
Abstract
Cobb syndrome is a rare neurocutaneous disease characterized by multiple spinal vascular anomalies and vascular skin lesions affecting the corresponding dermatome. We present a case of a 12-year-old boy with history of spinal arteriovenous malformation (AVM) extending from T4-T5 status post partial embolization 3 years ago and hyperpigmented patch overlying his thoracic back region presenting with 2 days of back pain and lower extremity numbness and weakness. He had multiple Type III AVMs within the spinal and paraspinal tissues involving the T4-T7 vertebral elements, most extensively T4 and T5. The largest aneurysm located at the confluence of the main AVM nidus was a 4 mm anterior spinal artery aneurysm, which was embolized with partial embolization of the main AVM nidus, resulting in complete aneurysm occlusion. This report provides valuable insight on the natural history, recurrence risk, and treatment options of Cobb syndrome to aid in early diagnosis and improve outcomes.
Introduction
Cobb syndrome is a rare neurocutaneous disease characterized by the presence of multiple spinal vascular anomalies and vascular skin lesions affecting the corresponding dermatome. Cutaneous vascular lesions, which are present at birth and persist, range from macular port wine stains to raised lesions like angiomas at a particular dermatomal level. 1 The deep vascular lesions occurring at the same level can be intramedullary, intraspinal extramedullary, vertebral or extraspinal and can be high flow (arteriovenous malformations (AVM)) or low flow (angiomas). 2 Cobb syndrome is typically diagnosed in late childhood following the onset of neurological symptoms. We present a case of a 12-year-old boy who presented with sudden onset paraparesis and numbness along with urinary retention found to have multiple AVMs at the level of a hyperpigmented skin lesion.
Case Presentation
The patient is a 12-year-old boy with a history of spinal arteriovenous malformation extending from T4-T5 status post partial embolization without complete obliteration 3 years ago. Since that time, patient did not have surveillance imaging. He presented with 2 days of midback pain, bilateral lower extremity numbness and weakness, and difficulty urinating requiring foley insertion. On neurological exam, the patient had normal strength, sensation, and reflexes in his upper extremities. In his lower extremities, patient's hip flexion/extension and knee flexion/extension were 4+/5 on the left and 4-/5 on the right. Dorsiflexion and plantarflexion were 0/5 on the left and 2/5 on the right. Sensation was decreased to all modalities below the level of the T4 dermatome. Patellar reflexes were 3 + bilaterally and Achilles reflexes were 4 + bilaterally, with sustained clonus on the left. The patient was noted to have a large patch of port wine stain lesion overlying his thoracic spinal region present since birth (Figure 1). Spinal MRI with and without contrast was obtained which showed an intramedullary T2 hypointense signal at T3-T4 with adjacent central hyperintensity within the cord extending to T6 inferiorly with associated adjacent cord edema indicating rupture (Figure 2).

Large patch of port wine stain lesion overlying the thoracic spinal region of a 12-year-old male patient with Cobb syndrome present since birth.

T2 weighted spinal magnetic resonance imaging (MRI) with and without contrast obtained in a 12-year-old male patient with Cobb syndrome showing an intramedullary T2 hypointense signal at T3-T4 with adjacent central hyperintensity within the cord extending to T6 inferiorly with associated adjacent cord edema/syrinx.
The patient was started on high dose IV steroids and then taken to the operating room for a spinal digital subtraction angiography (DSA) done by a vascular neurosurgeon. Multiple Type III AVMs within the spinal and paraspinal tissues were found involving T4-T7 vertebral elements, most extensively T4 and T5 (Figure 3). There were also several foci of arteriovenous shunting from T2-T5 most extensively involving the T3 and T4 segments. The main nidus, measuring approximately 1.2 cm, was predominantly supplied by the anterior spinal artery. Contribution to the anterior spinal axis was noted from right and left costocervical trunks via the C8 radiculomedullary arteries, right T5 segment between the medullary artery and right T8-T9 and left T10 radiculomedullary arteries. The largest supply involved the right T5 segmental artery.
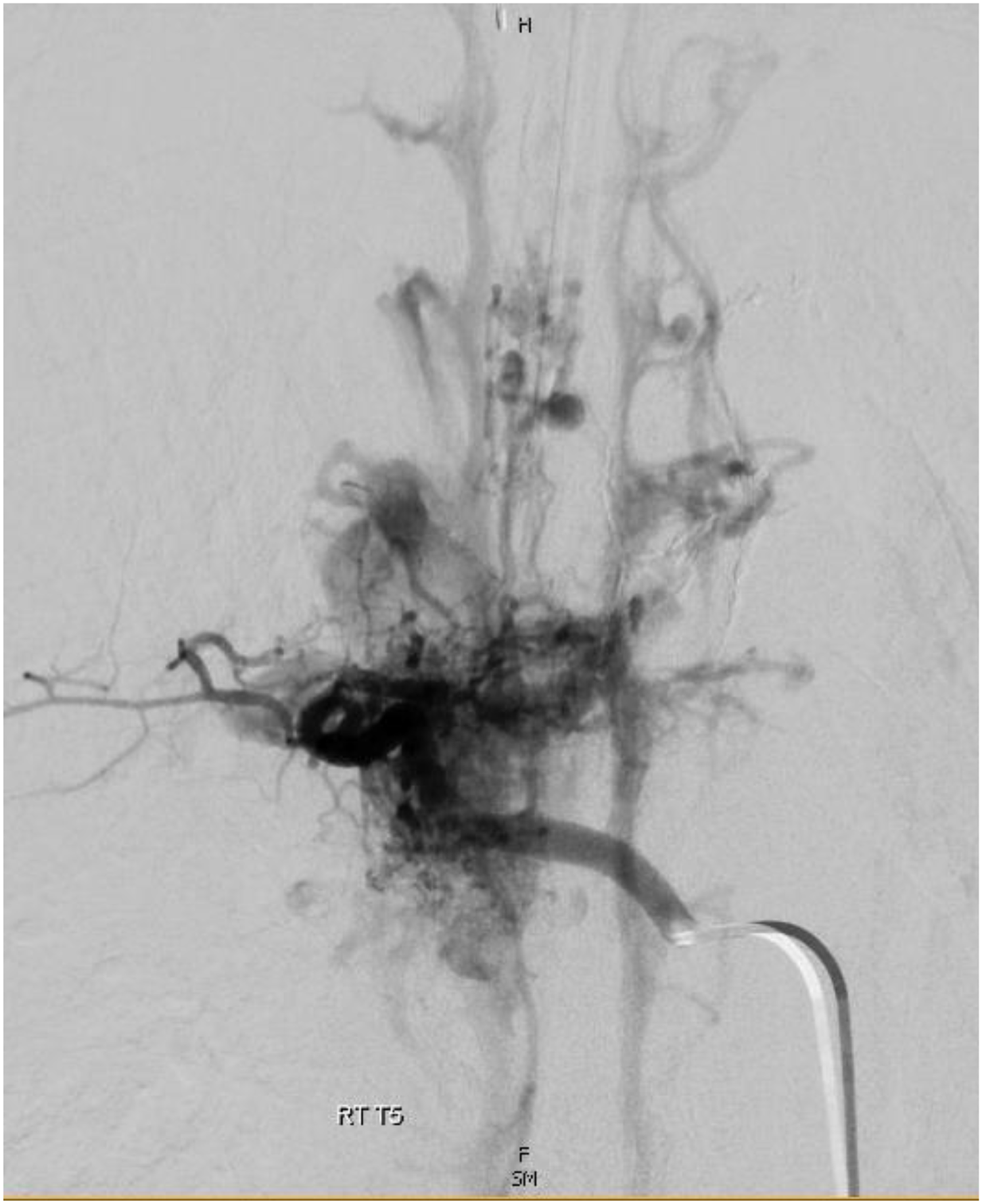
Pre-operative digital subtraction angiography (DSA) in a 12-year-old male patient with Cobb syndrome showing multiple arteriovenous malformations (AVMs) within the spinal and paraspinal tissues involving T4-T7 vertebral elements, most extensively at T4 and T5.
A 4 mm anterior spinal artery aneurysm was located at the confluence of the right radiculomedullary artery and the ascending and descending limbs of the anterior spinal artery. The aneurysm presumably reflected the site of recent rupture and was located maximally 1 cm caudal to the main AVM nidus. A second intranidal aneurysm measuring 3 mm was also noted. Venous drainage of the nidus was directed into the anterior spinal vein.
A more proximal and more direct limb associated with the anterior spinal aneurysm was chosen for embolization, achieving a flow control position. Under live subtraction guidance, the aneurysm was embolized with n-BCA: Lipidol 1:1.5 dilution liquid embolic, achieving excellent permeation of the aneurysm and its inflow pedicles, as well as partial permeation of the nidus. Post-embolization imaging demonstrated preservation of anterior spinal artery axis cranial and caudal to the embolized segment, with no residual opacification of the aneurysm, the main AVM nidus, or its intranidal aneurysm. (Figure 4).

Digital subtraction angiography (DSA) in a 12-year-old male patient with Cobb syndrome after embolization of a 4 mm anterior spinal artery aneurysm located at the confluence of the main arteriovenous malformation (AVM) nidus. Partial embolization of the main AVM nidus was also achieved, resulting in complete aneurysm occlusion and no identifiable residual inflow into the main nidus or its 3 mm intranidal aneurysm.
Postoperative physical exam was similar to preoperative exam. The patient finished an oral steroid taper and was discharged to a rehabilitation facility. On one month follow up, patient was noted to have improved lower extremity strength (knee extension was 3/5 on the right and 2/5 on the left and ankle dorsiflexion/plantarflexion was 2/5 on the right and 1/5 on the left) and able to urinate spontaneously. The patient has six month follow up scheduled with vascular neurosurgery, during which a spinal DSA will be performed for monitoring.
Discussion
A diverse range of presentations have been described for Cobb syndrome. It is a genetic, non-inherited condition thought to be due to a sporadic mutation at an early stage of embryogenesis. This mutation causes multiple vascular malformations to occur in the spine, muscles, skeleton, soft tissues, and skin. Spinal AVMs are divided into four subtypes based on the classic classification system, and Cobb syndrome is typically associated with Type III AVMs (Table 1).1–3 Though the disease is present at birth, clinical manifestations are usually not seen until late childhood. 2 Symptoms can range from monoparesis to sudden onset spastic quadriplegia. Bladder and bowel involvement is common but occurs later as the disease progresses. Onset of symptoms can be gradual over weeks to years, but sudden onset with rapid progression has been reported. 1
Four Subtypes for AVM Based on Classic Classification System.

This case highlights that any skin lesion associated with a spinal vascular lesion at the same level and acute onset neurological deficits should raise suspicion for the syndrome. While this patient had a previously diagnosed AVM at the level of a hyperpigmented skin patch years prior, the idea of Cobb syndrome was not brought up until his current presentation. The patient's symptoms were more severe in the current presentation compared to prior when patient had mild back pain and lower extremity numbness.
There are several hypotheses regarding the cause of neurological manifestations of Cobb syndrome, including blood steal syndrome producing cord ischemia, cord compression by spinal AVM, venous hypertension, and subarachnoid hemorrhage. 4 Given the presence of multiple AVMs and a ruptured aneurysm in the current patient, it is difficult to say which of these pathologies contributed most to his presentation. Computed tomography (CT) and magnetic resonance imaging (MRI) are useful modalities to assess vascular lesions, but final diagnosis depends on angiography. 5
The optimal management remains variable. Treatment options range from palliation without intervention to surgical resection and endovascular embolization. These options are usually combined with steroid therapy, which has been shown to have positive outcomes in reducing the number and extent of embolizations. 6 The goal of treatment is to effectively delay progression of symptoms by reducing mass effect, venous hypertension, and vascular steal. 4 Physical therapy is also utilized to improve the extent of neurological deficits.
As type III spinal AVMs are often extensive and at multiple levels, curative therapy may be hard to achieve and recurrence is common. AVMs with a nidus are more likely to rupture causing hemorrhage, and recurrence rate of hemorrhage is around 50%. Treatments are usually palliative measures to prevent further hemorrhage. Long-term follow up over 5 years after endovascular treatment has shown that approximately 40% of patients deteriorate, 30% improve, and 30% remain stable. 7
The course of this syndrome is unpredictable, making prognosis difficult. However, early diagnosis, treatment, and follow up at least yearly with spinal MRI and/or DSA has been shown to be beneficial in improving outcomes. 8 Involvement of a multi-disciplinary team consisting of Neurologists, Neurosurgeons, and Interventional Neuroradiology Specialists is crucial to manage the patient. 5
Footnotes
Author Contributions
Garcia, M:contributed to conception and design Select item drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Mulchan, N: contributed to conception and design Select item drafted manuscript critically revised manuscript gave final approvalagrees to be accountable for all aspects of work ensuring integrity and accuracy. Wells, J: contributed to conception and design Select item drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.