
Abstract
Background:
Total shoulder arthroplasty (TSA) is challenging in weight lifters due to their relatively young age and desire for sport continuation.
Purpose/Hypothesis:
This study aimed to assess return to weight lifting and long-term outcomes after inlay-TSA (iTSA). It was hypothesized that iTSA would lead to high return to sport and performance.
Study Design:
Case series; Level of evidence, 4.
Methods:
This study included weight lifters (<65 years of age) with advanced osteoarthritis (OA) treated with iTSA (2011-2023). Radiographic analysis established glenoid morphology (Walch classification), OA grade (Samilson-Prieto classification system), humeral head centralization (Walch index; contact point ratio), and periprosthetic loosening (modified Lazarus grading system; clinically relevant radiolucency: complete line >2 mm). The primary outcome was return to sport. Secondary outcomes included weight lifting frequency, Western Ontario Osteoarthritis of the Shoulder Index (WOOS) percentage, American Shoulder and Elbow Surgeons (ASES) score, visual analog scale (VAS) pain score, satisfaction score, and range of motion (ROM). One-repetition maximum (1RM) and cumulative weight total (multiplying sets, repetitions, and weight lifted) were compared preoperatively and at the last follow-up on bench press (BP), overhead strict press (OSP; single arm and barbell), and military press (MP). The Wilcoxon rank-sum and paired t tests were used to compare preoperative and last follow-up functional and radiographic outcomes.
Results:
Eighteen male weight lifters (3 competitive, 15 recreational; 24 shoulders) with a mean age of 54.6 ± 6.8 years were included. Prearthritic weekly lifting frequency included ≥4 sessions (n = 16) or 2 to 3 sessions (n = 8). The mean follow-up was 83.5 ± 31.6 months. All athletes returned to weight lifting without restrictions at a median of 8.5 months (IQR, 6-24 months). Overall, 78% (n = 14) returned to the same or higher activity. The Cumulative lifetime maximum BP weight (preoperative: 6822.0 ± 2951.3 lb; postoperative: 5498.0 ± 2534.2 lb) was not significantly different (P = .177). Athletes returned to 73.4% ± 20.5% of their 1RM single-arm OSP (BP: 57.3% ± 21.8%; MP: 55.8% ± 23.3%). The final mean patient-reported outcomes were 81.7% ± 21.0% for WOOS percentage, 86.7 ± 16.9 for ASES score, 1.0 ± 2 for VAS pain score, and 8.8 ± 1.5 for satisfaction score. Preoperative ROM significantly improved in forward elevation (from 117.6°± 34.8° to 142.4°± 31.8°; P = .008) and external rotation (29.9°± 18.9° to 46.5°± 26.9°; P = .008). Centralization improved in the Walch index (from 0.58 ± 0.09 to 0.54 ± 0.05; P = .025) and contact point ratio (0.58 ± 0.08 to 0.51 ± 0.05; P < .001). Two glenoid components were removed due to posttraumatic injuries.
Conclusion:
All athletes returned to weight lifting, with 78% returning to the same or higher activity. Weight lifters regained substantial performance levels at a mean of 74% of their prearthritic lifetime 1RMs. The long-term results support the treatment of advanced glenohumeral arthritis with iTSA for active patients.
Keywords
Total shoulder arthroplasty (TSA) remains the gold standard for managing advanced glenohumeral arthritis.12,17,18,33,35 Although traditionally performed primarily in older populations, there is an emerging demand for TSA in younger patients due to increased glenohumeral stresses and earlier onset of shoulder osteoarthritis (OA). Advancements in implant technology, improved functional outcomes, and pain relief have contributed to this trend.27,37 While various TSA options are currently being utilized, a consensus on the preferred treatment modality for younger and active patients has yet to be established.
Compared to older individuals, younger and athletic populations often have higher expectations after TSA, including the ability to exercise and participate in sports. 13 Despite return-to-sport rates of 70% to 93% after TSA,9,22,34 literature-based recommendations for high-intensity upper extremity sports such as weight lifting are inconclusive. Moreover, postoperative activity restrictions vary and often depend on implant design, with many surgeons advising against participation in activities with fall potential and high impact. 24 A survey conducted among international surgeons revealed that 57% recommended against weight lifting after anatomic TSA, while 82% discouraged it after reverse TSA. 24 Long-term outcomes are limited, but several studies have demonstrated favorable short- to midterm outcomes among heavy weight lifters, with high return-to-sport rates and improved functional and radiographic outcomes.1,40
The purpose of this study was to examine the records of weight lifters treated with iTSA and determine their long-term sport performance and clinical outcomes. We hypothesized that treatment with iTSA would result in a high return-to-sport rate specific to weight lifting, accompanied by favorable performance levels and clinical outcomes in an active patient population.
Methods
Inclusion and Exclusion Criteria
This is a retrospective review of an institutional database focusing on competitive and high-level recreational weight lifters treated with iTSA. The indication for iTSA was advanced glenohumeral arthritis in patients with an intact rotator cuff confirmed on physical examination and preoperative imaging. Nonoperative management, including a combination of activity modification, oral anti-inflammatory medications, glenohumeral corticosteroid injections, and physical therapy, failed in all patients. Study inclusion criteria consisted of weight lifters younger than 65 years of age with a minimum follow-up of 2 years and a desire to return to sport and/or weight lifting competitions. Exclusion criteria consisted of non–weight lifting patients and individuals outside the age window. All procedures were performed on an outpatient basis by 2 fellowship-trained orthopaedic surgeons (J.E.Z., J.W.U.) at a single institution using the same TSA implant (OVO with Inlay Glenoid Arthroplasty System; Arthrosurface). The study was approved by the local ethics committee (11-046).
Surgical Technique
Patients underwent general anesthesia with 2 g cephalosporin for infection control and 1 g tranexamic acid to control bleeding. Patients were placed in the beach-chair position, and standardized draping was used. Dissection was performed through a modified deltopectoral approach extending into the axillary fold and carried out through the plane of the conjoint tendon junction. If necessary, the pectoralis major muscle was released in muscular patients to improve visualization. The subscapularis was tenotomized and tagged 1 cm medial to its insertion for later repair. The biceps tendon was visualized and palpated for integrity. When necessary, the biceps was tenotomized at the base of the labrum. Through use of electrocautery, the body of the labrum was separated from the glenoid circumferentially to improve glenohumeral mobility impeded by osteophyte formation and head deformity. The humeral head was dislocated anteriorly, and implant templates were used to measure appropriate anterior-posterior and superior-inferior sizing. Glenohumeral osteophytes were removed when present. A centering pin was placed, and the humeral head was reamed.
Attention was then given to the glenoid preparation. The humeral head was reduced, and posterior glenoid retractors were placed. The labrum was removed circumferentially, and the capsule was peeled back to visualize the glenoid. Using a guide wire, a centering pin was placed in the inferior glenoid vault, an offset reamer was used to prepare the vault, and the implant was trialed. Small glenoid channels were drilled for improved cementation. In cases with eccentric posterior glenoid erosion and posterior humeral head displacement, the glenoid was placed in a standard fashion after removing the ridge with a small burr. Glenoid retroversion was left unchanged to maintain soft tissue tension. After the glenoid placement, the humeral head was dislocated again for final humeral preparation and humeral component placement (material: cobalt-chromium alloy articular component with a titanium CPTi undersurface coating).
Rehabilitation
Patients were advised to wear a sling for 4 weeks. Gentle passive range of motion (ROM) and pendulum exercises were permitted during postoperative week 1. Supervised physical therapy began at postoperative week 4 and consisted of active assisted and unassisted motion exercises. Strengthening began once near-full ROM was achieved. External rotation was restricted until postoperative week 8. Patients continued progressive strengthening of the musculature about the rotator cuff with increased resistance at postoperative months 3 to 6. Patients were cleared to return to all activities without restriction at 6 to 12 months.
Patient Assessment and Perioperative Metrics
Perioperative risk was assessed using the American Society of Anesthesiologists (ASA) Physical Status Classification System. 15 Intraoperative risk variables included blood loss, transfusion requirements, and complications. Postoperative complication assessment included revision procedures and implant removals.
Patients were surveyed regarding their training routines and weight lifting frequency before OA symptom development and after iTSA. The primary outcome measure was the ability to return to weight lifting. The return to weight lifting level was determined using activity frequency. Categorization of lifting frequency was adapted from prior frameworks 28 : 1 session per week, 2 to 3 sessions, or ≥4 sessions per week. Weight lifting capability was evaluated based on patient-reported participation and performance during 4 upper body strength movements: bench press (barbell on a flat bench), military press (standing overhead movement using a barbell), single-arm overhead strict press (seated overhead press holding dumbbells in each arm), and barbell overhead strict press (seated overhead press using a barbell). Patients reported their lifetime maximum lift and current 1-repetition maximum (1RM) for each exercise: bench press, military press, and single-arm overhead strict press. Cumulative weight lifted for bench press and barbell overhead strict press was calculated by multiplying sets, repetitions, and weight lifted per movement (lb) during routine exercise.
Patient-reported outcomes (PROs) included the Western Ontario Osteoarthritis of the Shoulder Index (WOOS) percentage (scale: 0-100), American Shoulder and Elbow Surgeons (ASES) Shoulder Score (scale: 0-100), visual analog scale (VAS) pain score (scale: 0 for no pain to 10 for worst pain imaginable), and satisfaction score (scale: 0 for unsatisfied to 10 for very satisfied).5,7,23,26 ROM was assessed pre- and postoperatively on forward elevation and external rotation.
Radiographic Assessment
Radiographic assessments were performed by 2 fellowship-trained orthopaedic surgeons (J.E.Z., J.W.U) and 1 sports medicine orthopaedic surgery fellow (A.A.B.) utilizing a standard of care 2-view shoulder series (Grashey and axillary). All radiographs were obtained at the time of clinical examination. The preoperative glenoid wear pattern was categorized using the Walch classification system.38,40 Preoperative OA grading was categorized using the Samilson-Prieto classification system. 14 The Walch index and contact point ratios were used to determine centralization of the humeral head pre- and postoperatively, where 0.5 demonstrates humeral head centralization and values >0.5 indicate posterior subluxation. The contact point ratio, described by Matsen and Gupta, 25 was calculated by dividing the distance from the anterior rim of the glenoid to the center of the glenohumeral contact by the total distance between the anterior and posterior rims of the glenoid. 40 The Walch index was calculated using the mediatrice method bisecting the glenoid joint surface with a perpendicular line; the subluxation percentage was then determined by the ratio of the length of the humeral head segment posterior to this line to the total diameter of the humeral head.11,38,40 Glenoid radiolucency was assessed using a modified Lazarus 20 grading system as previously proposed for keeled glenoid components, and humeral head loosening was assessed according to Sanchez-Sotelo et al.31,32 Humeral and glenoid regions were segmented into 3 regions on axillary and anterior posterior radiographs (Figure 1). Humeral head loosening was defined as a threshold of ≥2 mm in ≥2 zones or if tilt or subsidence of the component was identified.31,32 Glenoid loosening was defined as complete radiolucency >2 mm.20,31

Assessment of periprosthetic radiolucent lines in radiographic imaging. (I) Grashey postoperative radiograph with an aspherical humeral head component with an inlay glenoid 10 years postoperatively: superior undersurface (A), inferior undersurface (B), and surrounding fixation (C). (II) Axillary postoperative radiograph with an aspherical humeral head component with an inlay glenoid 10 years postoperatively: anterior undersurface (A), posterior undersurface (B), and surrounding fixation (C).
Statistical Analysis
All statistical analyses were performed using R software Version 4.5.1 (R Core Team). Normality of the data distributions was assessed using the Shapiro-Wilk test. Continuous variables are reported as means with standard deviations or medians with interquartile ranges. Categorical variables are summarized as frequencies and percentages. Pre- and postoperative comparisons of radiographic centralization and PROs were conducted in patients with available baseline data. Depending on normality, either a parametric independent 2-sample t test or a nonparametric Wilcoxon rank-sum test was applied to compare baseline and last follow-up values in patients with available baseline data. The return to lifetime 1RM was calculated on an individual level and expressed as a percentage. The return to upper body strength movement was calculated on a patient level and expressed as a frequency and percentage. Statistical significance was defined as a 2-tailed P value <.05.
Results
Between 2011 and 2023, 41 patients (48 shoulders) with a history of weight lifting underwent total shoulder replacement at our institution and 18 male patients (24 shoulders) with a mean age of 54.6 ± 6.8 years were included in the study (Figure 2).

Flowchart of patient and shoulder inclusion.
No patient had prior shoulder surgeries. All patients were diagnosed with degenerative joint disease. Secondary diagnoses included loose bodies (n = 8), cystic mass (1 humerus, 1 subacromial, 1 subcoracoid), cystic degeneration (n = 1), and tenosynovitis of biceps tendon (n = 1). Preoperative sport levels included 3 competitive and 15 recreational weight lifters. Overall, 62.5% of procedures were performed on the dominant shoulder. Preoperative Walch classifications were as follows: A1 (25%), A2 (12.5%), B1 (4.2%), B2 (45.8%), and B3 (12.5%), with 79% of shoulders classified as OA grade 3. ASA classes were as follows: 1 (12.5%), 2 (54.2%), and 3 (25.0%). The median operation time was 131.5 minutes (IQR, 113.8-155.5 minutes). The estimated total blood loss was 99.0 ± 53.0 mL, with no patients requiring a blood transfusion. Two patients were discharged within 23 hours after an observational period, with the remaining patients being discharged the same day. Patient characteristics are outlined in Table 1.
Preoperative Patient Characteristics for Inlay Total Shoulder Arthroplasty Patients a
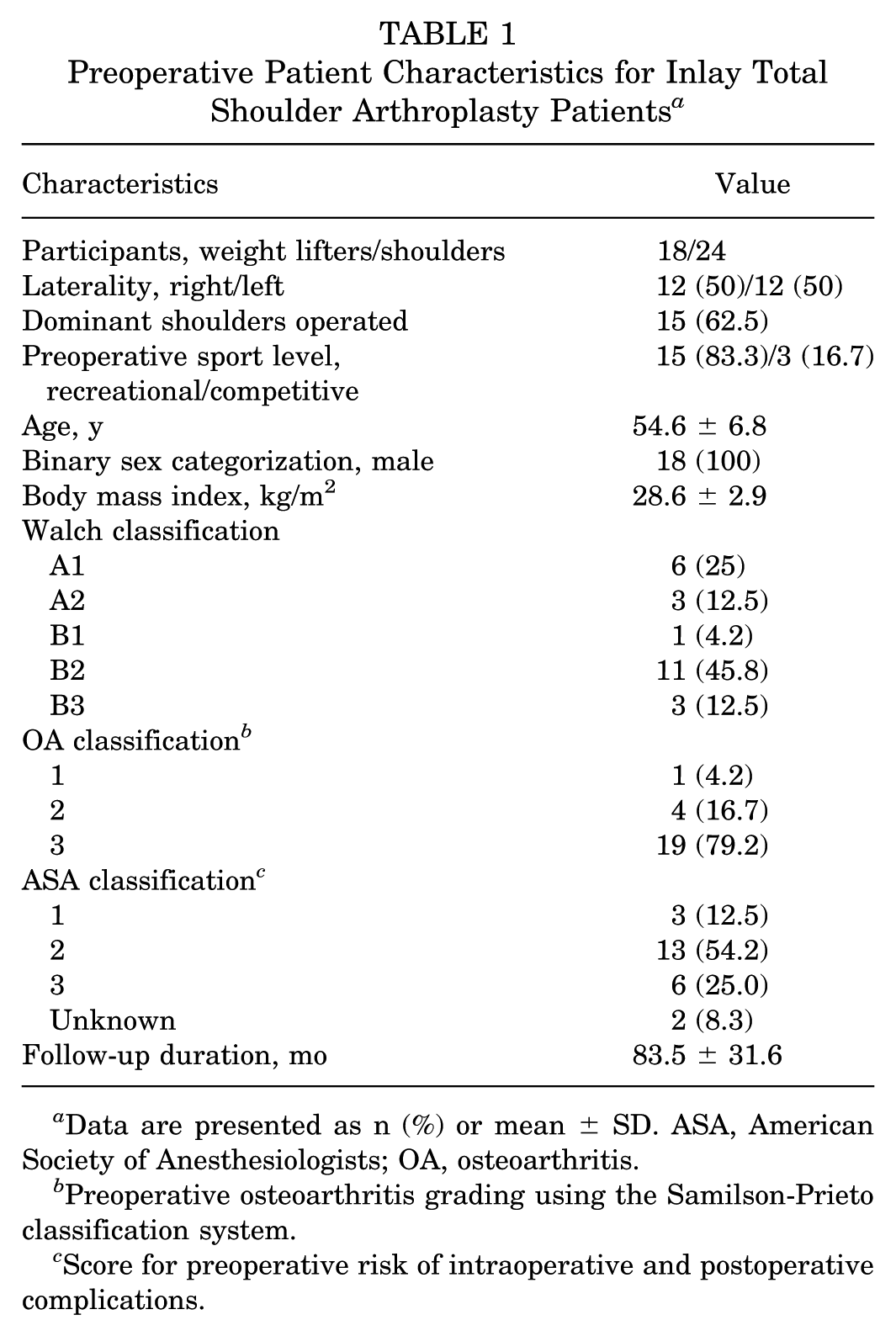
Data are presented as n (%) or mean ± SD. ASA, American Society of Anesthesiologists; OA, osteoarthritis.
Preoperative osteoarthritis grading using the Samilson-Prieto classification system.
Score for preoperative risk of intraoperative and postoperative complications.
Before OA symptoms, patients reported lifting frequencies of ≥4 sessions (n = 16) or 2 to 3 sessions (n = 8). During lifting sessions, athletes performed 3 sets for 10 repetitions at a mean of 179.5 ± 34.1 lb during bench press and 128.3 ± 47.8 lb during barbell overhead strict press. The preoperative mean lifetime 1RMs were 294.4 ± 104.0 lb for bench press, 113.0 ± 49.4 lb for single-arm overhead strict press, and 153.0 ± 63.2 lb for military press.
The return-to-sport rate was 100%, with all 18 patients maintaining their weight lifting activities at a mean follow-up of 83.5 ± 31.6 months. The postoperative median length of time to return to unrestricted weight lifting was 8.5 months (IQR, 6.0-24.0 months). At the last follow-up, 77.7% (n = 14) returned to the same or higher activity levels (Figure 3): 66.7% (n = 12) to the same level, 22.2% (n = 4) to a lower level, and 11.1% (n = 2) to a higher level. All 3 competitive lifters returned to the same level of activity. Recreational athletes who returned to lower activity levels reported a weekly weight lifting frequency of 2 to 3 sessions (n = 2) and 1 session (n = 2) per week.

Return to prearthritic weight lifting levels after inlay total shoulder arthroplasty.
Of the shoulders, 91.7% (n = 22) participated in pressing exercises at a mean frequency of 2.4 ± 1.3 days per week. Bench press and barbell overhead strict press sets and repetitions returned to pre-OA levels, whereas the weight lifted per repetition declined during bench press and overhead strict press (Table 2).
Performance Level: Return to Cumulative Weight Lifted After Inlay Total Shoulder Arthroplasty a

Data are presented as mean ± SD unless otherwise indicated.
Barbell on a flat bench.
Cumulative weight lifted was calculated by multiplying sets, repetitions, and weight lifted per movement (lb) on a patient level.
Seated overhead press using a barbell.
Return to cumulative weight lifted was calculated on an individual level for patients who returned to exercise movement.
The cumulative weight lifted returned to significantly similar lifetime maximum levels in bench press (P = .177) for athletes who returned to upper body strength movement. On an individual level, weight lifters returned to 56% to 74% of their lifetime 1RM for the bench press, single-arm overhead strict press, and military press (Table 3).
Performance Level: Return to 1 Repetition Maximum After Inlay Total Shoulder Arthroplasty a

Data are presented as n (%) or mean ± SD unless otherwise indicated.
Barbell on a flat bench.
Seated overhead press holding dumbbells in each arm.
Standing overhead movement using a barbell.
Return to upper body strength movement was calculated on a procedure level.
Return to lifetime maximum was calculated on an individual level for patients who returned to exercise movement.
The mean follow-up PROs included 81.7% ± 21.0% for WOOS percentage, 86.7 ± 16.9 for ASES score, and 1.0 ± 2 for VAS pain score. At the last follow-up, the mean satisfaction score was 8.8 ± 1.5. Patients significantly improved their preoperative ROM on forward elevation (from 117.6°± 34.8° to 142.4°± 31.8°; P = .008) and external rotation (from 29.9°± 18.9° to 46.5°± 26.9°; P = .008). Subgroup analysis in patients with baseline PROs (12/24) demonstrated significant improvements across all measures: WOOS percentage (P = .003), ASES score (P < .001), and VAS pain score (P < .001) (Table 4).
Summary of Patient-Reported Outcomes a

Data are presented as mean ± SD unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; NA, not applicable; VAS, visual analog scale; WOOS, Western Ontario Osteoarthritis of the Shoulder Index.
On radiographic analysis at the final follow-up, the Walch index significantly improved (from 58% ± 9% to 54% ± 5%; P = .025). Contact point ratios improved from 58% ± 8% preoperatively to 51% ± 5% at the last follow-up (P < .001). Two glenoid components were removed, and the remaining shoulders were not considered clinically at risk of periprosthetic radiolucency.
No intraoperative complications were encountered. Three patients experienced postoperative ipsilateral complications unrelated to the index procedure. All maintained long-term function and proceeded with contralateral iTSA. Patient 1 sustained a greater tuberosity fracture 33 months after iTSA that was managed nonoperatively (bony union: 79 days). At the 7-year follow-up, he reported 90% Single Assessment Numeric Evaluation (SANE) shoulder scores and activities without restrictions. Patient 2 sustained a fall from a roof, resulting in left hand and elbow fractures requiring open reduction and internal fixation 2 months after iTSA. He underwent glenohumeral arthroscopic capsular release, lysis of adhesions, and debridement of scar tissue 12 months after iTSA to relieve pain in the posterior aspect of the shoulder. He underwent loose bone fragment removal, synovectomy of the glenohumeral joint, and glenoid component removal 24 months after iTSA to relieve pain during daily activities and lifting. Nine years after iTSA, the patient maintained regular weight lifting with an 80% SANE score and underwent iTSA on the contralateral side 11 years after primary iTSA. Patient 3 developed shoulder instability after a boating accident 7 weeks after iTSA. Repair of a chronically torn subscapularis tendon, lysis of adhesions, and debridement of scar tissue were performed 11 months after iTSA, followed by glenoid component removal 24 months after iTSA due to infection and component loosening. He maintained regular weight lifting ≥4 times per week at 5 years after the index procedure.
Discussion
The purpose of this study was to assess the return-to-sport and long-term clinical outcomes after iTSA in a series of active weight lifters with advanced glenohumeral OA. All patients returned to unrestricted weight lifting at a median of 8.5 months. Most returned to regular activity, with 78% returning to the same or higher weekly lifting frequency and 56% to 74% functional strength recovery across the bench press, single-arm overhead strict press, barbell overhead strict press, and military press. High satisfaction, functional outcomes, and minimal pain were reported at a mean follow-up of 7 years. Improved centralization of the humeral head was achieved, and no gross loosening of the humeral component was observed. The glenoid component was removed in 2 cases due to posttraumatic injuries. All other glenoid components were stable, with no signs of clinically relevant radiolucency at the last follow-up.
As younger and more active populations undergo TSA, the expectations and rehabilitation goals continue to rise. In a systematic review, including 13 studies and 944 patients, anatomic TSA had higher return-to-sport rates than reverse TSA (92.6% vs 74.9%; P = .003). 22 However, studies reporting sport-specific rates of return (9 studies, 368 patients) noted no difference in return to the same level (P = .41). Nevertheless, more surgeons discourage weight lifting after reverse TSA (82%) compared to anatomic TSA (57%). 24 Surgeon recommendations for high-impact activities after TSA remain inconsistent, limiting patient expectations.
An alternative TSA design, iTSA, was adopted, which may withstand the performance demands and repetitive stresses associated with heavy weight lifting. 40 Inlay TSA combines a stemless, aspherical humeral head with an inlay glenoid, preserving proximal bone stock and providing a closer anatomic match with less implant volume in the anterior-posterior plane.16,21 The inlay glenoid design provides improved component stability while minimizing joint lateralization and intra-articular volume expansion. Previous studies have demonstrated excellent clinical and radiographic outcomes in challenging patient populations with this design.3,36
At a longer-term follow-up, our study builds on short- and midterm outcomes among heavy weight lifters. Ames et al 1 reported that 86.1% of patients returned to sport after anatomic TSA, with 63.9% resuming weight lifting and achieving 47% to 77% of prior strength across lifts. Our patients achieved similar strength recovery, returning to >50% of their lifetime 1RMs across the bench press, single-arm overhead strict press, and military press. Patients also maintained similar weight lifting frequencies postoperatively compared to their presymptomatic levels, with 78% returning to the same or higher activity.
Using the same implant system as our study, Yalcin et al 40 reported 100% return to sport in competitive weight lifters, with 50% of patients lifting the same weight and 44% exceeding their preoperative maximums. At a median follow-up of 38 months, significant improvements were seen in the Walch index (P < .001) and contact point ratio (P < .001). Our findings support the favorable outcomes reported in earlier studies and reconfirmed glenoid centralization. Our study expands on the subject by incorporating objective strength measures and longer-term data.
The risk of glenoid component loosening remains a concern in active patient populations.4,6 Although a systematic review conducted by Roberson et al, 29 consisting of 6 studies, reported a revision rate of 17% and radiolucency of 54% in TSA patients younger than 65 years of age at a mean follow-up of 9 years, significant improvements were observed in PROs, ROM, and pain. Our study demonstrated no gross loosening in 22 shoulders and 2 revisions due to posttraumatic injuries.
Glenoid loosening, specifically the “rocking horse phenomenon,” is a concern for TSA.2,4,6,8 Gagliano et al 8 compared loading force distribution and loosening after fatigue testing in onlay versus inlay glenoid prosthetics in 16 prescreened cadaveric shoulders (8 pairs). Their results indicate that force was greater in the onlay compared to the inlay prosthetics, and all onlay glenoid components showed gross loosening after a mean of 1126 cycles of a simulated rocking-horse mechanism (5 mm of anterior-posterior humeral translation). All inlay glenoid components remained intact without gross loosening after fatigue testing. Our results support these claims, with no gross loosening in the humeral head, and the majority of implants maintained position despite repetitive high loading.
Glenoid retroversion, posterior erosion, biconcavity, and humeral head subluxation are associated with glenoid loosening and, ultimately, TSA failure. 39 Eccentric posterior glenoid erosion and posterior humeral head displacement, frequently seen in weight lifters with Walch class B2, raise the risk of accelerated implant wear after TSA. 19 Therefore, additional surgical steps to ensure proper glenoid placement are often advised, avoiding persistent posterior subluxation and ensuring centralization of the humeral head. Matsen and colleagues described a “ream and run” technique to improve humeral head centering on the glenoid. The ream and run technique has been shown to improve Simple Shoulder Test scores,10,25,30 although Gilmer et al 10 found the prognosis for improvement was best in patients >60 years of age. Two athletes in our cohort returned to weight lifting with no restrictions after glenoid component removal. Future studies are needed to determine the effectiveness of the ream and run technique in a relatively young and active population.
There are several limitations in this study. While the statistical power is limited by the small cohort size, active weight lifters with a desire for sport continuation undergo TSAs less frequently than older individuals with no desire to start or return to weight lifting. Additionally, the absence of a control or comparison group limits generalizability. While the mean follow-up was 7 years, 7 shoulders were not evaluated past the 5-year time point. The detailed, long-term functional and radiographic follow-up provides clinically meaningful insights. There was a high loss to follow-up, and only 12 of 24 shoulders had complete baseline PRO measures, limiting the ability to assess the magnitude of improvement across the full cohort. In those with complete data, significant improvements were demonstrated across all PROs. Preosteoarthritic strength and lifting data were collected via retrospective patient recall with some athletes missing data, which may introduce bias. However, this bias is minimized by the inclusion of athletes who typically track training progress, metrics, and personal records. Importantly, the primary endpoint of the study was return to weight lifting.
Conclusion
Inlay TSA demonstrated 100% return to weight lifting in active patients with excellent functional recovery and satisfaction at long-term follow-up. Weight lifting frequency returned to preosteoarthritic levels, with 78% returning to the same or higher activity levels and similar repetitions and sets performed during bench press and barbell overhead strict press. Lifetime 1RMs returned to a mean of 74% of their prearthritic levels. Glenohumeral recentering was sustained at a mean follow-up of 7 years. This study may assist surgeons in providing postoperative counseling and setting expectations for individuals interested in resuming high activity levels. Our results support the treatment of advanced glenohumeral arthritis with iTSA in relatively young and active patients and provide further evidence to strengthen patient expectation management.
Footnotes
Final revision submitted February 18, 2026; accepted February 26, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.E.Z. received consulting fees from Arthrex, Arthrosurface, and Anika Therapeutics; hospitality payments from Arthrex; and education payments from Zimmer Biomet Holdings. J.W.U. received consulting fees from Anika Therapeutics and royalties or license from Linvatec Corporation.
Ethical approval for this study was obtained from the Baptist Health South Florida Institutional Review Board (IRB protocol 11-046).