
Abstract
Streptococcus pneumoniae (S. Pneumoniae) is a common cause of bacterial meningitis in the pediatric population, but rarely causes complications such as encephalitis, abscess, and seizures with the prompt initiation of proper antimicrobial therapy. In this report, we present a rare and severe case of S. Pneumoniae meningoencephalitis in a full term 6-month-old which progressed to multiple cerebral and cerebellar infarcts with concomitant cerebellar tonsillar herniation and hypercarbic respiratory failure requiring intubation and mechanical ventilation despite early initiation of antibiotics. Given the patient's clinical status and poor neurological prognosis, the family eventually opted for palliative extubation.
Introduction
S. Pneumoniae is a leading cause of pneumonia, otitis media, sinusitis, and other diseases, especially in the pediatric population. 1 It is spread via droplet transmission, by means of coughing, sneezing or close contact with an infected person. It is an opportunistic, gram-positive pathogen which can cause both noninvasive infections, limited to upper respiratory tract infections, as well as invasive pneumococcal disease, which can be devastating to the host. In invasive pneumococcal disease, S. Pneumoniae can advance via local spread with subsequent pneumonia, meningitis, and encephalitis or by infiltration of the blood stream leading to bacteremia and sepsis. Colonization is highly dependent on the effective evasion that S. Pneumoniae has on the immune system of its host. 2 If the pathogen can access the intravascular space and furthermore invade the blood brain barrier, it then replicates in the subarachnoid space, which starts a cascade of neurological consequences for the host. 3
In some cases, S. Pneumoniae infection can lead to rarer complications such as intracranial vasculopathy, disseminated intravascular coagulation, and intracranial infarction. It remains the most common cause of bacterial meningitis in children between 1 to 12 months of age and in adults of any age. Across the United States, the incidence of pneumococcal meningitis is 0.3 per 100,000 people. In Europe, 22.5% of bacterial meningitis in children is due to S. Pneumoniae. 4 Among those with all causes of bacterial meningitis, the incidence of stroke ranges from 24%to 43%, and children with S. Pneumoniae meningitis specifically have rates of stroke as high as 45%. 5 These stroke patients are much more likely to have seizures at presentation. 6 The pathophysiology by which S. Pneumoniae causes intracranial thrombosis is largely unknown, but some studies show that this is a result of bacterial induced inflammatory cascade, with neutrophil migration across the blood brain barrier and subsequent cytokine and chemokine release. This persistent inflammatory state results in cerebral edema, increased intracranial pressure, decreased cerebral perfusion, vasculitis, and vasospasm.3,7
Here we present a severe case of S. Pneumoniae causing meningoencephalitis, intracranial infarction and eventual death.
Case
A previously healthy 6-month-old presented to the hospital with altered mental status and whole body shaking, right side more than left, with right gaze deviation after a week of upper respiratory symptoms. The patient was up to date with his 4-month vaccines, including 2 doses of the pneumococcal conjugate vaccine, but had not yet received his 6-month vaccinations. His symptoms began 5 days prior to his initial presentation with fever and watery diarrhea. His mother administered acetaminophen and ibuprofen for symptom relief for 3 days prior to initial presentation, and she brought him to an outside hospital emergency department, when he began to have abnormal eye movements and bilateral shaking movements. He was observed overnight, diagnosed with simple febrile seizure, and sent home the following day. At home, his mother continued to treat with acetaminophen and ibuprofen, but he remained irritable and had multiple episodes of non-bloody, non-bilious emesis after meals with continued watery diarrhea for the next day and a half. The night prior to repeat presentation, the patient became progressively more somnolent and developed new right sided arm and leg shaking, accompanied by continuous right gaze deviation, which prompted his repeat arrival to the emergency room.
His vital signs were significant for hypothermic temperature of 95.4° F (35.2°C) and heart rate of 166 beats per minute. Respiratory rate, blood pressure, and oxygen saturation were within normal limits. Physical examination was notable for a somnolent infant responsive only to painful stimuli, not in acute distress. Anterior fontanelle was bulging and pulsatile, which mildly improved with fluid resuscitation. Lungs were clear to auscultation bilaterally, with no evidence of increased work of breathing and heart sounds were regular without murmur. Neurological examination revealed equal and reactive sluggish pupils, along with bilateral rightward gaze deviation with alternating nystagmus. Face was grossly symmetric with no visible cranial nerve deficits. Patient was noted to have continuous rhythmic twitching of his right wrist, fingers, and leg with right knee flexion posturing. Reflexes were 2+ throughout.
Abnormalities in laboratory studies at presentation included a white blood cell count (WBC) of 2.63 /nL, a platelet count of 42 /nL, sodium of 131 mmol/L, potassium of 5.4 mmol/L, alkaline phosphatase of 277 U/L, aspartate aminotransferase of 399 U/L, alanine aminotransferase of 110 U/L, INR 13.6 s, aPTT 47.7 s, fibrinogen 190 mg/dL. Venous blood gas revealed a pH of 7.10, with a carbon dioxide component of 67, bicarbonate of 21, and a lactic acid of 4.7 mmol/L. Blood and cerebrospinal fluid culture studies were sent, and the patient was immediately administered ceftriaxone 100mg/kg, vancomycin 20mg/kg, levetiracetam 60mg/kg, and lorazepam 0.5 mg, along with three consecutive rounds of fluid resuscitation (20 ml/kg each). Chest radiography (CXR) was negative for any infiltrates or masses and non-contrast head CT was normal. The patient was immediately admitted to the Pediatric intensive care unit (PICU) in the setting of acute toxic metabolic encephalopathy.
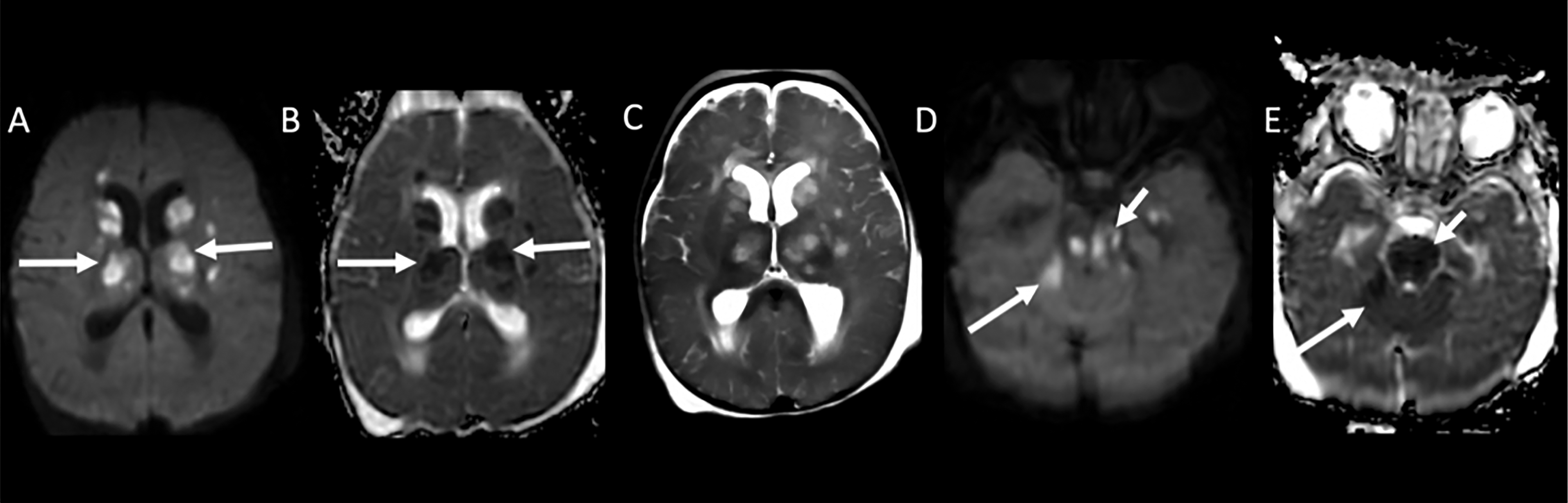
On the second day of hospitalization, brain MRI with and without contrast revealed multiple acute infarcts; with minimal enhancement in the bilateral basal ganglia, thalami, and brainstem; and prominent leptomeningeal enhancement in the basal cisterns, concerning for intracranial infection (Figure 1). Both CSF and blood culture bottles grew S. Pneumoniae later that day, and so he continued to receive treatment with ceftriaxone and vancomycin. Initial EEG demonstrated left sided cerebral dysfunction and epileptic discharges, though no active seizure activity was noted.

Multi-planar multi-sequential MRI Brain with and without contrast. Diffusion Weighted Image (DWI, A and C) and Apparent Diffusion Coefficient sequences (ADC, B and D) demonstrate multiple areas of restricted diffusion predominantly in the bilateral basal ganglia and thalami (arrows on A and B) and in the brainstem (arrows on C and D), consistent with acute infarcts. Prominent leptomeningeal enhancement in the basal cisterns on post-contrast T1WI (arrow E).
Three days later, the patient was noted to have asymmetric pupils and an urgently performed fast T2 brain MRI demonstrated dilation of the lateral ventricles and increased acute infarcts in the bilateral cerebral hemispheres, gangliocapsular regions, thalami, upper brainstem, and cerebellar regions (Figure 2). Soon after, the patient developed hypercarbic respiratory failure, prompting intubation. EEG at this time showed numerous multifocal and secondarily generalized subclinical seizures, and the patient was given a phenobarbital loading dose of 20mg/kg, started on phenobarbital 2.5 mg/kg twice daily and started on a continuous infusion of midazolam at 0.1 mg/kg/hr. Repeat brain MRI three days later demonstrated new large bilateral cerebellar infarctions causing mass effect on the fourth ventricle and resulting in hydrocephalus and cerebellar tonsillar herniation. Additionally, progression of the meningitis was observed with extension of parenchymal, leptomeningeal, and pachymeningeal enhancement (Figure 3). Given the patient's clinical status and poor neurological prognosis, the family opted for palliative extubation.
Follow up Fast T2 MRI Brain without contrast. DWI (A) and ADC (B) through basal ganglia demonstrate increased areas of restricted diffusion in the bilateral basal ganglia and thalami (arrows), consistent with increasing acute infarcts. There is corresponding edema on TWI (C). DWI (C) and ADC (D) through brainstem demonstrate Increasing infarcts in the brainstem (short arrows on D and E) and new right cerebellar infarct (long arrows on D and E).

Follow up multi-planar, multi-sequence MRI Brain with and without contrast. DWI (A and B) and ADC images (C) demonstrate infarcts in the bilateral basal ganglia and thalami (A) and new large acute infarcts in the bilateral cerebellar hemispheres (arrows on B and C) with significant mass effect. Axial T1 WI post-contrast images through the basal ganglia (D) and through the basal cisterns (E) show extensive areas of parenchymal, leptomeningeal and pachymeningeal enhancement (arrows) and obstructive hydrocephalus (asterisks).
Discussion
Pneumococcal meningitis is a serious disease that can lead to shock, respiratory failure, seizures, and intracranial infarction in the acute phase, as well as hearing loss, motor deficits, and death in the long term. 8 There are high rates of mortality and neurologic morbidity, and rapid treatment is essential. In children of any age, the most common infectious agents which can result in bacterial meningitis and neurological sequelae such as seizures, cerebral infarction, and death include Neisseria meningitidis (N. meningitidis) and Haemophilus influenzae type b (Hib), though S. pneumoniae meningitis has a much higher risk of causing neurological sequela when compared to N. meningitidis and Hib (75% vs 25% vs 20%). Escherichia coli, Group B Streptococcus, and Listeria monocytogenes are more often found in preterm neonates and infants < 3 months of age. These organisms should always be kept in mind when choosing empiric treatment for and pediatric patients. 8
It is important to note that in a study of pediatric bacterial meningitis, 60% of patients who experienced a stroke developed a fever >48 h prior to presentation. Other risk factors associated with intracranial infarction in bacterial meningitis include seizures at presentation, lower level of consciousness, and increased inflammatory markers. 5 Our patient developed a tragic complication of invasive pneumococcal disease, and his early risk factors were initially overlooked by the outside hospital. Given the duration of his symptoms, presentation, and age, even a rudimentary infectious workup was warranted. This delay resulted in a catastrophic clinical outcome. The presence of multiple infarcts on MRI performed the day after admission reflects the severity to which the disease had progressed in the days after his initial discharge from first the emergency department. It is also imperative to highlight that the patient had 5 days of fever and emesis before seeking medical services, further prolonging investigation and intervention. This not only emphasizes the importance of parental education, especially during the infant period, but also the need for thorough investigation and return precautions from emergency services.
Furthermore, after the diagnosis was made, the lack of corticosteroid use in this patient could have negatively impacted prognosis, as they have been found to reduce neurological sequela (17.9 vs 21.6%) in patients with bacterial meningitis and reduce mortality (29.9% vs 36%) in patients specifically with S. Pneumoniae compared to those without steroid treatment. 9 Corticosteroid use has been shown to successfully decrease inflammation in the subarachnoid space and administration within 12 h of antibiotic initiation is essential. 8
While the advent of vaccines has greatly diminished the rates of pneumococcal disease, there are still rare cases, like this one, in which timely medical investigation and attention could have positively impacted overall clinical prognosis. Strict return precautions, which were unfortunately not provided at the outside hospital emergency department, should be provided to every parent and patient to mitigate the consequences that occur from lack of timely treatment. Together with existing literature, this case demonstrates the utility of maintaining a low threshold for further investigation in children, particularly infants, accompanied by seizure or focal neurologic symptoms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.