
Abstract
Background:
While quadriceps tendon (QT) autograft is being increasingly utilized for primary anterior cruciate ligament reconstruction (ACLR), there remains limited evaluation of how QT autograft diameter and the ratio of graft diameter to femoral notch width (D-N ratio) affect clinical outcomes, such as rates of symptomatic knee stiffness or revision ACLR.
Hypothesis:
Larger QT autograft diameter and D-N ratio would be associated with higher rates of subsequent surgery for knee stiffness, whereas a smaller QT autograft diameter and D-N ratio would be associated with higher rates of revision ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All consecutive patients age ≥14 years who underwent primary QT autograft ACLR between 2011 and 2021 were analyzed. Exclusion criteria were <6-month follow-up, double-bundle ACLR, and concomitant procedures other than meniscal repair. Rates of subsequent surgery for knee stiffness and revision ACLR were evaluated at minimum 6-month and 24-month follow-up, respectively. Demographic and surgical variables were compared between knee stiffness and revision ACLR groups. Significance was set to P < .05.
Results:
A total of 374 patients (mean ± SD age, 22 ± 7 years; 42% female) met inclusion criteria, of which 209 patients (mean age: 23 ± 7 years; 49% female) had minimum 24-month follow-up. The rate of subsequent surgery for knee stiffness was 9.9% (37/374 patients), and the rate of revision ACLR was 9.6% (20/209 patients). Lateral meniscal repair (odds ratio [OR], 2.5; 95% CI, 1.2-5.2; P = .02) and D-N ratio >0.55 (OR, 3.4; 95% CI, 1.2-9.7; P = .02) were identified as independent predictors of subsequent surgery for knee stiffness. There was no significant difference in QT autograft diameter (9.2 vs 9.5 mm; P = .17), femoral notch width (17.3 vs 17.7 mm; P = .64), nor D-N ratio (0.54 vs 0.54; P = .87) between patients who underwent revision ACLR versus no revision ACLR.
Conclusion:
D-N ratio >0.55 and concomitant LM repair were associated with significantly higher odds of undergoing subsequent surgery for knee stiffness after QT autograft ACLR. Conversely, QT autograft diameter and D-N ratio were not associated with undergoing revision ACLR. Avoiding overstuffing of the femoral notch may reduce risk of subsequent surgery for knee stiffness without increasing the risk of undergoing revision ACLR.
The use of quadriceps tendon (QT) autograft during primary anterior cruciate ligament (ACL) reconstruction (ACLR) has gained popularity in recent years, 9 as it allows a more predictable graft size than hamstring tendon (HT) autografts,3,4,29 increased collagen fiber thickness compared with similar-sized bone–patellar tendon–bone (BPTB) autografts, 12 and less donor-site morbidity compared with both HT and BPTB autograft use.8,20 Conversely, a notable limitation of QT autograft use is potentially greater quadriceps strength asymmetry and muscle inhibition in the post-operative period, especially when compared to HT autograft use.15,19,37 Further, while the larger size of QT autografts enables restoration of the native ACL footprint, 28 recent clinical data suggest larger QT autografts may translate to a higher incidence of knee stiffness compared with other graft types.13,17 However, the relationship between the use of QT autograft and incidence of knee stiffness postoperatively remains unclear.2,16,34
Graft diameter ≥8 mm is often utilized during primary ACLR, as several studies have demonstrated a higher risk of revision ACLR after use of HT autografts <8 mm.6,21,23 However, recent literature evaluating revision ACLR rates after HT autograft use have challenged the 8 mm–graft diameter threshold, suggesting either lower thresholds such as 7-mm graft diameter or lack of association between graft diameter and risk of revision ACLR.1,14,25 Nevertheless, possibly given the larger size of QT versus HT autografts, there remains limited evaluation of how QT autograft diameter during primary ACLR affects clinical outcomes, such as rates of symptomatic knee stiffness or revision ACLR.10,16 Further, while a smaller femoral notch width has been identified as a risk factor for revision ACLR,5,16,36,41 there is limited evaluation of the relationship between QT autograft diameter and femoral notch width and the impact of this relationship on clinical outcomes after primary QT autograft ACLR. 16
The purpose of this study was to evaluate the impact of QT autograft diameter, and the ratio of QT autograft diameter to femoral notch width (D-N ratio), on rates of subsequent surgery for knee stiffness and revision ACLR after primary QT autograft ACLR. The hypothesis was that a large QT autograft diameter and D-N ratio would be associated with higher rates of subsequent surgery for knee stiffness, whereas a small QT autograft diameter and D-N ratio would be associated with higher rates of revision ACLR.
Methods
Data Collection
This retrospective study was approved by the institutional review board at the University of Pittsburgh. All consecutive patients aged ≥14 years who underwent primary anatomic single-bundle ACLR with QT autograft between 2011 and 2021 by 1 of 8 sports medicine fellowship–trained orthopaedic surgeons (J.D.H. and V.M.) were included for analysis. Exclusion criteria included revision ACLR, double-bundle ACLR, posterolateral ligament augmentation, or concomitant lateral extra-articular tenodesis, meniscus root repair, meniscal allograft transplantation, or osteochondral procedure.
Demographic data including age, sex, body mass index, and sports participation were obtained from chart review. Surgical variables were collected from chart review and operative notes and included concomitant repair of the medial meniscus (MM) or lateral meniscus (LM), QT autograft diameter (recorded in mm), and femoral notch width (recorded in mm). QT autograft diameter was recorded from operative notes and determined based on surgeon discretion during preoperative planning and at time of surgery. As described previously, the femoral notch width was measured at the level of the popliteal femoral insertion point using the coronal T1 magnetic resonance imaging (MRI) slice where the popliteal femoral insertion point was most prominently seen (Figure 1). 38 Finally, the D-N ratio was calculated as the autograft diameter divided by the femoral notch width and recorded as a ratio from 0 to 1. A smaller QT autograft diameter relative to femoral notch width would result in a smaller D-N ratio, whereas a larger QT autograft diameter relative to femoral notch width would result in a larger D-N ratio.

Measurement of the femoral notch width. Using the coronal T1 slice in which the popliteal femoral insertion point (asterisk) was most clearly visible, a line was drawn connecting the most inferior portion of the medial and lateral femoral condyles. A second line was drawn parallel to the first line at the level of the popliteal femoral insertion point, from which the notch width (a) was identified.
Femoral notch width measurements were performed by 2 independent raters (orthopaedic surgery resident physicians (S.D. and R.P.V.) with significant experience in orthopaedic research and knee-related imaging measurements. Interrater agreement and intrarater agreement was determined by calculating intraclass correlation coefficients (ICCs) for femoral notch width. ICCs were noted to be excellent for both interrater (ICC, 0.94) and intrarater (ICC, 0.97) reliability.
The primary outcome measures were subsequent surgery for knee stiffness (including manipulation under anesthesia (MUA), lysis of adhesions, and debridement of cyclops lesions) and revision ACLR. The indications for subsequent surgery for knee stiffness included loss of knee extension >5° at a minimum of 3 months postoperatively (after initial trial of nonoperative management), loss of knee flexion >10° along with loss of knee extension as above, and/or MRI-confirmed evidence of a cyclops lesion. Subsequent surgery for knee stiffness was evaluated among all patients with minimum 6-month follow-up, and revision ACLR was evaluated among all patients with minimum 24-month follow-up. After obtaining informed consent, all patients who met inclusion criteria were contacted via telephone and/or email to collect updated information regarding subsequent knee surgeries, and final follow-up length was determined by date of telephone survey completion or date of last in-office follow-up.
Surgical Procedure
All patients underwent primary anatomic single-bundle ACLR with ipsilateral QT autograft. The QT autograft was harvested just lateral to the vastus medialis oblique muscle, and graft thickness, diameter, and harvest of patellar bone block were determined based on surgeon discretion. Standard diagnostic arthroscopy was then performed to evaluate for concomitant cartilage and/or meniscal lesions. Notchplasty was not performed in any patient, because previous literature has demonstrated that notchplasty may alter knee biomechanics and affect graft accommodation without significant difference in clinical outcomes such as graft failure.22,35,42 Following diagnostic arthroscopy, the femoral tunnel was drilled through the anteromedial portal in the center of the anatomic ACL femoral footprint, and the tibial tunnel was drilled via an outside-in technique using a tibial guide in the center of the anatomic ACL tibial footprint. The QT autograft was passed and fixated on the femoral and tibial sides utilizing continuous or adjustable loop suspensory fixation, or interference screws, based on surgeon-specific technique. Fixation was performed at 90° of knee flexion for the femoral side and in slight flexion with a posterior drawer force for the tibial side. Following surgery, all patients were weightbearing as tolerated immediately unless a concomitant meniscal repair was performed, in which case patients were instructed to remain toe-touch weightbearing for 6 weeks. All patients were placed in a hinged knee brace for 6 weeks postoperatively, after which time the brace was discontinued. Patients who received concomitant meniscal repair were restricted to 0° to 90° of knee range of motion (ROM) for the first 4-6 weeks, then advanced to full ROM. The patients progressed through a stepwise physical therapy protocol that was dictated by patient progress and milestones. The patients were released to full sport at a minimum of 9 months postoperative based on progress with physical therapy and their passing of specific objective criteria, including strength symmetry of 90% and functional testing. 7
Statistical Analysis
Demographic and surgical variables were compared between groups who underwent subsequent surgery for knee stiffness versus not, as well as between groups who underwent revision ACLR versus not. Univariate analysis was performed using independent t test or Mann-Whitney U test for parametric and nonparametric data, respectively, and chi-square test for categorical dichotomous variables. Receiver operating characteristic (ROC) curves were generated to identify the D-N ratio cutoff for subsequent surgery for knee stiffness and revision ACLR with the highest Youden index, indicating the cutoff value with the most optimal sensitivity and specificity. Binary logistic regression analysis was performed to determine independent predictors of undergoing subsequent surgery for knee stiffness or revision ACLR. Finally, predicted probabilities of subsequent surgery for knee stiffness and revision ACLR were calculated from regression models and plotted against D-N ratio to generate a graph of predicted probability of each outcome. Significance for all tests was set to P < .05.
An a priori power analysis was performed to determine sample size required to detect a 0.5-mm difference in mean QT autograft diameter between patients who underwent subsequent surgery for knee stiffness or revision ACLR versus not. With an estimated rate of 10% for both subsequent surgery for knee stiffness and revision ACLR, 7 standard deviation of 0.8 mm for QT autograft diameter, 7 and 2-sided alpha of .05, the sample size analysis indicated that 22 patients in the subsequent surgery for knee stiffness or revision ACLR group and 224 patients in the group without subsequent surgery for knee stiffness or revision ACLR would be required to achieve 80% power (total of 246 patients).
Results
Total Study Population
After applying exclusion criteria, a total of 374 patients (mean ± SD age, 22 ± 7 years; 156 [42%] female) with minimum 6-month follow-up were included for analysis, of which 209 patients (mean age, 23 ± 7 years; 102/209 [49%] female) had minimum 24-month follow-up. The follow-up rate was 82% at 6 months and 46% at 24 months. Baseline demographics were found to be similar between patients with 6-month and 24-month follow-up (Table 1). The overall rate of subsequent surgery for knee stiffness was 9.9% (37/374 patients), and the overall rate of revision ACLR was 9.6% (20/209 patients).
Demographic Comparison Between Patients With 6-Month Versus 24-Month Follow-up a

Data are presented as n (%) or mean ± SD. Bold P value indicates significant finding at p < 0.05 level. BMI, body mass index.
In the total study population, mean QT autograft diameter was 9.6 ± 0.7 mm (range, 7.0-11.5 mm), mean femoral notch width was 18.3 ± 2.7 mm (range, 12.1-27.3 mm), and mean D-N ratio was 0.53 ± 0.08 (range, 0.29-0.76). The distribution of QT autograft diameters in the total study population is shown in Appendix Table A1.
Subsequent Surgery for Knee Stiffness
There were no significant differences in demographic variables between patients who underwent subsequent surgery for knee stiffness and those who did not (Table 2). Surgical variables associated with undergoing subsequent surgery for knee stiffness included concomitant LM repair (38% vs 20%; P = .02), smaller femoral notch width (17.5 vs 18.4 mm; P = .02), higher mean D-N ratio (0.56 vs 0.53; P = .04), and D-N ratio >0.55 (59% vs 33%; P = .003) (Table 3). QT autograft diameter was not found to statistically differ between patients who underwent subsequent surgery for knee stiffness versus patients who did not undergo subsequent surgery for knee stiffness (9.5 vs 9.6 mm; P = .41) (Table 3). Binary logistic regression analysis identified concomitant LM repair (odds ratio [OR], 2.45; 95% CI, 1.17-5.15; P = .02) and D-N ratio >0.55 (OR, 3.36; 95% CI, 1.17-9.65; P = .02) as independent predictors of undergoing subsequent surgery for knee stiffness (Table 4).
Demographic Comparison Between Patients Who Underwent Subsequent Surgery for Knee Stiffness Versus Not a

Data are presented as n (%) or mean ± SD. BMI, body mass index.
Surgical Characteristics Between Patients Who Underwent Subsequent Surgery for Knee Stiffness Versus Not a

Data are presented as n (%) or mean ± SD. Bold P values indicate significant finding at p < 0.05 level. D-N ratio, graft diameter to femoral notch width ratio; LM, lateral meniscus; MM, medial meniscus.
Binary Logistic Regression for Subsequent Surgery for Knee Stiffness a

Bold P values indicate significant finding at p < 0.05 level. Nagelkerke R2 = 0.086. D-N ratio, graft diameter to femoral notch width ratio; LM, lateral meniscus.
ROC curve analysis identified a D-N ratio of 0.55 as an optimal cutoff for subsequent surgery for knee stiffness (sensitivity, 61%; specificity, 66%), with an area under the curve (AUC) of 0.61 (Figure 2).

The receiver operating characteristic (ROC) curve was generated to identify the diameter-to-notch (D-N) ratio cutoff for subsequent surgery for knee stiffness.
Revision ACLR
There were no significant differences in demographic variables between patients who underwent revision ACLR and those who did not (Table 5). Additionally, there was no significant difference in QT autograft diameter (9.2 vs 9.5 mm; P = .17), femoral notch width (17.3 vs 17.7 mm; P = .64), mean D-N ratio (0.54 vs 0.54; P = .87), or proportion of patients with D-N ratio >0.64 (20% vs 12%; P = .29) between patients who underwent revision ACLR versus not (Table 6).
Demographic Comparison Between Patients Who Underwent Revision ACLR Versus No Revision ACLR a

Data are presented as n (%) or mean ± SD. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index.
Surgical Characteristics Between Patients Who Underwent Revision ACLR Versus No Revision ACLR a

Data are presented as n (%) or mean ± SD. D-N ratio, graft diameter to femoral notch width ratio; LM, lateral meniscus; MM, medial meniscus.
ROC curve analysis identified a D-N ratio of 0.64 as an optimal cutoff for revision ACLR (sensitivity: 21%, specificity: 88%), with an AUC of 0.48 (Figure 3).

A receiver operating characteristic (ROC) curve was generated to identify the diameter-to-notch (D-N) ratio cutoff for revision anterior cruciate ligament reconstruction.
Predicted Probability of Outcomes
The predicted probability of undergoing subsequent surgery for knee stiffness and revision ACLR based on D-N ratio is shown in Figure 4. With increasing D-N ratio, there was an exponential increase in predicted probability of undergoing subsequent surgery for knee stiffness, as well as a small linear decrease in the predicted probability of undergoing revision ACLR with increasing D-N ratio. With increasing D-N ratio, the range of predicted probability of undergoing subsequent surgery for knee stiffness was 3.4% (D-N ratio of 0.29) to 24.3% (D-N ratio of 0.76). With increasing D-N ratio, the range of predicted probability of undergoing revision ACLR was 10.8% (D-N ratio of 0.29) to 8.9% (D-N ratio of 0.73). The intersection point of the predicted probability curves for subsequent surgery for knee stiffness and revision ACLR was a D-N ratio of 0.53, which corresponded to a 9.8% predicted probability of undergoing subsequent surgery for knee stiffness and a 9.7% predicted probability of revision ACLR.
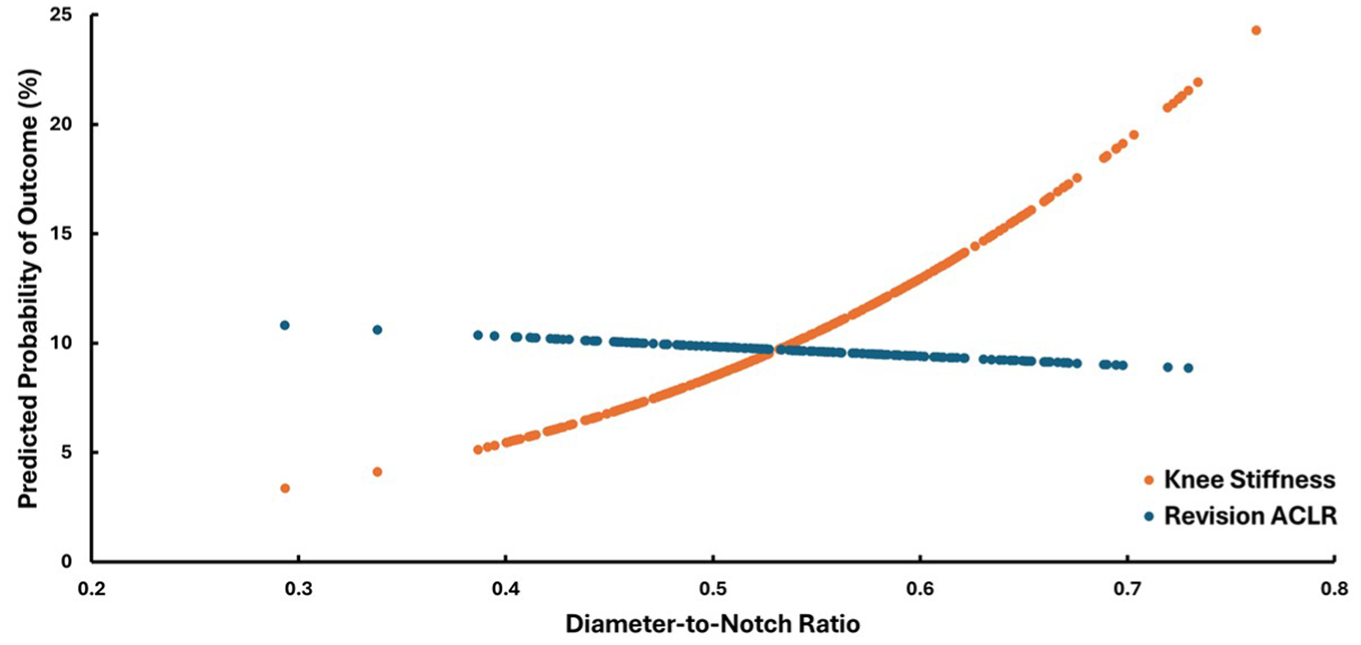
Predicted probability of undergoing subsequent surgery for knee stiffness or revision anterior cruciate ligament reconstruction (ACLR) based on diameter-to-notch ratio.
Discussion
The most important finding of this study was that a D-N ratio >0.55 was associated with >3 times higher odds of undergoing subsequent surgery for knee stiffness after primary QT autograft ACLR, whereas QT autograft diameter, femoral notch width, and D-N ratio were not associated with undergoing revision ACLR. The data from this study suggest that avoidance of overstuffing the femoral notch with the QT autograft may decrease risk of subsequent surgery for knee stiffness without significantly increasing risk of undergoing revision ACLR after primary QT autograft ACLR.
Prior studies have identified a smaller femoral notch width and anterior graft placement as risk factors for arthrofibrosis and cyclops lesions resulting in knee stiffness after ACLR.11,24,26,30 This is likely due to increased graft-notch impingement resulting in loss of knee extension. 24 Literature evaluating the impact of graft diameter on postoperative outcomes after ACLR has mainly identified a higher risk of revision ACLR with graft diameter <8 mm,6,21,23 with limited literature evaluating the impact of larger graft diameters on rates of knee stiffness after ACLR. With regard to QT autograft specifically, available evidence demonstrates higher rates of MUA following use of QT autograft versus other graft choices during ACLR, 17 possibly secondary to quadriceps muscle inhibition, though this relationship remains unclear,15,18,39 as well as increased risk for cyclops syndrome with QT autograft diameter >9.25 mm.13,17 However, graft-notch impingement resulting in loss of knee extension is influenced by both autograft diameter and femoral notch width, and therefore it is paramount to view both variables in tandem when evaluating rates of postoperative knee stiffness. 16 In the present study, a D-N ratio >0.55 was associated with 3 times higher odds of undergoing subsequent surgery for knee stiffness, which may serve as a threshold for surgeons during preoperative planning of appropriate QT autograft diameter based on femoral notch morphology. However, future studies may be warranted to further validate the present findings. Based on the results of this study, the authors are currently selecting smaller graft diameters during QT ACLR in an effort to mitigate risk of postoperative knee stiffness requiring subsequent surgery.
In contrast, QT autograft diameter and D-N ratio were not associated with higher rates of revision ACLR in this study. This may be explained by the fact that, in the present study, nearly all included QT autografts were ≥8 mm in diameter, which is above the commonly cited threshold associated with higher risk of revision ACLR.6,21,23 However, this represents an important advantage of QT autografts, in that QT autografts ≥8 mm in diameter can be reliably harvested in most patients, compared with HT autografts where graft size is often highly dependent on patient characteristics.4,10,31 Based on the findings of this study, with QT autograft diameter ≥8 mm, there does not appear to be an influence of QT autograft diameter on risk of revision ACLR. This is an important finding of the study as, in conjunction with the higher rate of subsequent surgery for knee stiffness with D-N ratio >0.55, surgeons may individualize QT autograft diameter based on femoral notch morphology to decrease risk of both knee stiffness and revision ACLR postoperatively.28,43 Future biomechanical and/or clinical studies may be needed to evaluate the load to failure and revision ACLR risk with QT autografts <8 mm, as this was not captured in the present study.
Finally, concomitant LM repair was found to be an independent predictor of undergoing subsequent surgery for knee stiffness after primary QT autograft ACLR. Although the literature remains conflicted, several other recent studies have demonstrated an association between concomitant LM repair and knee stiffness postoperatively.13,17,27,33 Possible reasons for this relationship include delayed weightbearing and ROM postoperatively to protect the meniscal repair compared with isolated ACLR, increased tightening of the knee capsule as a result of placement of the meniscal repair implant, and increased intra-articular inflammation postoperatively in the setting of combined ACLR with meniscal repair, which may contribute to scar formation.13,17,32 Additionally, LM repair performed at the time of ACLR has been linked to increased flexion and extension strength deficit compared to ACLR with MM repair or isolated ACLR, which may explain the higher rate of subsequent surgery for knee stiffness. 40 The present study found 2.5 times higher odds of undergoing subsequent surgery for knee stiffness after ACLR with concomitant LM repair, increasing the evidence for an association between concomitant LM repair and postoperative knee stiffness. These data may support individualized rehabilitation protocols following QT autograft ACLR combined with LM repair to minimize risk of subsequent surgery for knee stiffness.
Limitations
There are several limitations to the present study. First, the 6-month and 24-month follow-up rate was 82% and 46%, respectively, which places the study at risk for selection bias. Second, the small between-group difference in mean QT autograft diameter between patients who underwent, or did not undergo, subsequent surgery for knee stiffness and/or revision ACLR increases the risk that the present study was underpowered to identify true differences in univariate analysis. However, all consecutive patients undergoing primary QT autograft ACLR over a 10-year time span were reviewed for potential inclusion to maximize the number of patients available for inclusion in this study. Third, there is risk for selection bias, as only 35 patients had QT autograft size <9 mm. Finally, the present study's outcomes included subsequent surgery for knee stiffness, which does not include patients who experienced knee stiffness but did not undergo subsequent surgery for knee stiffness, as well as revision ACLR, which does not include patients who experienced clinical graft failure but did not undergo revision ACLR. As a result, the outcome measure reported in the study may reflect an underestimation of the true prevalence of knee stiffness and revision ACLR after QT autograft ACLR.
Conclusion
D-N ratio >0.55 and concomitant LM repair were associated with significantly higher odds of undergoing subsequent surgery for knee stiffness after QT autograft ACLR. Conversely, QT autograft diameter and D-N ratio were not associated with undergoing revision ACLR. Avoiding overstuffing of the femoral notch may reduce risk of subsequent surgery for knee stiffness without increasing the risk of undergoing revision ACLR.
Footnotes
Appendix
Distribution of Graft Diameters in Total Patient Population a
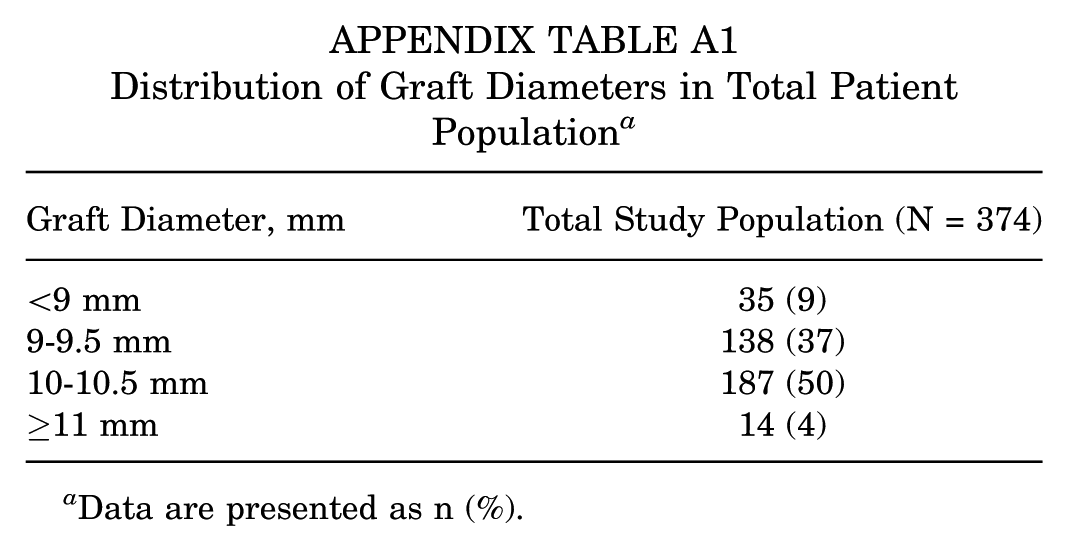
| Graft Diameter, mm | Total Study Population (N = 374) |
|---|---|
| <9 mm | 35 (9) |
| 9-9.5 mm | 138 (37) |
| 10-10.5 mm | 187 (50) |
| ≥11 mm | 14 (4) |
Data are presented as n (%).
Final revision submitted February 10, 2026; accepted February 16, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.D.H. is on the editorial board of Knee Surgery, Sports Traumatology, and Arthroscopy (KSSTA) and Annals of Joint and is a consultant for Smith & Nephew. J.J.I. is the president of the board of directors of Movement Science Media/Journal of Orthopaedic and Sports Physical Therapy. V.M. is on the editorial board of KSSTA, is chair of research for AOSSM, and serves as a consultant for Smith & Nephew.
Ethical approval for this retrospective study was obtained from the institutional review board of the University of Pittsburgh (No. STUDY19030196).