards recommended by the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines (PRISMA) (Page et al., 2021).
Information Sources and Search Strategy
A systematic search of PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane, Scopus, Web of Science and Embase databases was performed on 23rd March 2022. Cross-sectional, longitudinal and correlational studies on hearing loss and postural stability in older adults published between January 1, 1950, and November 4, 2019, were identified. A total of 616 new articles were published between November 4th, 2019, and this search time. In total, 75 progressed to a full text assessment, 50 were excluded and 25 included in the systematic review (See Figure 1 PRISMA Flow Chart). To ensure a comprehensive thorough search of the literature and data sources, an experienced librarian informationist at The University of Queensland was engaged. The search strategy was formulated using medical subject terms targeting three domains: hearing impairment, postural stability and older adults. Key words pertaining to hearing impairment included: ‘hearing disorders’, ‘Auditory diseases central’, ‘Otosclerosis’, ‘deafness’, ‘Hearing loss’, ‘presbycusis’, ‘Tinnitus’ and ‘Hearing impairment’. Key words pertaining to postural stability included: ‘postural balance’, ‘walking’, ‘mobility limitation’, ‘falls’, ‘postural stability’, ‘postural control’ and ‘stumble’. The following key words were included to identify studies relating to older adults: ‘elderly’, ‘geriatric’, ‘aging’, ‘elders’, ‘senior citizen’ and ‘retired’. References of relevant studies were examined to ensure a comprehensive search of existing literature. Please see Supplementary Material, for full details of the electronic search strategies.

PRISMA Flowchart of Study Selection for Systematic Review. CINAHL = Cumulative Index to Nursing and Allied Health Literature.
Study Selection and Eligibility Criteria
Two reviewers (J.I.F. and M.M.) independently reviewed the title and abstracts to select studies that met the pre-defined inclusion and exclusion criteria. Study selection and data extraction were performed using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia). Inclusion criteria were: (1) human studies, (2) study population aged 60 years and older with hearing loss, (3) study reports on an objective measure of postural stability, or gait and (4) primary research. Exclusion criteria were: (1) duplicate articles, (2) population characteristics (i.e., aged <60 yrs and/or no hearing loss reported), (3) participants diagnosed with a neurological or peripheral vestibular condition (e.g., stroke, Parkinson's disease, BPPV, Meniere's disease, etc.), (4) no objective measure of postural stability (e.g., self-report or questionnaire), (5) not relevant to study question and (6) study design (e.g., review, position paper, single case study, incomplete data, etc.). Articles that were included based on the title and abstract screening then underwent full-text screening by both investigators independently to ensure the inclusion and exclusion criteria were met. Disagreements or discrepancies between investigators were resolved via team discussion, with a third investigator available if a consensus was not met.
Data Extraction
The following data items were extracted from all included studies and provided in detail in Table 1: study design, participant characteristics, auditory measure, measure of postural stability and study outcomes (Page et al., 2021). When study information, participant characteristics or other necessary data were absent, the corresponding authors were contacted. All necessary data was obtained using this method. One reviewer independently collected all key data points. This data was then confirmed by an additional independent reviewer. No automation tools were used for this process. Any objective measure of postural stability or gait were considered eligible data for inclusion, with no limit placed on how postural stability was objectively measured.
Study Characteristics.

Note. N = number of participants; OA = Older Adults; YA = Younger Adults; NormH = Normal Hearing; HI = Hearing Impaired; Mod = Moderate; Mod-Sev = Moderate to Severe; Sev = Severe; PTA = Pure Tone Average; SPPB = Short Physical Performance Battery; SOT = Sensory Organisation Test; MCT = Motor Control Test; Vestib = Vestibular; Dysfx = Dysfunction; CoP = Centre of Pressure; NSD = No Significant Difference; SLS = Single Leg Stance; EO = Eyes Open; BMD = Bone Mineral Density; STS = Sit To Stand; FAEO = Feet Apart Eyes Open; FAEC = Feet Apart Eyes Closed; FTEO = Feet Together Eyes Open; FTEC = Feet Together Eyes Closed; M-L = Medio-Lateral sway; A-P = Antero-Posterior sway.
Quality of Evidence
The methodological quality of included studies was assessed using the modified Newcastle-Ottawa Scale (NOS) adapted for cross-sectional studies (Herzog et al., 2013). Using this scale, the literature quality is assessed across three domains: selection, comparability and outcome. Selection includes sample representation, sample size justification, whether non-respondents were recorded, and how exposure (in this case presence of hearing impairment) was ascertained. Comparability looks at how confounding factors were or were not controlled and outcome includes whether a validated and objective method was used and the statistical quality. The scale is graded out of 10 points, with 9–10 points indicating very good study quality, 7–8 points indicating a good study, 5–6 points a satisfactory study and 0–4 points indicating an unsatisfactory study. Quality appraisal was completed independently by two reviewers (J.I.F. and S.G.B.). These scores were then compared, and any discrepancies were resolved via team discussion to create a mutually-agreed quality score for each included study.
Data Synthesis and Analysis
Data analysis was completed using the Cochrane Review Manager software, RevMAN v. 5.4.1 (https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download). Meta-analyses were performed using a random effects model and graphically displayed using Forest plots. Statistical heterogeneity was assessed using Higgins I2 test, with an I2 value greater than 50% considered to indicate larger heterogeneity (Higgins & Thompson, 2002; Higgins et al., 2003).
The main analysis was conducted to examine the association between hearing impairment and postural stability outcomes. Three measures of postural stability were used most consistently across different papers and therefore were included in the meta-analysis: the time taken for 5x sit to stand test, gait speed and Short Physical Performance Battery total score. The 5x sit to stand test measures the time taken to sit and stand five times from a seated position (Goldberg et al., 2013; Muñoz-Bermejo et al., 2021). It is commonly used to assess functional mobility in older adults (Whitney et al., 2005), difficulties with this test have been associated with lower limb strength (Bohannon et al., 2010), imbalance (Lord et al., 2002), gait abnormalities (Whitney et al., 2005) and falls risk (Buatois et al., 2010). Reduced gait speed has been associated with impaired postural stability (Almarwani et al., 2016) and increased falls risk in older adults (Brodie et al., 2014). The Short Physical Performance Battery is a combination of three tests: standing balance for 10 s in 3 different stance positions, gait speed and 5x sit to stand time with a total score out of 12 (higher score indicating better lower extremity function). Poor SPPB scores have been associated with falls risk (Lauretani et al., 2018), impaired mobility (Guralnik et al., 2000; Vasunilashorn et al., 2009) and postural instability (Tabue-Teguo et al., 2018).
Some studies included all participants with hearing impairment as one group, and others separated participants into groups based on severity of hearing impairment. To avoid duplicating results, subgroup analyses were performed for those with mild hearing impairment (defined as audiometry results of 25–40 dB HL) and moderate to-severe hearing impairment (defined as audiometry results of >40 dB HL) (World Health Organisation, 1991).
Results
Search Results
In this study, 7,870 abstracts were screened, 75 full text articles reviewed and 25 studies included for qualitative synthesis. Figure 1 provides the PRISMA flow chart for these search results. No additional articles were identified from the reference lists of the articles and no eligible articles surfaced in our search strategy that needed translation.
Study Characteristics
Twenty-five studies involving a total of 27,847 participants across 12 countries were included in this systematic review (see Table 1). Included studies were primarily cross-sectional observational in design (n = 18). Baseline data measurements were extracted from four longitudinal studies (Table 1; Huang et al., 2019; Martinez-Amezcua et al., 2021; Viljanen et al., 2009a, 2009b), and one randomised controlled trial (Table 1; Bruce et al., 2019b). Recruitment methods varied between the studies and included largely research participant pools from universities, patients within Otoneurological and Ear, Nose Throat clinics as well as nationally-representative samples of Medicare enrolees and those from a senior welfare centre.
Seventeen of the included studies examined postural stability in older adults with hearing impairment (Bruce et al., 2019a; Chen et al., 2015; Gorecka et al., 2018; Kamil et al., 2016; Koh et al., 2015; Kowalewski et al., 2018; Mikkola et al., 2015; Sakurai et al., 2021, 2022; Szeto et al., 2021; Thomas et al., 2018; Tomioka et al., 2015; Viljanen et al., 2009a, 2009b; Vitkovic et al., 2016; Wollesen et al., 2018; Yévenes-Briones et al., 2021). One study investigated the association between hearing impairment and physical activity (Gispen et al., 2014). Six studies examined the association between hearing impairment, postural stability and a third factor; cognition (Bruce et al., 2019b; Huang et al., 2019; Sakurai et al., 2022), bone mineral density (Mendy et al., 2014), atherosclerosis (Deal et al., 2016; Martinez-Amezcua et al., 2021) and vestibular dysfunction (Tan et al., 2011). The final study evaluated postural stability in the elderly more generally, however did state that all participants had some degree of hearing impairment (Barozzi et al., 2005).
Postural Stability Outcome Measures
For a study to be included, it needed to utilise an objective measure of postural stability; however, the measure used varied greatly between studies. The most consistent was the time taken to complete the 5x sit to stand (5xSTS) test (Bruce et al., 2019a, 2019b; Chen et al., 2015; Deal et al., 2016; Kamil et al., 2016; Martinez-Amezcua et al., 2021; Mikkola et al., 2015; Wollesen et al., 2018; Yévenes-Briones et al., 2021). This was followed by the Short Physical Performance Battery (Chen et al., 2015; Deal et al., 2016; Martinez-Amezcua et al., 2021; Mikkola et al., 2015; Wollesen et al., 2018; Yévenes-Briones et al., 2021). Gait speed was also measured in a number of studies, with variations in path length (ranging from 2.4 m to 10 m) and pace instructions (comfortable or fast pace) (Chen et al., 2015; Deal et al., 2016; Huang et al., 2019; Mikkola et al., 2015; Sakurai et al., 2021, 2022; Szeto et al., 2021; Tomioka et al., 2015; Viljanen et al., 2009a; Wollesen et al., 2018). Multiple studies included some form of standing balance assessment, which varied in duration (10–60s), foot position (feet apart, feet together, tandem, single leg) and surface (firm, foam). Five studies analysed Centre of Pressure (CoP) with various systems including a Wii® balance system (Nintendo, Kyoto, Japan) (Vitkovic et al., 2016), Good balance system (Metitur Ltd, Jyväskylä, Finland) (Viljanen et al., 2009b), FreeMED (Sensor Medica, Rome, Italy) (Thomas et al., 2018) and the Equitest® (NeuroCom International Clackamas) (Barozzi et al., 2005; Bruce et al., 2019a). The remaining studies utilised measures such as the Timed Up and Go (TUG) Test (Koh et al., 2015) and Actigraph data to measure mean daily minutes of moderate and vigorous physical activity daily (Gispen et al., 2014). Three studies examined postural control under dual task conditions. Two used customised platforms delivering perturbations in the forward direction with and without an auditory memory task while measuring degree of body sway using a 3-dimensional motion capture system (Bruce et al., 2019a; Kowalewski et al., 2018), CoP movement and reaction times (Bruce et al., 2019a; Victoria, 2018). The other (Gorecka et al. (2018) recorded spatio-temporal gait parameters while walking with and without dichotic listening conditions.
Quality Assessment
Table 2 shows the summarised quality assessment (using the modified NOS), with scores ranging from 3 (unsatisfactory) to 10 (very good), averaging 7.47 ± 1.8. The overall quality level was considered very good for 10 studies, good for 8 studies, satisfactory for 6 studies and one study was considered unsatisfactory.
Quality Rating of Included Studies Using the Modified NOS.
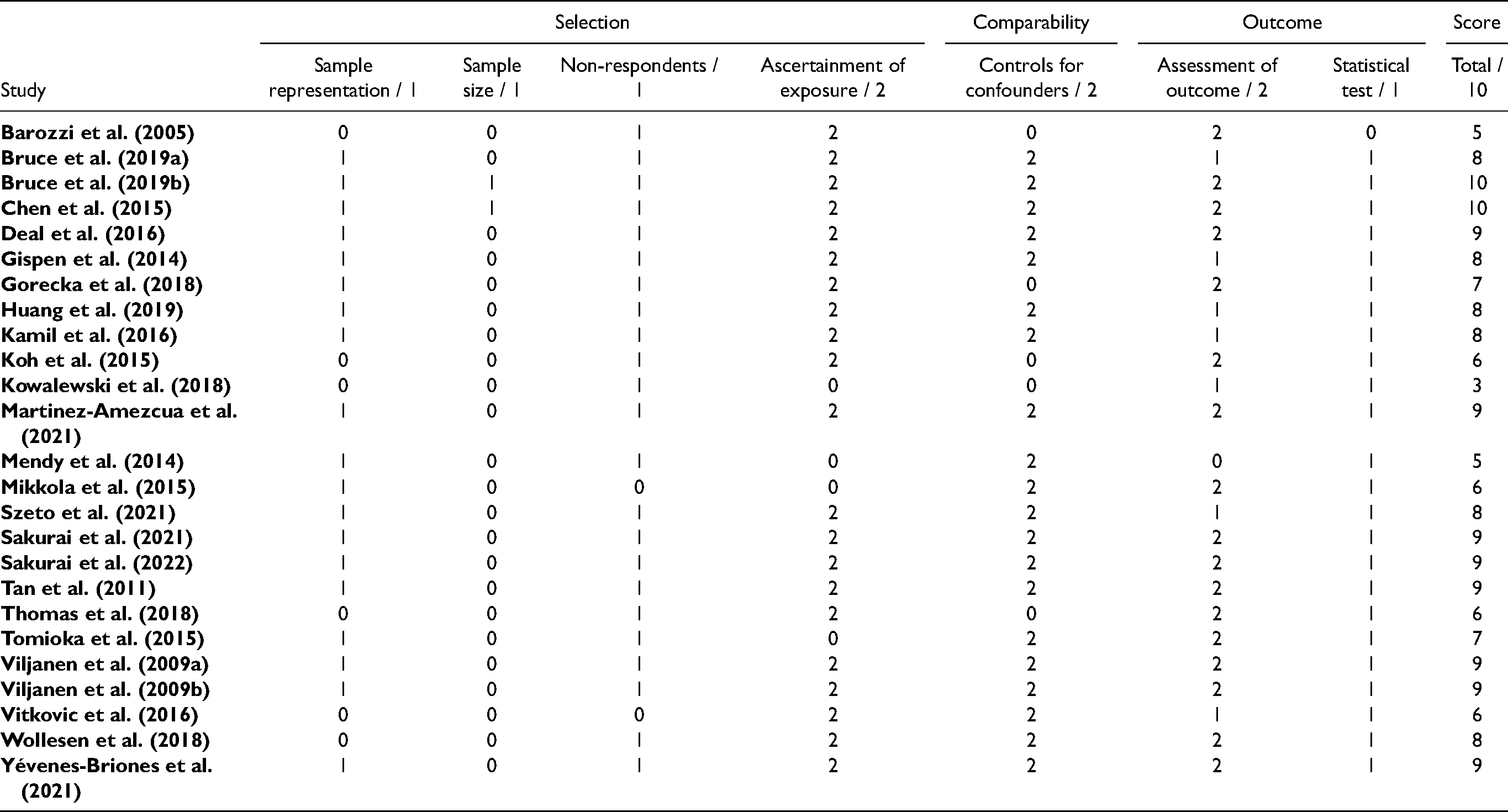
Two studies met the criteria for all seven elements of the modified NOS (Bruce et al., 2019b; Chen et al., 2015) as they had appropriate justification of sample selection, controlled for confounding variables, used objective and validated outcome measures and appropriate statistical analyses These were the only two studies to include a justification of sample size. Participants were considered to be a true representation of the sample in 20 of the included studies, with the remaining five studies using convenience sampling and different recruitment methods for hearing impaired and normal hearing groups. A summary of non-respondents was documented in 23 of the 25 studies, with the remaining two studies having different sample size numbers described in the methodology as those reported on in the results (Mikkola et al., 2015; Tan et al., 2016).
Auditory status of the participants was measured objectively via an audiogram in 21 of the included studies. Three of the remaining studies utilised self-report with questions varying from self-rating of no, little, or significant hearing trouble, (Mendy et al., 2014), or a specific question; ‘do you feel you have a hearing loss?’ (Tomioka et al., 2015) and ‘do you have difficulty hearing when conversing with another person in a noisy environment?’ (Mikkola et al., 2015). The final study (Kowalewski et al., 2018) stated they recruited participants with normal hearing and those with a bilateral hearing loss. However, they did not specify how this was measured prior to administering the outcome measures, which included sentence-in-noise tasks.
Confounders of age, sex and cardiovascular risk factors were controlled for in 20 of the included 25 studies, with many studies also including confounders of education, otological concerns, cognition and arthritis. Although the outcome measures used to measure postural stability varied greatly between studies, 17 studies used an objective, validated measure, 7 studies utilised a non-validated measure and one used a non-standard method (Thomas et al., 2018). All studies except (Barozzi et al., 2005) used statistical testing that was clearly described.
Meta-analysis
Eight studies were identified for inclusion in meta-analyses due to the common postural stability outcome measure used (Figure 2A–H). All eight studies were of good to very good quality according to their modified NOS scores. The meta-analyses examined difference in postural stability (either 5x STS time, gait speed, or SPPB score) between hearing impairment groups. Some studies grouped data for all participants with hearing impairment, and others separated into groups based on severity of hearing impairment. The meta-analyses described in Figure 2A–H detail the subgroup analyses comparing postural stability between those with either moderate-severe or mild hearing impairment and those without hearing impairment, or between those with moderate-severe and mild hearing impairment. Three studies used the same measures of postural stability however were excluded from the meta-analysis, due to (1) absence of audiometry testing (Mikkola et al., 2015), or (2) gait speed capture protocols where gait speed was captured over a longer distance (10 m) (Tomioka et al., 2015) and at a fast pace (Viljanen et al., 2009a), which differed from the other studies.
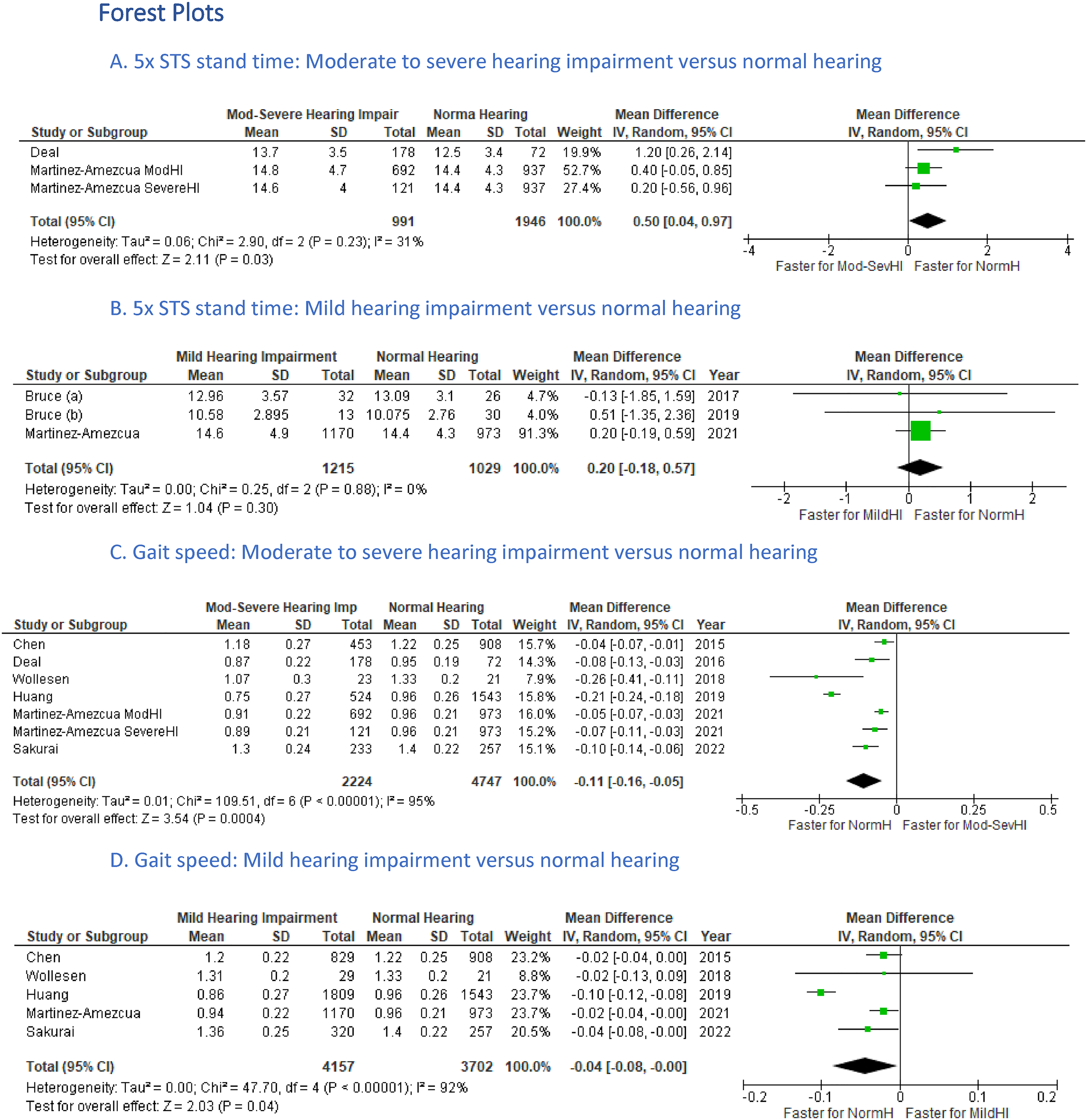
(A–H) Forest Plots of 5xSTS; Gait Speed and Total SPPB Score for Moderate to Severe Hearing Impairment Versus Mild Hearing Impairment and Normal Hearing Groups.
Differences in 5xSTS Time Across Hearing Impairment Groups
Figure 2A showed that those with moderate to-severe hearing impairment had significantly longer 5xSTS time (mean difference = 0.50s, 95%CI = 0.04, 0.97, p = .03) than those with normal hearing. This comparison had no statistically significant differences in heterogeneity an I2 = 31% (p = .23), reflecting that the studies showed little variability in their outcome measure mean differences, which may have reflected low clinical diversity, (Figure 2A). In contrast, there were no significant differences in 5xSTS time between those with mild hearing impairment and those with normal hearing (mean difference = 0.20 s, 95%CI = −0.18, 0.57, p = .30) (Figure 2B). This comparison also had no statistically significant differences in heterogeneity an I2 = 0% (p = .88). The study excluded from the meta-analysis, due to the absence of an audiometrically defined hearing impairment (Mikkola et al., 2015), reported results in line with the meta-analysis finding, showing significantly longer 5xSTS time for those with major subjective hearing difficulty compared to those with no reported hearing difficulty and no difference in 5xSTS time between hearing impairment groups.
Differences in Gait Speed Across Hearing Impairment Groups
In a meta-analysis of six studies, those with moderate to-severe hearing impairment had significantly slower gait speeds than normal hearing groups (mean difference = −0.11 s, 95%CI = −0.16, −0.05, p < .001) (Figure 2C). However, the included studies had significant heterogeneity (I2 = 95%, p < .001). Those with mild hearing impairment also walked significantly slower than those with normal hearing; however, this difference was not as large as that of the moderate to-severe hearing impairment groups (mean difference = −0.04 s, 95%CI = −0.08, −0.00, p = .04) (Figure 2D). This comparison also demonstrated high heterogeneity (I2 = 92%, p < .001). When comparing hearing impairment groups, those with moderate-to-severe hearing impairment had significantly slower gait speed than those with mild hearing impairment (mean difference = −0.06 s, 95%CI = −0.10, −0.03, p < .001) with significant heterogeneity between studies (I2 = 86%, p < .001) (Figure 2E).
Differences in Total SPPB Score Across Hearing Impairment Groups
Those with moderate-to-severe hearing impairment had significantly lower total SPPB score (mean difference = −0.79, 95%CI = −1.18, −0.41, p < .001) and significant heterogeneity (I2 = 78%, p = .001) when compared to those with normal hearing (Figure 2F). In contrast, no significant differences in total SPPB scores were noted between mild hearing impairment and normal hearing groups (mean difference = −0.29, 95%CI = −0.60, 0.03, p = .08). As with the moderate to-severe hearing impairment group heterogeneity was again high (I2 = 80%, p = .002) (Figure 2G). When comparing hearing impairment groups, those with moderate to-severe hearing impairment had significantly lower total SPPB scores than those with mild hearing impairment (mean difference = −0.68, 95%CI = −1.19, −0.17, p = .009) and significant heterogeneity between studies (I2 = 86%, p < .001) (Figure 2H). One study (Mikkola et al., 2015) was excluded from the meta-analysis due to absence of audiometry testing, yet their results reflected those found in the meta-analysis, with lower total SPPB scores in those with major self-reported hearing difficulty compared to those with normal hearing and no difference between those with some reported hearing difficulties to normal.
Narrative Synthesis
Thirteen of the 25 included studies investigated differences in standing balance across hearing impairment groups. Four of these studies included standing balance as part of the SPPB however did not analyse the standing balance component individually (Chen et al., 2015; Deal et al., 2016; Martinez-Amezcua et al., 2021; Yévenes-Briones et al., 2021). Barozzi et al. (2005) included an assessment of standing balance with feet together and eyes closed; however, they only included participants with hearing impairment and no comparator group and included no analysis of standing balance as an isolated measure. All remaining eight studies favoured an association between poorer standing balance and hearing impairment, regardless of standing balance testing protocol (variable base of support, surface, visual conditions), (Koh et al., 2015; Mendy et al., 2014; Mikkola et al., 2015; Tan et al., 2011; Thomas et al., 2018; Tomioka et al., 2015; Viljanen et al., 2009b; Wollesen et al., 2018), inferring that overall standing balance is impacted by hearing impairment no matter the difficulty or conditions of the standing balance task
Three studies extended their analysis of standing balance to include postural sway using force plates. Viljanen et al. (2009b) examined mean mediolateral and anteroposterior sway velocity and velocity moments during semi-tandem stance for 20 s in 429 older women, reporting a significant negative association between increasing severity of hearing impairment and increasing mediolateral sway velocity and velocity moments using the good balance system (Metitur Ltd, Jyväskylä, Finland). Thomas et al. (2018) supported these findings in 13 adults with moderate hearing impairment, reporting significant associations between hearing impairment and increased CoP ellipse areas, particularly in the sagittal plane for both feet together eyes open and eyes closed conditions using the FreeMED system (Sensor Medica, Rome, Italy). In contrast, Vitkovic et al. (2016) found no significant differences in postural sway measurements in 28 older adults with varying levels of hearing impairment when standing with feet apart or together, with eyes open or closed on both firm and foam surfaces for 60 s using a Nintendo Wii Balance board (Nintendo, Kyoto, Japan). The two studies used participants with varying degrees of hearing impairment; Vitkovic et al. (2016) had a mean hearing impairment of nearly 20 dB HL less than Thomas et al. (2018).
Two studies used the standardised static balance computerised dynamic posturography protocols available on the Equitest® (NeuroCom International Clackamas) to measure postural stability. Bruce et al. (2019b) found no significant differences in sway area between 12 older adults with hearing impairment and 30 with normal hearing. In contrast, Barozzi et al. (2005) reported that 90% of participants with a hearing impairment (Mean PTA 62 ± 3.4 dB HL) scored abnormally (high sway) on the SOT. This could potentially relate more to the differences in hearing impairment severity between the two studies with Bruce et al. (2019b) testing those with mild hearing impairment (PTA between 25 and 40 dB HL) whereas Barozzi et al. (2005) tested those with severe hearing impairment (mean PTA 62 ± 3.4 dB HL).
Two studies gathered spatiotemporal measures of postural stability during gait using an electronic walkway or instrumented insoles but were not included in the systematic review as they combined hearing impairment severity as a total with the mean hearing impairment at 39.0 dB HL(±9.7) falling directly across the mild and moderate to severe hearing-impaired sub-groups and therefore preventing them from being allocated into either meta-analysis subgroup. Results of both studies reflected those of the meta-analyses of gait speed, in that a poorer gait performance was found with greater hearing impairment. Sakurai et al. (2021) reported a significant correlation between reduced gait speed and higher stride length variability with increasing severity of hearing impairment. Using different measures, Szeto et al. (2021) found an increase in double support period variability with increasing hearing impairment severity.
Additional Outcome Measures
Two studies examined reactive postural stability using custom made perturbation platforms, delivering perturbations in the forward direction and repeated with an auditory memory task while measuring degree of body sway using 3-dimensional motion capture systems. Bruce et al. (2019a) assessed changes in cognitive performance and balance performance (as measured by degree of plantarflexion and hip extension) during these perturbations with varying levels of background noise. They found that unlike older adults with normal hearing, those with hearing impairment demonstrated lower cognitive performance when dual-tasking in noisy conditions, reflecting a ‘posture first prioritisation’, re-allocating cognitive resources to maintaining postural stability in the most challenging environments. Kowalewski et al. (2018) recorded the number of steps required to regain balance in response to surface perturbations and reported that older adults with hearing impairment required a greater number of steps to regain balance for all test conditions. However, it was not clear if the group effects were only due to hearing impairment, as the groups included young and older adults. Gorecka et al. (2018) also measured spatio-temporal gait parameters while walking at a comfortable pace and during a dual-task dichotic listening condition. They found hearing impairment modulated a reduction in gait speed, stride length, step length and increased step width during single and dual-task conditions in older adults compared to young adults. However, the impact of age on this modulating effect was not analysed.
The remaining three studies utilised more functional measures of balance outcomes. Koh et al. (2015) found no significant differences in TUG time for older adults with hearing impairment compared to those with normal hearing. Gispen et al. (2014) found those with moderate to-severe hearing impairment and not mild hearing impairment, had significantly lower daily and total step counts compared to those with normal hearing as detected using an Actigraph accelerometer. Finally, Yévenes-Briones et al. (2021), used the SPPB test series to create a grouping to reflect lower limb function (impaired lower limb function defined as a total SPPB score ≤6). They grouped all data for those with mild and moderate to-severe hearing impairment and found a significant association between hearing impairment and impaired lower extremity function.
Discussion
This systematic review of 25 studies including meta-analyses suggests that older adults with moderate to-severe hearing impairment have poorer postural stability when compared to those with normal or mild hearing impairment. All meta-analysis outcomes (5xSTS time, gait speed and SPPB score) from eight studies showed that those with moderate to-severe hearing impairment performed significantly poorer than those with normal hearing. In contrast, those with mild hearing impairment only showed reduced gait speed when compared with adults with normal hearing. Aligning with these results, those with moderate to-severe hearing impairment had significantly slower 5xSTS times, slower gait speeds and lower total SPPB scores than those with mild hearing impairment.
The majority of studies in the narrative synthesis also supported these findings in that poor postural stability measured with a variety of methods was associated with or worse in those with hearing impairment, when compared to those without hearing loss. In support, those studies that showed no difference or no association often included older adults with mild hearing loss.
These data support findings from a previous systematic review of seven studies, six of which were included in the current study, investigating the association between hearing impairment, postural control and mobility in older adults (Agmon, 2017). All studies included in this review by Agmon et al. (2017) demonstrated an association between hearing impairment and postural control across several aspects including gait speed, standing balance and walking endurance. This was the case even after controlling for major covariates such as comorbidities, smoking, physical activity and body mass index. The only other related systematic review was by Jiam et al. (2016) who investigated the association between hearing loss and a factor often related to postural instability – falls. They found the odds of falling were 2.39 times greater in those with hearing loss than those with normal hearing. While this systematic review did not include an analysis of falls risk or rates, reduced postural stability has been shown to be a direct risk factor for falls (Assantachai et al., 2003; Girard et al., 2014; Lin & Ferrucci, 2012; Maki et al., 1994; Pua et al., 2017). The current study expands the systematic review by Agmon (2017) by examining more papers/participants, including a meta-analysis, examining both static and dynamic aspects of postural stability, and investigating the impact of the severity of hearing impairment on postural stability.
Potential Rationales for Relationship Between Hearing Impairment and Postural Stability
The results of the meta-analysis and narrative synthesis suggest there is a relationship between the severity of hearing impairment and the severity of postural instability, irrespective of whether it is assessed statically or dynamically. There could be several potential reasons for this association.
First, the impact of aging and age-related physiological processes that impact hearing, postural stability and vestibular function needs to be considered. Age-related degeneration to the corpus collosum has been shown to cause reduced gait speed and neural presbycusis (Gates & Mills, 2005; Rosano et al., 2005). Age-related micro-vascular disease can also affect both the cochlear and lower limb function (Mikkola et al., 2015; Torre et al., 2005). However, an association between hearing impairment and reduced postural stability was still found despite confounders of age, sex and cardiovascular health being controlled for in 20 of the included 25 studies. This suggests there is more to this association than simply the effects of aging processes on both postural and auditory systems.
Another postulated explanation for these changes in postural sway and postural stability outcomes in those with hearing impairment is an association between hearing impairment and vestibular dysfunction in older adults (Abd El-Salam, 2018; Kurtaran et al., 2016; Todd et al., 2000; Zuniga et al., 2012). The otolith organs have a role in modifying antigravity muscle tone and as such, a reduction in otolith function has been shown to correlate with increased mediolateral postural sway (Farrell & Rine, 2014; Maki et al., 1994; Serrador et al., 2009). The saccule, one of the two otolith organs, shares a paired embryological origin with the cochlear (Todd et al., 2000; Zuniga et al., 2012). Due to this, it is postulated that pathologies affecting the cochlea may cause dysfunction of the saccule and hence changes to postural sway (Abd El-Salam, 2018; Doettl et al., 2021; Kurtaran et al., 2016; Todd et al., 2000; Zuniga et al., 2012). This relationship could also be a result of age-related neural degeneration affecting both the cochlear and vestibular systems concurrently therefore influencing postural stability (Agrawal et al., 2009; Baloh et al., 2003; Gispen et al., 2014). However, Lin & Ferrucci (2012) found an association between hearing impairment and falls even after controlling for vestibular function. Our systematic review did not encompass an analysis of vestibular function; however, the results did show a significant association between severity of hearing impairment, poorer standing balance and greater postural sway, specifically mediolateral sway (Viljanen et al., 2009b). This supports the potential role of changes in otolith and vestibular function in mediating postural sway patterns. Further research examining postural control and vestibular function in people with hearing impairment may assist in disentangling the relationship between these systems.
Another explanation could be related to the suggestion that postural stability and sway is influenced by changes in auditory cues which provide acoustic landmarks that assist in creating a representation of the surrounding space to better stabilise the body (Deviterne et al., 2005; Gandemer et al., 2014). Studies have previously shown that the richer the auditory environment the smaller the degree of postural sway (Gandemer et al., 2017). This suggests that older adults with hearing impairment could theoretically have increased postural sway as they are less receptive to available auditory information. None of the studies included in this review analysed postural sway changes in response to auditory cues in those with normal hearing and hearing-impaired individuals. However, Gorecka et al. (2018) did show that hearing impairment modulated a reduction in gait speed, stride length, step length and increased step width during dichotic listening conditions, which adds weight to the above theory. Further research looking at the effects of auditory cues on postural sway in those with hearing impairment and normal hearing individuals is warranted, particularly modulating the level of auditory stimulus to match the level of hearing impairment.
Attention may also play a role in the relationship between postural instability and hearing impairment. It seems that when dual tasking, older adults with mild hearing impairment tend to show a posture-first strategy to prioritise their postural stability over the cognitive task, often showing no change in balance performance but a deterioration in cognitive performance in this situation (Bruce et al., 2019a). Hearing impairment has been shown to increase cognitive demand due to higher-level changes in central integration of information, which can adversely impact on postural stability measures in older adults, particularly when attempting to dual task (Koh et al., 2015; Wollesen et al., 2018). Older adults have displayed a reduced ability to multi-task while performing challenging gait or balance tasks (Brauer et al., 2002; Siu et al., 2009), particularly those with a history of falls (Brauer et al., 2001). In the paper by Bruce et al. (2019a), postural prioritisation was unique to the mild hearing impaired group of participants who appeared to reallocate cognitive resources from cognitive working memory to the motor task in order to maintain postural stability (Doumas et al., 2008; Li & Lindenberger, 2002). This dual-task cost to cognitive compensation was not seen in older adults with normal hearing and was not examined in people with moderate-severe hearing impairment.
Limitations & Reliability of Results
Several limitations should be considered when interpreting the results of this review and meta-analysis. Firstly, among the eight studies included in the meta-analysis, there was substantial between-study heterogeneity (I2 between 80% and 96%). On comparing these studies more closely, we observed a marked variation in the populations studied, how hearing impairment was defined and how postural stability was assessed. The age of participants seemed to show the greatest discrepancy, with a variation of over 15 years between different studies. Meta-analysis of gait speed showed the highest between-study heterogeneity (I2 92–96%), which is likely a reflection of the variation in distance used to calculate gait speed, with this varying from 2.4 m to 10 m.
Although most studies used an audiometry evaluation of hearing impairment, the methods of testing and definitions of hearing impairment (including severity) differed between studies, reflecting the many definitions of degrees of hearing loss that exist (Timmer et al., 2015). For example, some studies measured average threshold frequencies of 500 Hz, 1 kHz, 2 kHz and 3 kHz across both ears, whereas others included 4 kHz (instead of 3 kHz) and in the better ear only. Most studies used similar threshold range definitions of normal hearing (<25 dB HL), mild HI (25–40 dB HL) and moderate to-severe HI (≥40 dB HL). However, an exception to this is Huang et al. (2019)'s paper, who used a screening test that classified people into normal, moderate or severe HI based on how many of six pure tones they heard in their worst ear, meaning that someone with normal hearing in one ear and severe or profound HI in the other would be included in the poor hearing group. Huang's results were included in the meta-analyses of gait speed only, these calculations were repeated with Huang removed and showed no change to the statistical significance of the results.
Study quality (as assessed using the modified NOS) was variable between studies, with an average score within the ‘good’ range (7.47 ± 1.8). Only two studies met all criteria, with the most common quality-related issues being justification of sample size, convenience sampling and summary of non-respondents. Study quality impacts the robustness of the results and may also have contributed to the high heterogeneity scores.
Study Implications and Future Directions
Hearing impairment is highly prevalent in the older population, experienced by over 60% of people aged 60 years and over (Agrawal et al., 2009). There is growing evidence on the association between hearing impairment and postural stability and negative health outcomes (Agmon et al., 2017; Bang et al., 2020; Genther et al., 2015). With our ageing population, there is an increasing need to investigate these relationships to contribute to preventative healthcare solutions and reduce disability. The findings of this review suggest those with at least moderate hearing impairment have significantly poorer postural stability than those with normal hearing. The detection of at least mild hearing impairment could be used as a method of identifying the need for further balance assessment and conversely, detection of postural imbalance could be a marker to warrant further hearing assessment. Declines in hearing could trigger implementation of a preventative balance rehabilitation program to prevent decline in postural stability, particularly during challenging dual-task conditions. Identification of a moderate or greater degree of hearing impairment could be a prompt to delve further into screening of postural stability and falls risk in these individuals. This review also supports the development of novel hearing interventions that take into account the potential associated postural stability deficits of these individuals. Further longitudinal and prospective cohort studies across people with a range of hearing impairment severities is required to establish causal associations.
Conclusion
This review provides evidence there is an inverse association between increasing hearing impairment and poorer postural stability. This association is statistically significant for those with moderate to-severe hearing impairment, however less so for mild hearing impairment. To elucidate the underpinning reasons, further studies utilising objective measures of auditory function that adhere to established audiometric definitions of hearing impairment, alongside measures of postural stability under specific conditions and potential contributing factors are needed.
Supplemental Material
sj-docx-1-tia-10.1177_23312165221144155 - Supplemental material for The Association between Hearing Impairment and Postural Stability in Older Adults: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-tia-10.1177_23312165221144155 for The Association between Hearing Impairment and Postural Stability in Older Adults: A Systematic Review and Meta-analysis by Jacinta I. Foster, Katrina L. Williams, Barbra H. B. Timmer and Sandra G. Brauer in Trends in Hearing
Footnotes
Acknowledgements
The authors wish to thank research assistant Ms. Katrina Kemp for her assistance on this project. The authors wish to thank research assistant Ms. Katrina Kemp and Mrs Marina Mahafza for their support in the screening and reviewing of the studies for inclusion in the review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Sonova AG as part of a larger study series. The grant sponsors were not involved in study design, collection, analysis or interpretation of data, writing of the manuscript or the decision to submit the manuscript for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.