
Abstract
The aim of the present study was to investigate the effect of ear asymmetry, order of testing, and gender on transient-evoked otoacoustic emission (TEOAE) pass rates and response levels in newborn hearing screening. The screening results of 879 newborns, of whom 387 (study group) passed screening successfully in only one ear in the first TEOAE screening, but passed screening successfully in both ears thereafter, and 492 (control group) who passed screening successfully in both ears in the first TEOAE, were retrospectively examined for pass rates and TEOAE characteristics. Results indicated a right-ear advantage, as manifested by significantly higher pass rates in the right ear (61% and 39% for right and left ears, respectively) in the study group, and in 1.75 dB greater TEOAE response amplitudes in the control group. The right-ear advantage was enhanced when the first tested ear was the right ear (76%). When the left ear was tested first, pass rates were comparable in both ears. The right-ear advantage in pass rates was similar in females versus males, but manifested in 1.5 dB higher response amplitudes in females compared with males, regardless of the tested ear and order of testing in both study and control groups. The study provides further evidence for the functional lateralization of the auditory system at the cochlear level already apparent soon after birth in both males and females. While order of testing plays a significant role in the asymmetry in pass rates, the innate right-ear advantage seems to be a more dominant contributor.
Keywords
Introduction
In humans, a large corpus of evidence supports functional lateralization of the auditory system from the cochlea to the cortex along the lifespan. This asymmetry found at different levels of the auditory pathways is already evident a few days after birth (e.g., Bertoncini et al., 1989; Sininger & Cone-Wesson, 2006; Thornton, Marotta, & Kennedy, 2003). At the cortical level, asymmetry was evident in newborns to speech stimuli presented to the right versus left ear (Bertoncini et al., 1989; Dehaene-Lambertz, Hertz-Pannier, & Dubois, 2006). Additional physiological evidence from newborns indicates asymmetry at the subcortical level. Specifically, brainstem responses to click stimuli were characterized by larger right Wave V amplitudes, shorter Wave III and Wave V latencies (Eldredge & Salamy, 1996; Sininger & Cone-Wesson, 2006), and Wave I to Wave V interpeak latencies in the right ear (Keefe, Gorga, Jesteadt, & Smith, 2008). At the cochlear level, most studies reported asymmetries between the right and left ears that manifested in higher prevalence of spontaneous otoacoustic emissions in the right ears (Burns, Arehart, & Campbell, 1992). Asymmetry between ears in newborns also manifested in transient-evoked otoacoustic emissions (TEOAEs) with larger amplitudes, whole wave reproducibility, and higher signal-to-noise ratio (SNR) in the right ears (Aidan, Lestang, Avan, & Bonfils, 1997; Berninger, 2007; Newmark, Merlob, Bresloff, Olsha, & Attias, 1997; Saitoh et al., 2006; Thornton et al., 2003). Taken together, these findings support an innate right-ear advantage manifested at the different levels of the auditory system.
OAE are routinely used nowadays while testing at-term newborns in universal newborn hearing screening (UNHS) programs aimed at detecting permanent congenital hearing loss as early as possible (Prieve, 2007). TEOAEs provide a reliable, quick, and noninvasive method, which enables testing each ear separately (Kemp, 2002). Since 1997, a UNHS program is operating routinely at the Sheba Medical Center with approximately 10,000 newborns tested each year. While testing newborns in our UNHS program using TEOAE, we observed that among newborns who initially failed in one ear, pass rates tended to be higher in the right versus the left ears. This observation led us to examine whether an asymmetry exists in initial newborn pass rates between the right and left ears. To date, only Berninger and Westling (2011) reported higher pass rates in the right versus the left ears among newborns who failed unilaterally TEOAE screening. If indeed such an asymmetry exists, it may be an additional manifestation of the right-ear advantage that can be documented soon after birth.
A potential contributing factor that may also affect TEOAE pass rates is the order of testing, that is, whether the right ear is tested before the left ear or vice versa. The effect of this factor has been investigated regarding TEOAE characteristics in newborns who initially passed screening successfully in both ears (Thornton et al., 2003). Specifically, a greater right–left TEOAE amplitude difference was found when the right ear was tested first, as compared with the difference found between ears when the left ear was tested first. The effect of testing order on the magnitude of the right–left asymmetry in TEOAE pass rates has not been systematically studied in newborns who did not initially pass screening in one ear. Only Berninger and Westling (2011) briefly dismissed the possibility that the order of testing affected the higher pass rates in right ears found in their study, as more than half of their newborns were first tested in the left ear.
Another factor that is known to affect TEOAE responses in newborns is gender, with greater TEOAE amplitudes in females versus males (Aidan et al., 1997; Berninger, 2007; Newmark et al., 1997; Saitoh et al., 2006; Thornton et al., 2003). The effects of right–left asymmetry and order of testing on TEOAE amplitudes were reported to be similar in males and females among newborns who initially passed screening successfully in both ears (Thornton et al., 2003). The effect of gender on pass rates among newborns who did not initially pass screenings in one ear is also yet to be determined.
Thus, the purpose of the present study was to assess whether ear asymmetry manifests in pass rates and TEOAE response levels while taking into account the potential contributing factors. Specifically, we evaluated the effects of ear, order of testing, and gender in two groups of healthy full-term newborns: (a) a study group—newborns who passed screening successfully in only one ear in the first TEOAE screening test, but passed screening successfully in both ears thereafter, and (b) a control group—newborns who passed screening successfully in both ears in the first TEOAE test.
Materials and Methods
Participants
Data from a population of newborns born during the first 3 months of 3 consecutive years (2006–2008) were extracted according to the following inclusion criteria: (a) full-term newborns (>37 weeks gestational age); (b) no pre- or postnatal complications; (c) first TEOAE screening test performed within the first 48 hr after birth; (d) no known risk factors for hearing impairment according to the Joint Committee on Infant Hearing position statement (2000); (e) both ears tested during the same screening session; (f) available data regarding the order of testing; and (g) passed successfully final TEOAE screening in both ears (initial TEOAE for control group and final TEOAE for study group).
The study group consisted of 387 newborns (202 males and 185 females) who failed unilaterally the first TEOAE screening test but passed screening successfully in both ears thereafter. Of these, 228 newborns passed the second screening test successfully prior to discharge, while 159 newborns passed the screening successfully 10 to 14 days following discharge. The control group consisted of 492 newborns (243 males and 249 females) who successfully passed the first TEOAE test bilaterally. This group was selected using random number generation, by choosing newborns born on the same date as each of the infants included in the study group that fulfilled the first six inclusion criteria. For both groups, the order of testing was equally distributed, with half of the newborns first tested in the right ear and half in the left ear.
The current study was approved by the institutional review board of the Sheba Medical Center (1534-14-SMC).
Hearing Screening Protocol
The screening protocol for newborns with no risk factors for hearing impairment at the Sheba Medical Center consisted of a TEOAE test which was usually conducted during the first postnatal day, excluding those infants born on weekends who were tested on the second postnatal day. Newborns who failed the first TEOAE test (in one or two ears) were rescreened with TEOAE the following day. Those who failed in-hospital screening were scheduled for a TEOAE rescreen 10 to 14 days following discharge.
TEOAE screening was conducted with an ILO292 OAE analyzer (Otodynamics Ltd, Hatfield, Hertfordshire, UK; software version 4.2) using a neonatal probe. The nonlinear Quickscreen mode of stimulation was used with a click rate of 80 presentations per second and an analysis time window of 2.5 to 12.5 ms poststimulus. Click levels varied between 74 and 87 dB peak equivalent SPL (dB pe SPL) as measured in the newborns ear canal. A high-pass filter with a cutoff at 800 Hz was also activated. The rejection level for testing was set individually at 42 to 55 dB SPL according to the noise level. Noise input levels were collected by the microphone during samples that were below the rejection level. For each ear, when the pass criteria was met after collecting at least 50 low-noise data samples (below the rejection level), the test terminated. If the pass criterion was not met at that point, the presentation of stimuli continued up to the point where the pass criterion was met.
The following pass criteria were used: (a) whole wave reproducibility ≥ 50%; (b) minimum response level ≥ 0 dB SPL; (c) presence of emissions in three frequency bands 2, 3, and 4 kHz with SNR levels ≥ 6 dB. A refer was defined when no emissions were present or when the recorded emissions did not reach one or more of the above-mentioned criteria.
Audiologists and staff members of the UNHS program tested the newborns in their crib in a quiet room in the nursery. The majority of newborns were asleep during TEOAE testing. The ear that was more easily accessible to the examiner was tested first. Whenever debris was visible in the ear canal, the probe was removed and the probe tip was changed before another attempt was performed.
Data Analysis
Preliminary analyses showed that there were no statistically significant differences in any of the research variables between the newborns in the study group who passed the second in-hospital rescreen test successfully and those who passed it after the discharge. Therefore, we collapsed the data for these two subgroups in the analyses presented later.
Pass rates
The effect of ear (right vs. left), order of testing (first tested vs. second tested ear), and gender (females vs. males) on pass rates were evaluated by means of chi-squared tests.
To eliminate the possibility that stimulus levels or noise input levels were different between the passing and failing ears and between the first and second tested ear, thus confounding pass rates, we performed a two-way between-subject analysis of variance (ANOVA) for each ear separately with stimulus level or noise input level as the dependent variables and pass or fail and order of testing as independent variables.
TEOAE response levels
Data from the initial TEOAE testing of the study group soon after birth were compared with that of the control group. Preliminary analyses yielded a significant difference in the age at testing between the control group (M = 24.97 hr, SD = 8.62) and the study group (M = 20.37 hr, SD = 7.16), t(874.4) = 8.63, p < .0001. Therefore, we included the age at testing as a covariate in the ANOVAs that compared between the study and control groups. Specifically, TEOAE response levels were evaluated for each ear separately by using a three-way between-subject analysis of covariance (ANCOVA) with response level as the dependent variable and group (study vs. control), testing order (first vs. second tested ear), and gender (female vs. male) as the independent variables.
To eliminate the possibility that stimulus levels or noise input levels were different between the study and control groups and thus may have influenced response levels, we performed a two-way between-subject ANCOVA for each ear separately with stimulus level or noise input level as the dependent variables and group and gender as independent variables. As TEOAE response levels were not significantly affected by order of testing, this variable was not included in these analyses.
TEOAE response levels were also evaluated separately in the study and control groups. In the study group, response levels in the passing ears were evaluated by using a three-way between-subject ANOVA with response level as the dependent variable and ear (right vs. left), testing order (first vs. second tested ear), and gender (female vs. male) as the independent variables. In the control group, response levels were evaluated by using a three-way ANOVA for response levels, with tested ear (right vs. left) as the within-subject independent variable and testing order and gender as the between-subject independent variables.
In ANOVAs, the Bonferroni correction was used to assure an experimentwise confidence level of 95% by dividing the overall .05 critical p level by seven (three main effects, three two-way, and one three-way interaction), with resulting comparisonwise critical p of .007.
Results
Pass Rates
Ear effect
Of a total of 387 newborns in the study group, 235 (61%) passed screening successfully only in the right ear, while 152 (39%) passed successfully only in the left ear. Thus, the proportion of newborns who successfully passed screening in the right ear was significantly higher than those who passed in the left ear, χ2(1, N = 387) = 17.80, p < .001 (Figure 1(a)).
TEOAE pass rates in the study group: (a) tested ear; (b) order of testing; and (c) interaction between tested ear and order of testing.
Order effect
The pass rate was 65% (253 newborns) in the first tested ear and 35% (134 newborns) in the second tested ear. Thus, the proportion of newborns who successfully passed screening in the first tested ear was significantly higher than the proportion who passed in the second tested ear, χ2(1, N = 387) = 36.59, p < .001 (Figure 1(b)).
Interestingly, the ear effect was dependent upon the testing order. Specifically, among 193 newborns who were first tested in the right ear, 147 (76%) passed the right ear successfully, while of the 194 newborns who were first tested in the left ear, 88 (45%) passed the right ear successfully, χ2(1, N = 387) = 38.49, p < .001 (Figure 1(c)).
Gender effect
Similar pass rates were found in males and females. Specifically, of the 202 male newborns, 126 (62%) passed successfully in the right ear and of the 185 females, 109 (59%) passed successfully in the right ear, χ2(1, N = 387) = 0.48, ns.
Of the 103 males who were first tested in the right ear, 84 (82%) passed the right ear successfully, while of the 90 females who were first tested in the right ear, 63 (70%) passed the right ear successfully. This difference was significant as found in a moderated logistic regression analysis (p = .049). That is, the effect of order on ear asymmetry tended to be more pronounced in males compared with females.
Testing conditions
Mean Stimulus Levels and Noise Input Levels (Standard Deviations) in the Failing Versus Passing Ears for the Right and Left Ears Separately.

For both right and left ears, significantly higher noise input levels were measured in the ear canals of the failing ears compared with the passing ears (Table 1). No significant differences in noise input levels were found between the first and second tested ear (p > .15).
TEOAE Response Levels
Between-group comparisons
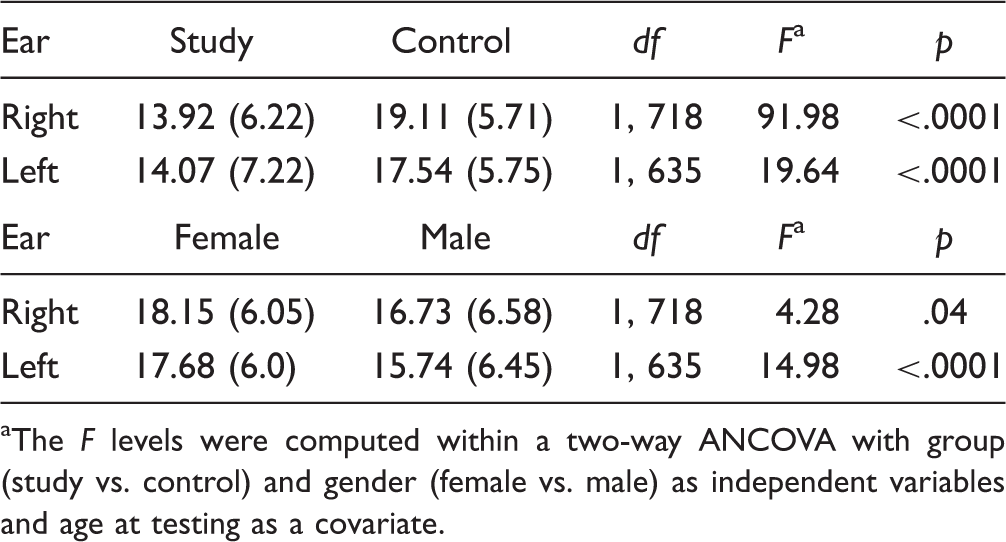
Mean TEOAE amplitudes in the study and control groups for the right and left ears are presented in Figure 2. For both ears, response levels were significantly higher in the control group compared with the study group (Table 2). Furthermore, for the left ear only, response levels were significantly higher among females compared with males (Table 2) with no significant interaction between group and gender. No significant differences were found between TEOAE response levels in the first versus the second tested ear. For both ears, stimulus levels and noise input levels were similar between the study and control groups, and between males and females (all p’s > .5), thus eliminating the possibility that these factors may have influenced TEOAE response levels.
Mean TEOAE amplitudes in the study and control groups for the right and left ears. Mean TEOAE Response Levels in dB SPL (Standard Deviations) in the Study Versus Control Groups and in Females Versus Males for the Right and Left Ears Separately. The F levels were computed within a two-way ANCOVA with group (study vs. control) and gender (female vs. male) as independent variables and age at testing as a covariate.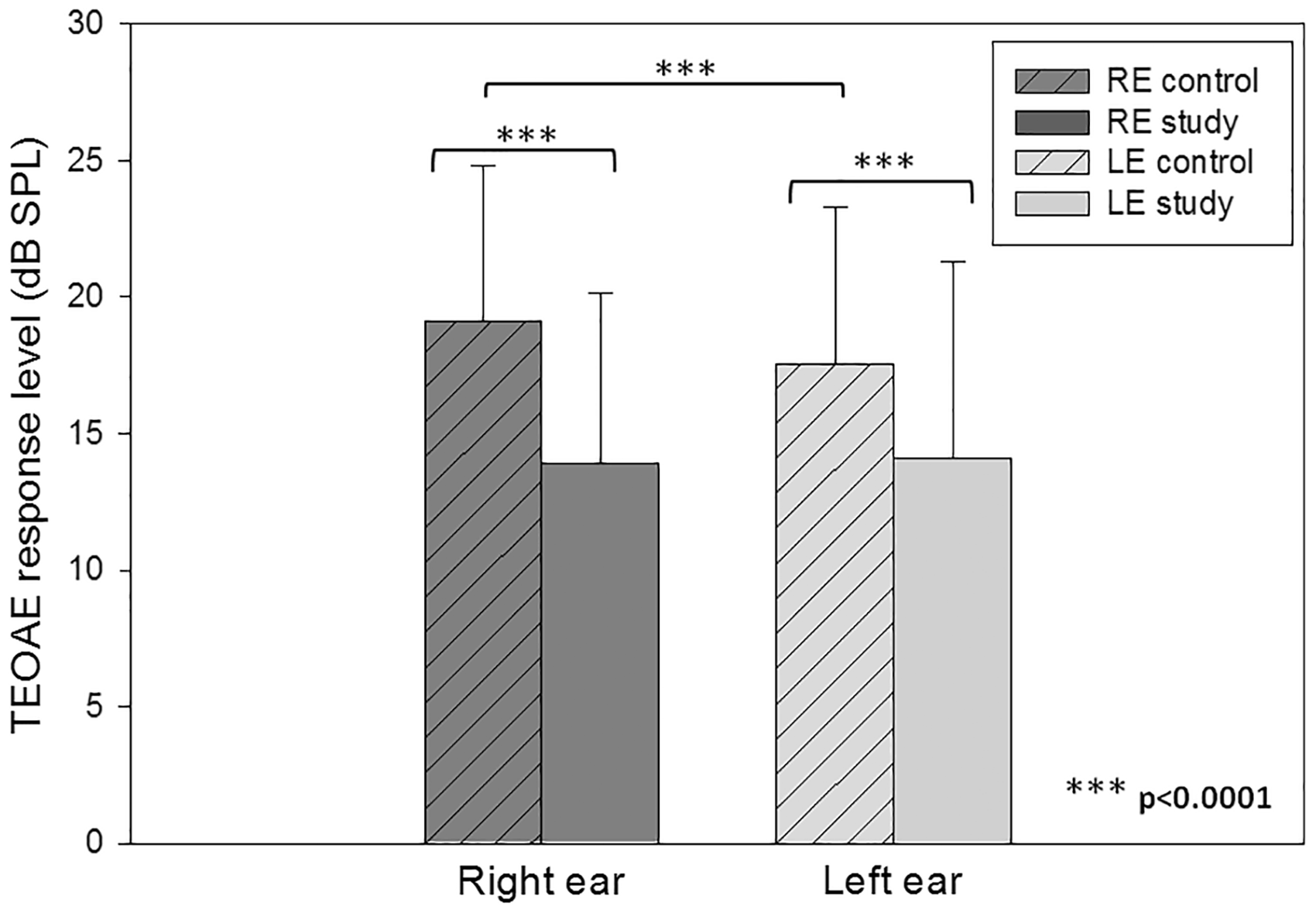
Within-group comparisons
TEOAE response levels were also evaluated in each group separately. In the study group, no significant differences were found in the passing ears between the right and left ear, between the first and second tested ear, and between females and males (all p’s > .01).
In the control group, higher response levels were found in the right ears compared with the left ears, F(1, 488) = 49.52, p < .0001 (Table 2). Furthermore, response levels were significantly greater in females (M = 19.85 dB SPL SD = 5.09, M = 18.30 dB SPL SD = 5.50, for the right and left ears, respectively) compared with males (M = 18.35 dB SPL SD = 6.20, M = 16.77 dB SPL SD = 5.91, for the right and left ears, respectively), F(1, 488) = 10.77, p = .001. These differences cannot be attributed to stimulus levels and noise input levels (for stimulus levels all p’s > .20 and for noise input levels all p’s > .07). Finally, no significant differences were found between TEOAE response levels in the first versus the second tested ear.
Discussion
The current study was designed to evaluate whether ear asymmetry exists in newborn hearing screening results. Specifically, we asked whether a right-ear advantage was evident in pass rates and TEOAE characteristics in a group of newborns who initially failed screening in one ear and passed screening successfully thereafter. TEOAE characteristics of the studied group were compared with those of a control group of newborns who passed both ears successfully. The effects of testing order and gender on screening results were also evaluated.
The first major finding was a right-ear advantage in pass rates in the study group as manifested by significantly higher pass rates in the right ear (61%) compared with the left ear (39%). This result is in accordance with the frequency of unilateral pass rates in TEOAE screening collected in our UNHS program at Sheba Medical Center during a period of 16 years. Specifically, of a total of 159,115 tested newborns, 19,554 (12.3%) failed unilaterally the first TEOAE and passed successfully TEOAE screening thereafter. Of these, 59% passed the right ear successfully whereas 41% passed screening in the left ear (unpublished data). To our knowledge, only Berninger and Westling (2011) reported data from a large cohort of over 31,000 newborns and indicated remarkably similar results to those of the current study. In their cohort, right ear pass rates amounted to 61% among newborns who failed unilaterally TEOAE screening. One confounding factor that may influence pass rates is the stimulus levels measured in the newborns ear canal. Berninger and Westling (2011) reported that the higher right ear pass rates could not be attributed to differences in stimulus levels between ears. In the present study, the possibility that stimulus levels may have influenced passing rates was ruled out, as for both right and left ears, stimulus levels were significantly higher in the failing ears compared with the passing ears.
The right-ear advantage in pass rates found in the present study is in line with the significantly 1.57 dB greater TEOAE amplitudes in the right versus left ear in the control group. This finding provides additional supporting evidence for the previously published right-ear advantage in TEOAE characteristics in newborns (Aidan et al., 1997; Berninger, 2007; Key, McPherson, Smyth, Latham, & Loscher, 1997; Newmark et al., 1997; Saitoh et al., 2006; Thornton et al., 2003).
It is well established that pass rates using TEOAE in the first day after birth are lower than those recorded in following days (Berninger & Westling, 2011; Doyle, Rodgers, Fujikawa, & Newman, 2000; Kok, van Zanten, & Brocaar, 1992; Thornton, Kimm, Kennedy, & Cafarelli-Dees, 1993). This finding has been previously explained by debris in the external ear canal resulting in partial or complete obstruction and negative middle ear pressure due to lack of ventilation (Doyle et al., 2000; Kok et al., 1992; Prieve, Hancur-Bucci, & Preston, 2009; Thornton et al., 1993). Due to the retrospective nature of the present study, data regarding external and middle ear status were not available. Nevertheless, in the case of external or middle ear problems that may affect OAEs, the greatest effect is expected in the low-frequency region (Thornton et al., 1993), while the criterion for the presence of TEOAE was restricted to the high frequencies (2–4 kHz) in the current study. Moreover, it has been shown that low pass rates were also found in the first postnatal days in neonates with clear external ear canals and normal middle ear pressure and compliance at the time of testing (Thornton et al., 1993, 2003). Additionally, Thornton et al. (2003) reported that the mean amplitude of the emissions in their newborns increased from Day 1 to 3 after birth with the largest change occurring in the high-frequency region. Thus, other factors, such as maturation and developmental changes that occur in the cochlea during the first few days of life, may come into play (Salomon, Anthonisen, Groth, & Thomsen, 1992; Thornton, 1999; Thornton et al., 1993). Following this notion, the finding of higher pass rates in the right ear soon after birth, found in the present study, may be a manifestation of earlier maturation of the right ear compared with the left ear resulting in a right-ear advantage in pass rates. The presumed earlier maturation of the right ear coincides with the well-known asymmetry at different levels of the auditory system, already apparent in the first few days of life (e.g., Bertoncini et al., 1989; Sininger & Cone-Wesson, 2006; Thornton et al., 2003).
In the present study, TEOAE response levels of the newborns who initially passed screening in one ear only were significantly lower than those who initially passed screening in both ears successfully (mean difference of 3.5–5.2 dB for the left and right ears, respectively). This may also be related to maturational and developmental changes that occur in the cochlea during the first few days of life. Similarly, Prieve et al. (2009) reported that infants who initially failed screening soon at birth and were afterward found to have normal hearing had lower TEAOE amplitudes at 1 month of age compared with those infants who initially passed screening in both ears successfully. Furthermore, in the current study, the mean age at testing of newborns who initially passed screening in both ears was higher compared with that of newborns who initially passed screening successfully in one ear only (mean difference of 4 hr). Thus, we cannot rule out the possibility that the mean age at testing may also have contributed to the difference in the response levels between the two groups.
A novel finding of the present study is the significant effect of testing order (right ear first vs. left ear first) on pass rates. Specifically, the right-ear advantage was enhanced when the first tested ear was the right ear, resulting in a 76% pass rate in the right ear compared with a pass rate of 61% in the right ear when order of testing was not taken into account. Interestingly, when the left ear was the first tested ear, pass rates were comparable in both ears (45% and 55% in the right and left ears, respectively). It should be noted that in the present study, the order of testing was equally distributed with half of the newborns first tested in the right ear and half in the left ear. Clearly, while the right-ear advantage cannot be attributed solely to the order of testing, this factor must be taken into account. To our knowledge, only Berninger and Westling (2011) dismissed the possibility that the order of testing in their study affected the higher pass rates in right ears, as 58% of their newborns were first tested in the left ear, but did not study the magnitude of the right–left asymmetry in pass rates while taking the order of testing into account. Further support to the influence of the order of testing on TEOAE responses in newborns can be found in the TEOAE amplitude data reported by Thornton et al. (2003) from a large population of newborns (over 10,000) who passed hearing screening in both ears successfully. They reported a small yet significant order effect that amounted to 0.2 dB. In the present study, no significant order effect was found on TEOAE response levels in our control group of newborns who passed both ears successfully. It may be the case that as the order effect is less prominent than the ear effect, large cohorts are required to demonstrate this effect on response levels.
Several explanations were postulated regarding the effect of order of testing. Thornton et al. (2003) dismissed the possibility that the differences in response levels were due to differences in stimulus levels between the first and second tested ears. Similarly, in the present study, no significant differences in stimulus levels were found between the first and second tested ears and thus cannot explain the higher pass rates in the first tested ear. Thornton et al. (2003) further suggested that as newborns were first tested in the more accessible ear, the effect of order of testing may be related to a higher humidity and possibly local temperature in the second tested ear. The relationship between higher local ear temperature and lower response levels is, however, not yet clear. We offer an alternative explanation that may be related to the testing procedure. In clinical practice, testing of the first ear is initiated while the baby is sleeping. Testing the second ear requires turning the newborn’s head, often resulting in awakening or restlessness, which may lead to higher failure rates in the second tested ear. This notion is in keeping with a previous report that tested the effect of different activity states of infants on TEOAE failure rates and found higher failure rates among infants who were in noisy states compared with those tested asleep or in an awake, but peaceful state (Key et al., 1997). In the present study, no significant differences were found, however, in noise input levels between the ears that were tested first and second. This assumption requires, however, further investigation of TEOAE noise levels at each frequency band between the first and second tested ear, as suggested by Keefe et al. (2008).
In the present study, the right-ear advantage was evident in pass rates in a comparable proportion of females (62%) and males (59%). TEOAE characteristics, however, differed significantly between females and males in the study and control groups. Specifically, higher response levels were found in females compared with males, regardless of tested ear and order of testing. The significantly 1.5 dB greater TEOAE amplitudes in females versus males in the control group are in agreement with previously published data consistently showing higher OAE amplitudes in female ears in newborns (Berninger, 2007; Cassidy & Ditty, 2001; Saitoh, 2006; Thornton et al., 2003). A possible explanation for gender differences is androgen exposure during prenatal development. Greater exposure to androgens in males is thought to result in a reduction of the cochlear amplifier function resulting in diminished TEOAE amplitudes (McFadden, 2009).
Conclusion
The present study provides further evidence for functional asymmetry of the auditory system at the cochlear level already apparent shortly after birth in both males and females. A right-ear advantage manifested in higher pass rates and in greater TEAOE response amplitudes. While order of testing plays a significant role in pass rates asymmetry, the innate right-ear advantage seems to be a more dominant contributor.
Footnotes
Acknowledgments
We are grateful to Chen Damari, Liat Moskowitch, Shimrit Tobiana, and Yael Weiss from the Department of Communication Disorders, Tel Aviv University for their help in data collection and preliminary data analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.