
Abstract
Self-reports of subjective hearing difficulties by people with hearing loss may be a useful complement to audiometry in hearing aid rehabilitation. To be useful, such self-reports need to be reliable. This study investigated the reliability and the validity of the Swedish Hearing Handicap Inventory for the Elderly (Screening Version; HHIE-S). Sixty-nine participants completed a questionnaire before hearing aid rehabilitation. Of these individuals, 49 completed hearing aid rehabilitation (aged between 23 and 94 years), and 41 of these 49 participants completed the questionnaire after completing the rehabilitation. The Swedish HHIE-S exhibited good internal consistency (Cronbach’s alpha coefficient of .77). The questionnaire was effective for evaluating hearing aid rehabilitation, and a statistically significant reduction in hearing difficulties was observed. The clinicians found the questionnaire easy to administer and effective in hearing aid rehabilitation. The findings from the study support the use of the HHIE-S in clinical practice.
Introduction
The Hearing Handicap Inventory for the Elderly (HHIE; Ventry & Weinstein, 1982) was translated into Swedish and psychometrically validated by Öberg, Lunner, and Andersson (2007). In 1983, a shorter version, denoted HHIE-Screening, was published for use as a screening (S) tool (Ventry & Weinstein, 1983). The primary objective of this study was to evaluate the reliability and validity of the Swedish translation of the HHIE-S, investigating the effectiveness and usability of this instrument in the hearing aid rehabilitation of a group of first-time hearing aid users.
Hearing impairment is one of the most common health problems in the elderly, and because of the aging of the population, the number of people who suffer from hearing impairment will increase in the coming decades. Consequently, a greater need for audiological rehabilitation will be apparent in the coming years. Despite hearing problems, few individuals seek hearing health care, and hearing aid uptake is still low (Chia et al., 2007; Gussekloo et al., 2003; Karlsson & Rosenhall, 1998; Popelka et al., 1998). A study that investigated the subjective hearing difficulties and hearing aid uptake of people who are 85 years old revealed that the main reasons for not acquiring a hearing aid were the interpretation that one’s hearing difficulties were not sufficiently severe and the assumption that hearing difficulties are a normal condition of older age (Meyer & Hickson, 2012; Öberg, Marcusson, Nägga, & Wressle, 2012). A primary goal for clinicians is to increase the awareness of hearing loss among elderly people. A self-report instrument can increase the awareness of one’s hearing loss and benefit the goal setting of subsequent hearing aid rehabilitation (Meyer & Hickson, 2012).
Limited correlations have been found between objectively measured hearing and self-reported hearing difficulties. Lutman (1991) and Ventry and Weinstein (1983) suggested that the hearing difficulties in elderly people are more appropriately measured via self-reports rather than inferred from audiometric data. Knudsen, Öberg, Nielsen, Naylor, and Kramer (2010) concluded that self-perceived activity limitation and participation restriction are important determinants in hearing aid rehabilitation, as these variables are able to predict the four key elements in a rehabilitation, namely seeking help, uptake, use, and satisfaction with hearing aids. In the era of evidence-based medicine, increasing demands for high-quality service can be discerned, and it is necessary to have reliable and valid instruments to evaluate the rehabilitation processes. In Sweden, there is an absence of validated self-reports that measure subjective hearing difficulties. The Swedish translation of the HHIE instrument was found to be reliable and acceptable for clinical use and was subsequently used in several studies (Öberg et al., 2007; Öberg, Andersson, Wänström, & Lunner, 2008, 2009). The clinicians and individuals found the instrument useful in the rehabilitation process but requested a questionnaire that was less time-consuming.
The short form of the HHIE, denoted the HHIE-S, has been translated to many different languages and has been used in several studies (Chang, Tseng, Chao, Hsu, & Liu, 2008; Lichtenstein, Bess, & Logan, 1988; Mulrow, Tuley, & Aguilar, 1990; Tomioka et al., 2013; Ventry & Weinstein, 1983; Vuorialho, Karinen, & Sorri, 2006; Weinstein, 1986, 1991). This questionnaire has been found to have high internal consistency reliability (Cronbach’s alpha .87–.91) and high test–retest consistency for different languages (r = .84–.98; Tomioka et al., 2013; Weinstein, 1986; Weinstein, Rasheedy, Taha, & Fatouh, 2015). Because of its reliability, validity, and brevity, the HHIE-S has been one of the most widely used instruments in English-speaking countries (Weinstein et al., 2015). This instrument has also been found to be effective in measuring the effects of different types of hearing aid rehabilitation (Chang et al., 2008; Mulrow et al., 1990; Primeau, 1997; Vuorialho et al., 2006; Weinstein, 1991). However, this instrument has never been validated for a Swedish population.
Methods
Procedure
The questionnaire and an informed consent form were sent by mail to the participants before their first visit to the hearing clinic of the University Hospital in Linköping, Sweden. The participants brought their questionnaire to their first visit to the clinic. At the visit, the clinician and the participant discussed the hearing difficulties considering the HHIE-S results, and the instrument was also used as a basis for goal setting. The participants who decided to undergo hearing aid rehabilitation completed the postrehabilitation measurement with the HHIE-S at their last visit to the clinic, that is, the visit at which they decided to keep their hearing aids.
The study was approved by the Ethics Committee in Linköping (Dnr 2014/106-31).
Participants
In total, the HHIE-S questionnaire was mailed to 134 individuals, including 74 women and 60 men with a mean age of 71.4 years (SD 15.1, range 23–94 years). Fifteen individuals did not complete the informed consent form and were excluded from the study. The remaining 119 participants (66 women and 53 men, mean age 71.1 [SD 15.6], range 23–94 years) generated 69 questionnaires that were eligible for analyses, which is a response rate of 51%. There were several reasons for the failure to complete the questionnaires. Thirty-eight individuals did not bring the questionnaire to the clinic, 2 were experienced users, and 11 never visited the clinic. Forty-nine individuals completed hearing aid rehabilitation, and 22 individuals rejected hearing aids. Of the 22 who rejected hearing aids, 15 never tried hearing aids (1 had normal hearing, 5 were not motivated, 5 experienced mild hearing difficulties, 1 had surgery, and 3 did not provide a reason), and 7 were fitted with hearing aids but returned them after some weeks (4 received no benefit from the hearing aids, 2 had health problems, and 1 provided no reason). Fifteen of the 22 who rejected hearing aids completed the HHIE-S before their visit to the clinic. This group of 15 is referred to as the nonusers group. Four individuals completed the questionnaire before the visit but chose assistive devices, and one individual had not yet completed the rehabilitation and were therefore excluded from the postrehabilitation evaluation.
Questionnaire
The HHIE-S comprises 10 items that were selected from the 25-item version of the HHIE (Ventry & Weinstein, 1982, 1983). The HHIE-S questionnaire was designed to measure hearing handicap; in this article, the outcomes of the HHIE-S are described as measurements of activity limitations and participation restrictions. The Swedish HHIE-S was constructed using the same 10 items in the English version from the translated 25-item HHIE (Öberg et al., 2007). The 10 items are divided into two subscales. Five items explore the emotional consequences (HHIE-E), and the remaining five items explore the social or situational effects (HHIE-S). There are three response options for each item, namely yes (score = 4), sometimes (2), or no (0). The scores are summed up, and higher scores indicate greater perceived activity limitation and participation restriction. Scores of 0 to 10 represent little or no activity limitations or participation restrictions, scores of 12 to 24 indicate mild to moderate limitations and restrictions, and scores of 26 to 40 indicate significant limitations and restrictions (Weinstein, 1986). When using the questionnaire to measure the effect of hearing aid rehabilitation, it has been recommended that the pre- and postrehabilitation scores should differ by at least 10 points (true change) for the hearing aid intervention efforts to be considered effective (Newman, Jacobson, Hug, Weinstein, & Malinoff, 1991; Primeau, 1997).
Statistical Analyses
The Swedish HHIE-S was tested for reliability and validity. Reliability is defined as the degree to which the measured results reflect the true results. The reliability of the HHIE-S was assessed based on internal consistency and split-half reliability. The Cronbach’s alpha coefficient was used to determine internal consistency. Split-half reliability was assessed using the Guttman formula. The 10 items were divided into two lists such that the first half of the list included items 1 to 5 (three emotional and two social items), and the second half of the list included items 6 to 10 (two emotional and three social items). Validity was assessed by floor and ceiling effects and was considered present if more than 15 % of the participants achieved the minimum or the maximum scores. Responsiveness was assessed by calculating the pre-post HHIE-S mean scores for first-time hearing aid users and was measured with dependent t test and measurements of effect sizes (ESs). ESs were measured using Cohen’s d (Cohen, 1988). The differences between the pre- and posttreatment means were divided by the standard deviation from the pretreatment measurements. An ES of 0.2 is considered small, whereas ESs of 0.5 and 0.8 are considered moderate and high, respectively (Cohen, 1988). Parametric tests were used because the data were normally distributed, as determined using the Kolmogorov–Smirnov test for normality. Categorical data were analyzed with the chi-square test.
Pearson’s product moment correlation coefficient was used to measure the associations of the pre–post HHIE-S mean scores and of the HHIE-S mean scores with the pure-tone averages (PTA) at 0.5, 1, 2, and 4 kHz in the better ear. An independent t test was used to investigate the difference in the HHIE-S scores between the users and nonusers. The data were analyzed using the STATISTICA software package (Statsoft, 2015, version 12), and results with p values < .05 were considered statistically significant.
Results
Reliability and Validity
The internal consistency values revealed a Cronbach’s alpha of .77, and the item-total correlations ranged from .22 to .60. The split-half value, using the Guttman formula, was .75. One participant recorded the maximum score before (1.5%) and four participants recorded the minimum score (10%) after hearing aid rehabilitation, which did not exceed the criteria for floor or ceiling effects.
Mean HHIE-S Scores of the Users and Nonusers
Demographic Data, Initial HHIE-S Scores, and p Values Between Hearing Aid Users and Nonusers.

Note. HHIE-S = Hearing Handicap Inventory for the Elderly (Screening Version); PTA = pure-tone average.
No perceived activity limitations and participation restrictions.
Mild to moderate perceived activity limitations and participation restrictions.
Significant perceived activity limitations and participation restrictions.
Responsiveness
Means, SDs, p Values, and Effect Sizes (ES) for Pre- and Postrehabilitation HHIE-S Scores.

Note. HHIE-S = Hearing Handicap Inventory for the Elderly (Screening Version); CI = confidence interval.
In this study, 69% of the participants with initial scores above 10 demonstrated a decrease of at least 10 points. Two participants were excluded because their initial scores were less than 10 points, and of the remaining participants, 56% (23 of 41) of the participants showed a total score of 10 or below postrehabilitation.
A correlation was performed to further investigate whether there was a relation between the initial HHIE-S mean score and the PTA in the better ear and a statistically significant correlation was found (r = .36, p < .05). No statistically significant correlation was found between the HHIE-S improvement scores and the PTA (r = .06). Figure 1 shows a scatterplot with the HHIE-S improvements as a function of the PTA hearing threshold levels (0.5, 1, 2, and 4 kHz) in the better ear. This scatterplot shows that several participants with mild hearing losses indicated significant improvements. Sixty-three percent of the participants with PTA in their better ears between 10 and 30 dB, 85% of those with PTA between 31 and 40 dB, and 55% of those with PTA between 41 and 50 dB demonstrated a change by at least 10 points.
Scatterplot with HHIE-S improvements as a function of PTA hearing threshold levels (0.5, 1, 2, and 4 kHz) in the better ear (r = .06).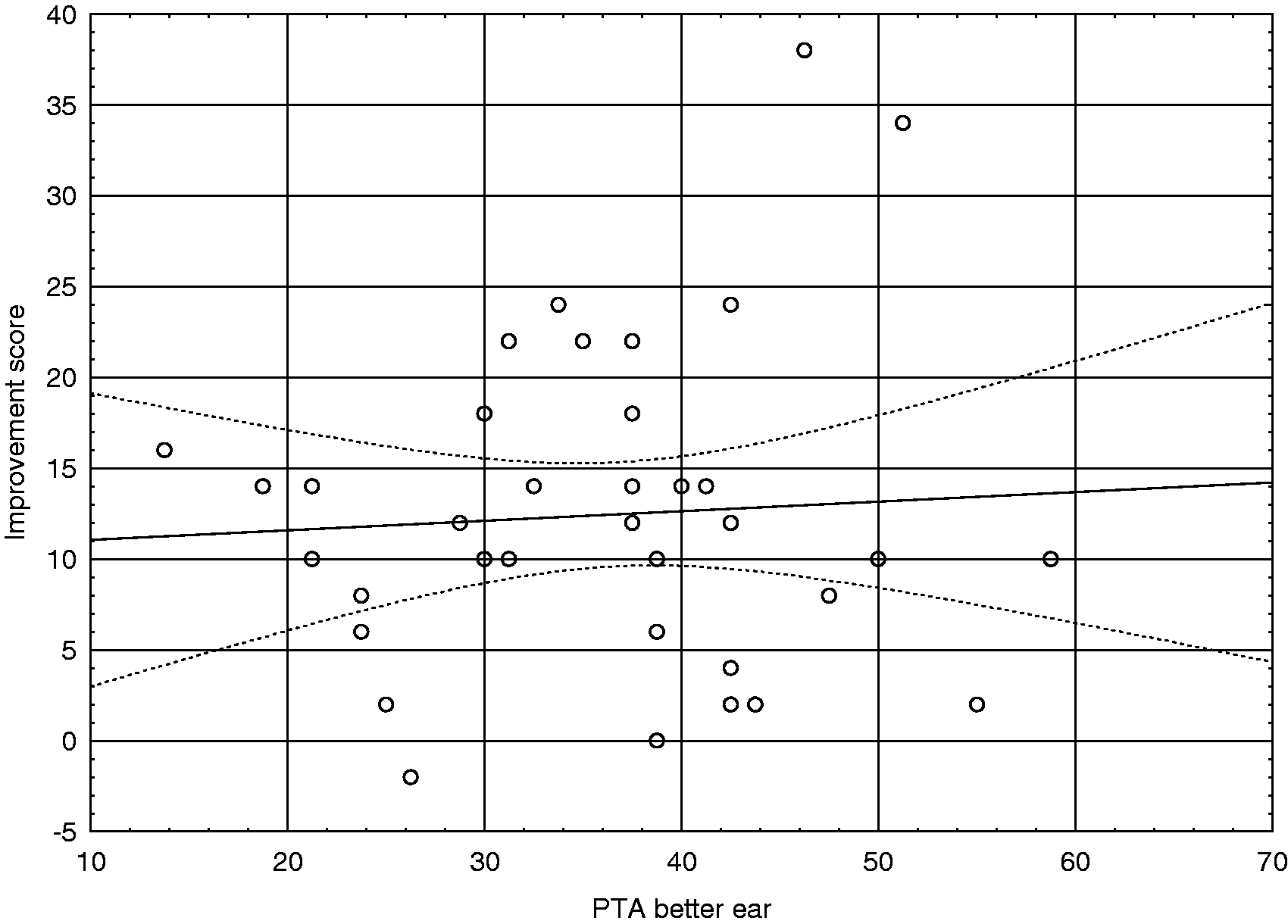
Discussion
This study showed that the Swedish HHIE-S is a reliable instrument. The questionnaire was found to be an effective and valid instrument for evaluating hearing aid rehabilitation. The clinicians found the HHIE-S easy to administer and effective because it facilitated the initial and subsequent goal setting of the rehabilitation. One objective of this study was to evaluate the reliability and validity of the Swedish translation of the HHIE-S. The reliability of the HHIE-S and the internal consistency were acceptable (Clark-Carter, 2004), although Cronbach’s alpha and the split-half value in the present study were somewhat weaker than those obtained in other studies (Ventry & Weinstein, 1983 [.87]; Tomioka et al., 2013 [.91]). For the split-half value, Weinstein (1986) and Tomioka et al. (2013) found values of .87 and .90, respectively. Another objective was to investigate the effect and usability of this instrument in the hearing aid rehabilitation of a group of first-time hearing aid users.
The HHIE-S questionnaire was found to be a valid instrument to measure the effects of hearing aid rehabilitation. In the present study, the ES of the HHIE-S total was 1.38. This finding is consistent with other studies that have used the HHIE-S before and after rehabilitation and found ES of 1.24 to 2.46 (Chang et al., 2008; Primeau, 1997; Weinstein, 1991). Newman et al. (1991) suggested that for clinical purposes, an individual’s pre- and postrehabilitation scores should differ by at least 10 points for a hearing aid intervention to be considered effective. However, this criterion can only be used when the subject exhibits over 10 points on the prerehabilitation assessment. In this study, 69% of the participants demonstrated a change of 10 points or more. In the study by Newman et al. (1991), 92% of the participants exhibited a change of 10 points, and in the study by Primeau (1997), 73% of the adults and 81% of the older adults exceeded the 95% confidence interval when they were evaluated 6 weeks after hearing aid fitting. One reason for the somewhat lower rates of the participants who reach a change of 10 points in the present study may be because 25% of the participants had initial scores of 11 to 14. It is unrealistic to believe that the majority of people with hearing difficulties would have total scores of 0 to 4 points postrehabilitation because scores of 0 to 10 points indicate no hearing difficulties (Weinstein, 1986). In evaluating the effects of hearing aid rehabilitation, another way to consider the effect of the rehabilitation can be to measure the number of participants who fall 10 points postrehabilitation. It could be argued that it is normal to have scores of up to 10 points postrehabilitation because not all hearing difficulties can be solved with hearing aids. More than half of the participants in this study had postrehabilitation scores below 10, which indicates small residual hearing difficulties. When using the HHIE-S in hearing aid rehabilitation in the clinic, one goal can be to reach a change of 10 points. This goal would be relevant if the participants have initial scores above 20 points.
No differences were found, in this study, in the prerehabilitation scores between the users and nonusers, which verifies that activity limitations and participation restrictions are not the only factors associated with hearing aid uptake (Knudsen et al., 2010).
A weak correlation was found between the initial HHIE-S mean scores and the PTA, and no correlation was found between the improvements in the scores and the PTA in the present study. Several studies have investigated the relationship between hearing aid rehabilitation satisfaction and the PTA and come to the same conclusion as the present study (Bertoli, Bodmer, & Probst, 2010; Knudsen et al., 2010; Newman et al., 1991; Öberg et al., 2007; Wong, Hickson, & McPherson, 2003). In the present study, several participants with mild hearing loss showed significant improvements, and similar results have been reported in other studies (Kochkin, 1997; Newman et al., 1991). These findings support the idea that the participants with audiometrically mild hearing loss experience difficulties in many listening situations (e.g., listening in restaurants, concerts, and movies) that often cannot be predicted from audiograms (Newman et al., 1991), but hearing aid rehabilitation can be rather successful in these cases (Kochkin, 1997; Newman et al., 1991). This observation indicates that it is important to use self-reports.
The clinician found the HHIE-S to be effective. The initial HHIE-S facilitated goal setting, and the clinician noted that the questionnaire made more participants better aware of their hearing losses and difficulties. At the last visit, the pre- and postrehabilitation HHIE-S scores could easily be compared, and the results were helpful for identifying the participants who required additional rehabilitation.
One limitation of this study is the low response rate. Many participants forgot to bring either the informed consent form or both the consent form and the questionnaire to their first visit at the clinic. This approach was chosen to give the participants the opportunity to complete the questionnaire undistracted at home and to give them time to reflect on the items. Another approach could be to ask the participants to complete the questionnaire and informed consent form while sitting in the waiting room.
Conclusion
This study revealed that the Swedish HHIE-S is a reliable instrument. Specifically, the questionnaire was found to be an effective instrument for evaluating hearing aid rehabilitation. In addition, the clinicians found the HHIE-S easy to administer and useful in hearing aid rehabilitation.
Footnotes
Acknowledgments
We thank all of the clinicians in the audiology clinic at Linköping University Hospital who cared for the participants in their hearing aid rehabilitation.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Östergötland County Council Research Foundation.