
Abstract
Background:
Acetabular labral tears are a common cause of hip pain. While larger tear size has been linked to worse outcomes after arthroscopic treatment, the influence of labral tear location remains incompletely understood.
Purpose:
To investigate how labral tear location affects functional outcomes, conversion to total hip arthroplasty (THA), and patient satisfaction after arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary hip arthroscopy were retrospectively sent online surveys at a minimum of 8 years after their surgery. Tear location was classified into superior, anterosuperior, and posterosuperior based on intraoperative findings. Outcomes included patient-reported outcome measures, conversion to THA, Patient Acceptable Symptom State improvement, and overall patient satisfaction. Unadjusted and adjusted logistic regression models were performed to identify potential confounding variables.
Results:
In total, 138 patients were included with a mean ± SD follow-up time of 11.1 ± 2.5 years. There was no significant difference in all postoperative patient-reported outcome measures across tear locations, although posterosuperior tears demonstrated lower mean outcomes as compared with superior and anterosuperior. Labral tear location was also not found to significantly influence rates of Patient Acceptable Symptom State achievement. Satisfaction was similar among superior, anterosuperior, and posterosuperior tear locations. THA conversion occurred in 20.9% of patients and was not independently associated with tear location after adjusting for confounders. Age was the strongest predictor of THA conversion, and tear size was also significant.
Conclusion:
Acetabular labral tear location was not found to be a significant predictor of functional or clinical outcomes after hip arthroscopy. However, while labral tear location was not predictive of conversion to THA, age and tear size were significant predictors of conversion.
Acetabular labral tears are one of the most common causes of hip pain in young and middle-aged adults, with a prevalence of 57% in the general asymptomatic population and up to 80% of symptomatic patients with femoroacetabular impingement. 35 The acetabular labrum is a triangular fibrocartilage structure located circumferentially around the acetabular rim, and it acts as a seal around the femoral head, which increases mechanical stability while providing joint lubrication and increased load distribution.3,15 Tears in the acetabular labrum can compromise these normal functions, leading to increased pain levels, altered gait mechanics, and an increased risk for developing osteoarthritis.2,19,25
For patients who have failed nonoperative treatments, hip arthroscopy is the standard of care for definitive management of symptomatic acetabular labral tears. 30 Many studies have shown improvements in patient-reported outcome measures (PROMs) after hip arthroscopy. However, a subset of patients will still require subsequent conversion to total hip arthroplasty (THA), often attributed to osteoarthritis disease progression.17,30,36,37 Understanding which factors significantly influence patient outcomes and conversion to THA is crucial for optimizing patient selection and managing postoperative expectations.
Previous studies have identified several factors that indicate poor outcomes after hip arthroscopy for the treatment of labral tears, including older age, higher body mass index (BMI), presence of low back pain, and the presence and severity of osteoarthritis.7,9,20,34 Additionally, large labral tears have been shown to be independent predictors of outcomes after surgery; however, the impact of the location of labral tears has yet to be fully understood. 4 The acetabular labrum is also heterogeneous in structure, with the thickest portion in the superior and posterior regions and the widest in the anterior and superior regions. 27 This region-specific architecture of the acetabular labrum warrants further analysis to determine if certain regions are better suited to handle abnormal biomechanical forces, suggesting that injury patterns will have different impacts on outcomes after surgical treatment.
Under normal circumstances, the concavity of the femoral neck allows for the hip joint to be stressed in multiple planes without impingement of the labrum between the acetabulum and femoral neck, with areas of higher load transmitting larger shear forces to the labrum. 14 Most labral tears occur in the setting of femoroacetabular impingement. In patients with distortions of the femoral neck concavity, such as those seen with hypertrophic cam lesions, pistol grip deformities, or epiphysial growth anomalies, the labrum becomes impinged upon at the endpoints of certain motions. 14 Greater femoral anteversion, acetabular anteversion, and dysplasia increase the reliance on the labrum for support, resulting in a higher likelihood of tearing, most commonly in the superior and anterosuperior regions.14,15 Positions that place the hips in forced flexion and abduction, such as prolonged sitting on the ground, have been shown to increase the prevalence of posterior labral tears, although these are relatively uncommon. 14 These anatomic differences may translate into different patterns of healing and clinical outcomes.
Given the increasing utilization of hip arthroscopy for the treatment of acetabular labral tears, there is a need for long-term studies evaluating the relationship between labral tear location and clinical outcomes. 1 The purpose of this study is to investigate the long-term PROMs, rates of achieving clinically meaningful outcomes, overall patient satisfaction, and rates of conversion to THA after hip arthroscopy based on where the labral tear was located. Understanding these relationships provides further insight for patient counseling, surgical planning, and optimizing outcomes in hip arthroscopy.
Methods
Data Collection
This study protocol was approved by the institutional review board (2011P000053) with each patient providing consent. This retrospective study was conducted with patients undergoing hip arthroscopy for symptomatic labral tears by a single, high-volume orthopaedic sports medicine surgeon specializing in hip arthroscopy (S.D.M.), with >8 years of arthroscopic hip surgical experience before the first patient was included in this study. All patients with clinical findings indicative of femoroacetabular syndrome (ie, pain; limited range of motion of flexion, adduction, and internal rotation or flexion, abduction, and external rotation) underwent magnetic resonance imaging and at least 3 months of nonoperative therapy to include hip mobility and core-strengthening exercises. Patients whose symptoms did not decrease to a tolerable level were considered for hip arthroscopy. Patients were included if they underwent primary hip arthroscopy from 2002 to 2013, were aged ≥18 years at the time of surgery, and completed an emailed online survey with minimum 8-year follow-up from the index surgery. The surveys included the modified Harris Hip Score (mHHS), Non-arthritis Hip Score (NAHS), Lower Extremity Functional Scale, Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Specific Subscale (HOS-SSS), and International Hip Outcome Tool (iHOT-33), all of which are validated questionnaires to assess for hip symptom severity. Clinically meaningful outcomes were evaluated by rates of achieving the Patient Acceptable Symptom State (PASS) from previously established threshold values at 5 years.28,31 Overall patient satisfaction was assessed with a binary scale (satisfied vs not satisfied). Patients were considered satisfied if they responded “yes” on the survey to both of the following: (1) if they were happy with their outcomes and (2) if they would choose the procedure again knowing the outcomes. Data on conversion to THA, revision hip arthroscopy, and other secondary surgical procedures were collected through patient surveys and a manual chart review of each patient's electronic medical record.
Patient descriptive data, including age at the time of surgery, sex, BMI, race, and ethnicity, were collected from electronic medical records (Table 1). Preoperative radiographic parameters, including Tönnis grade, dysplasia, and type of femoroacetabular impingement (none, cam, pincer, or combined), were also evaluated from preoperative radiographs (Table 2).
Descriptive Characteristics of Study Population Based on Labral Tear Location a

Data are reported as mean ± SD or No. (%). Statistical analysis was performed by 1-way analysis of variance for continuous variables and Fisher exact test for categorical variables. Bold indicates P < .05. BMI, body mass index.
Clinical and Radiographic Characteristics of Study Population Based on Labral Tear Location a

Data are reported as mean ± SD or No. (%). Statistical analyses were performed by 1-way analysis of variance and Fisher exact test. Bold indicates P < .05. FAI, femoroacetabular impingement; LCEA, lateral center-edge angle.
Patients were excluded for the following: hip dysplasia defined as lateral center-edge angle ≤20° or acetabular inclination >45°, BMI ≥35 kg/m2, Tönnis grade ≥2, prior ipsilateral hip arthroscopy, concomitant procedures (eg, periacetabular osteotomy), inflammatory arthritis, avascular necrosis (including Legg-Calvé-Perthes disease), and slipped capital femoral epiphysis.
Tear Classification
Labral tear locations were classified intraoperatively using a clock-face method divided into 5 distinct areas based on the Beck classification system for acetabular cartilage defects (Figure 1). 23 While the Beck classification system originally used zones A to E, these were renamed posteroinferior, posterior, superior, anterior, and anteroinferior, respectively, for the purposes of our study. Tears spanning the posterior and superior regions were classified as posterosuperior, and tears spanning the superior and anterior regions were classified as anterosuperior. Tears spanning >2 consecutive anatomic regions (ie, posterosuperior to superior to anterosuperior) were excluded from the final analysis to minimize the effect of tear size, as tears spanning multiple regions will inherently be larger. Anterior, posterior, anteroinferior, and anterior-to-anteroinferior tears were also excluded for low sample sizes (Figure 2). Tear size was reported in degrees based on the clock-face Beck classification method, with 1 hour being equal to 30°.
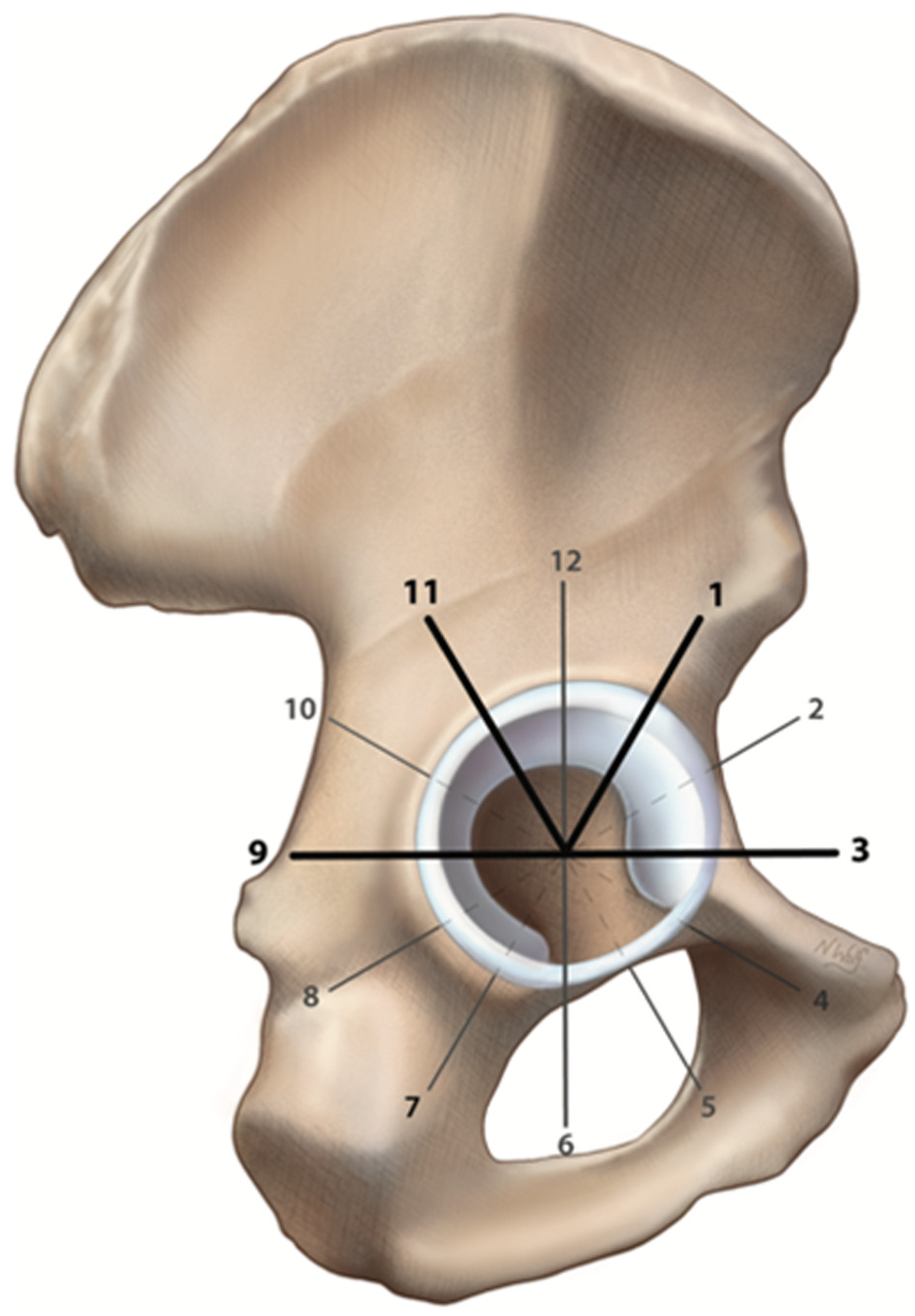
Locations of labral tears. Labral tear locations were extracted from patient operative reports using a clock-face naming convention: superior tears were from 10:00 to 2:00; anterosuperior tears, 12:00 to 3:00; and posterosuperior tears, 8:00 to 11:00. The same naming convention was used for left and right labral tears. Illustration by Nicole Wolf, MS, ©2025.

CONSORT flow diagram for patient selection. BMI, body mass index.
Abbreviated Surgical Technique
Each operation in this study was conducted by a single, fellowship-trained sports medicine orthopaedic surgeon (S.D.M.). For each procedure,10,11,29 patients were placed in the supine position on a hip distraction table (Smith & Nephew). Four arthroscopic portals were established: anterolateral, anterior, midanterior, and Dienst. 13 Labral debridement was performed if the labral tear was considered degenerative, hypoplastic, or isolated to a single anatomic plane involving <50% of the labrum. Labral repair was performed if there was sufficient healthy labral tissue for suture fixation or if the tear extended into the chondrolabral junction. Cam and pincer lesions were addressed with femoral neck osteoplasty, acetabular osteoplasty, or both.
Postoperative Protocol
After surgery, all patients without absolute contraindications were prescribed 81 mg of aspirin daily for 3 weeks for the prevention of deep vein thrombosis. All patients in our study followed the senior surgeon's studied and published 5-phase postoperative protocol. 26 The protocol consisted of patients initially ambulating with crutches while maintaining a flat-foot, stiff-leg gait on the operative side for 6 weeks after surgery. Patients were instructed to decrease abnormal stresses to the best of their abilities on the operative site without limping. After 6 weeks, patients could wean off crutches as tolerated and ride an indoor stationary bike. After 10 weeks, patients could advance to using an elliptical trainer and begin light swimming with the use of a buoy board between their legs. At the 4-month mark, patients could begin short-arc leg presses and hamstring curls. Once patients were 6 months out from surgery, they were permitted to gradually resume normal impact activities as tolerated. This protocol was designed to gradually increase motion without overloading the repair.
Statistical Analyses
All statistical analyses were performed in R software (Version 4.3.0; R Foundation for Statistical Computing). Continuous variables were reported as means with standard deviations, while categorical variables were presented as counts and percentages. Pairwise statistical comparisons for conversion to THA were performed with anterosuperior tears serving as the reference group, as this was the most common tear location in our study. For continuous variables such as PROMs, analysis of variance with a post hoc Tukey test and pairwise independent 2-tailed t tests were performed to compare means among groups. Categorical variables, such as conversion to THA and satisfaction, were analyzed by Fisher exact tests to account for smaller sample sizes. A sensitivity analysis was performed to compare satisfaction with PASS threshold achievement percentages. The relationship between tear location and THA conversion was evaluated by unadjusted and multivariable adjusted logistic regression models. The unadjusted analysis examined the crude association between tear location and THA conversion, while the multivariable model adjusted for age, tear size, and Tönnis grade. Odds ratios (ORs) with 95% confidence intervals were calculated, and statistical significance was set at P < .05 for all analyses. An a priori power analysis was performed to determine the minimum sample size needed to detect a minimal clinically important difference of 15.1 points in mHHS among tear location groups at 5 years (G*Power Version 3.1).27,30 Previous research from the senior author's prospective hip outcome registry demonstrated that mHHS had a standard deviation of 13. A difference in means of 11.4 points was considered the threshold for detecting a 5-year clinically meaningful difference in mHHS, based on previously published studies.27,30 Assuming these conditions, an alpha level of .05, and unequal distribution of patients across tear locations, a sample size of 12 patients in the posterosuperior and superior groups and 88 patients in the anterosuperior group will provide 80% power (1 –ß error probability).
Results
Patient Descriptive and Baseline Characteristics
Of the 513 patients who underwent hip arthroscopy during the study period, 166 returned completed surveys. Of these, 138 patients met inclusion criteria with a mean ± SD follow-up of 11.1 ± 2.5 years (range, 8.0-19.7 years). Three patients were excluded for a high BMI, 3 had Tönnis grade ≥2, 14 had labral tears spanning >2 anatomic regions, and 8 were excluded for low sample sizes (Figure 2). Patient descriptive and baseline characteristics are reported in Table 1. The mean age was 43.2 ± 11.3 years, with 67% of patients being female. The mean BMI was 26.4 ± 4.3 kg/m2 with a mean tear size of 52.1°± 25.3°. Anterosuperior tears were the most observed tears in our cohort (n = 103; 74.6%), followed by superior tears (n = 21; 15.2%) and posterosuperior tears (n = 14; 10.1%).
There was no significant difference in age among groups (P = .138), but there was a significantly higher percentage of female patients in the superior tear group as compared with the anterosuperior and posterosuperior tear groups (P = .006) (Table 1). No significant differences were observed in BMI among groups (P = .786). Follow-up time differed significantly among groups, as patients with superior tears had longer mean follow-up than patients with anterosuperior and posterosuperior tears (12.4, 10.9, and 11.3 years, respectively; P = .049).
Radiographic and Intraoperative Characteristics
Preoperative radiographic and intraoperative characteristics are summarized based on tear location in Table 2. All clinical and radiographic characteristics showed no significant differences among groups, except for labral tear size (P < .001). However, differences in labral tear size are unavoidable from the classification system used, owing to antero- and posterosuperior tears spanning 2 consecutive anatomic regions. In total, 114 patients (82.6%) had no radiographic evidence of hip arthritis and 24 (17.4%) had Tönnis grade 1. Patients were evenly distributed regarding their tear location (P = .377). No significant differences were noted in the presence and type of femoroacetabular impingement across tear locations (P = .259). An overall 76 patients (55.1%) underwent labral repair while 59 (42.8%) underwent labral debridement. There were no statistically significant differences in rates of labral debridements versus labral repairs for the 3 tear locations of interest (P = .059).
Functional Outcomes and PASS
Patients did not show any statistically significant difference in long-term mean outcomes across all PROMs based on tear location (Table 3). At final follow-up, mHHS scores were 80.6 ± 17.5 for posterosuperior tears, 88.3 ± 12.4 for anterosuperior, and 88.8 ± 12.7 for superior (P = .20). Similar patterns were observed for NAHS (P = .27), Lower Extremity Functional Scale (P = .14), HOS-ADL (P = .38), HOS-SSS (P = .17), and iHOT-33 (P = .15) at final follow-up. Similarly, PASS achievement did not differ significantly among tear locations for mHHS (71.4% for superior, 65.7% for anterosuperior, and 53.8% for posterosuperior, P = .575), NAHS (P = .933), HOS-ADL (P = .991), and iHOT-33 (P = .135).
Clinical Outcomes Based on Labral Tear Location a

Data are reported as mean ± SD or No. (%). Mean PROM values and percentage of patients achieving PASS are based on tear location. Statistical analysis was performed with 1-way analysis of variance for comparing mean PROMs and a Fisher exact test for PASS achievement. No significant differences were found among tear location groups (all P > .05). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SSS, Hip Outcome Score–Sports Specific Subscale; iHOT-33, International Hip Outcome Tool; LEFS, Lower Extremity Functional Scale; mHHS, modified Harris Hip Score; NAHS, Non-arthritis Hip Score; PASS, Patient Acceptable Symptom State; PROM, patient-reported outcome measure.
THA Conversion
The overall THA conversion rate was 20.3% (28/138 patients) with a mean time of 6.1 ± 4.6 years to conversion after initial hip arthroscopy. THA conversion rates were not significantly different across locations, with THA conversion rates of 23.3% (24/103) for anterosuperior tears, 21.4% (3/14) for posterosuperior tears, and 4.8% (1/21) for superior tears (P = .12). In the unadjusted logistic regression model, superior tears were 85.2% less likely to require conversion to THA (OR, 0.148; 95% CI, 0.008-0.767; P = .069) as compared with anterosuperior tears. While posterosuperior tears were 18.5% more likely to require conversion to THA, this was not statistically significant (OR, 1.185; 95% CI, 0.304-3.883; P = .789) versus anterosuperior tears.
In our multivariate model, the adjusted ORs showed notable changes from the unadjusted estimates (Table 4). After adjusting for age, tear size, and Tönnis grade, there was no difference in the odds of conversion to THA. For superior tears as compared with anterosuperior tears, the adjusted OR was 1.15 (95% CI, 0.14-11.17; P = .886), and for posterosuperior tears, the adjusted OR was 0.34 (95% CI, 0.04-2.14; P = .255). Age emerged as the strongest predictor, with each additional year of age at the time of surgery resulting in a 5.2% increased adjusted odds for conversion to THA (OR, 1.05; 95% CI, 1.01-1.1; P = .012). From this finding, a 10-year age difference would correspond to 66% higher odds in eventual conversion to THA. Additionally, tear size was an independent predictor of conversion to THA, with 5% increased odds for every additional degree in tear length (OR, 1.05; 95% CI, 1.02-1.09; P = .006). Tönnis grade was not a significant predictor for conversion to THA (OR, 2.27; 95% CI, 0.89-6.02; P = .086).
Odds Ratio of Conversion to THA a

Unadjusted and adjusted odds ratios with 95% confidence intervals comparing anterosuperior and posterosuperior tears against superior tears (reference group). Adjusted odds ratios account for age, tear size, and Tönnis grade. P values were calculated by multivariable logistic regression with statistical significance of P < .05. OR, odds ratio; THA, total hip arthroplasty.
Patient Satisfaction
The overall patient satisfaction rate in our study was 79.7% (110/138). Satisfaction across all groups was similar, with superior tears having the highest satisfaction at 81.0%, followed by anterosuperior at 80.6% and posterosuperior at 71.4% (P = .718) (Table 3). To assess the validity of using 5-year PASS thresholds at an extended follow-up, we performed a sensitivity analysis comparing PASS achievement rates with patient satisfaction. Overall, patient-reported satisfaction rates were 13.0 percentage points higher than their composite PASS achievement rates (77.7% vs 64.6%). This pattern was consistent across tear locations, with a 9.6–percentage point difference for superior tears (81.0% satisfaction vs 71.4% composite PASS), 15.8–percentage point difference for anterosuperior tears (80.6% vs 64.8%), and 13.7–percentage point difference for posterosuperior tears (71.4% vs 57.7%). Among individual PROMs, HOS-ADL demonstrated the closest alignment with satisfaction (mean difference, 7.8%), while iHOT-33 showed the largest disconnect (mean difference, 33.1%).
Discussion
Regarding labral tear location overall, there were no significant differences among patients in long-term PROMs, PASS achievement, conversion to THA, or patient satisfaction. These findings are promising as previous studies have reported that patients undergoing hip arthroscopy typically report significantly improved functional outcomes postoperatively, as well as minimal complication rates and high rates of survivorship.6,7,16,21,24 The present study, with a minimum 8-year follow-up, adds to the growing body of literature demonstrating significantly improved long-term outcomes for hip arthroscopy, finding overall satisfaction of roughly 80%. These results provide evidence that differences in labral tear locations should not be a contraindication for hip arthroscopy.
The major finding of this study was that patients with anterosuperior, superior, and posterosuperior tears all demonstrated similar postoperative PROM scores at a minimum 8-year follow-up, suggesting that anatomic tear location alone is not a reliable indicator of postoperative functional outcomes. This finding aligns with existing evidence in the broader orthopaedic literature demonstrating that anatomic variables often have limited correlation with functional outcomes. With regard to shoulder labral tears, Houck et al 18 performed a study of how tear location affects physical examination findings before surgery. They found that tear locations failed to show differences in minimal clinically important difference and were correlated with only small differences in range of motion. Additionally, meniscal tears showed no significant difference in outcomes after surgery in terms of tear patterns (horizontal vs radial) and tear locations (anterior horn, body, or posterior horn). 12
Recent long-term outcome studies have demonstrated the durability of hip arthroscopy beyond the midterm 2- to 5-year follow-up periods. In a 10-year retrospective study, Domb et al 8 found that 77.8% of patients met PASS for mHHS, 63.2% for NAHS, and 55.6% for HOS-SSS, consistent with the values described in our study. Additionally, these patients reported a 23.8% conversion to THA at a mean 41.5 months, highlighting the ability for arthroscopic labral repair to restore function and prevent or delay THA. 8 With our 8-year minimum and 11.1-year mean follow-up, these outcomes are valuable for establishing realistic long-term patient expectations and guiding surgical indications.
PASS achievement rates were similar among the cohorts, indicating that patients achieve relatively similar results after surgery for all tear locations included in this study. Given the retrospective nature of this study and the lack of preoperative PROMs, PASS achievement was one of the main outcomes in determining a successful improvement. While all tear location groups achieved >84% PASS achievement for HOS-ADL, rates for iHOT-33 had a wider range, at 31% for posterosuperior, 41% for anterosuperior, and 62% for superior. This variation in PASS rates across PROMs has been described in the literature, with a systematic review by Levy et al 22 finding that overall PASS after hip arthroscopy was 88% for mHHS but far harder to achieve for other scales, with only 25% and 30% of patients achieving PASS for HOS-ADL and HOS-SSS, respectively. Although our study found that more patients achieved PASS for HOS-ADL as compared with other PROM scales, it highlights the complexity of measuring outcomes in regard to which motions and activities show the most improvement after surgery. Additionally, from the sensitivity analysis, the consistently higher satisfaction relative to PASS achievement suggests that 5-year PASS thresholds may be too conservative at a minimum 8-year follow-up period, with patients self-reporting higher levels of satisfaction than the PASS thresholds across all studied PROMs.
Furthermore, labral tear location was not found to significantly influence conversion to THA rates; however, patient age at surgery was the strongest independent predictor of conversion to THA, with the odds of conversion to THA increasing by 5.2% for each additional year of age at index surgery. This trend is supported by other studies in the literature, as exemplified by an insurance database study by Tiao et al 33 that retrospectively studied 5048 patients and identified age and preexisting osteoarthritis as significant predictors of THA conversion; specifically, patients aged 41 to 50 years and those aged 51 to 60 years were >3 and 6.5 times more likely to undergo conversion to THA as compared with patients aged <40 years. Patients <40 years old had a low rate of conversion, with an overall THA conversion rate of 2.7%. A similar insurance database study by Schairer et al 32 found a similar trend, with patients <40 years old having significantly lower rates of conversion to THA as compared with patients aged 60 to 69 years. It also identified osteoarthritis and obesity as independent predictors of THA conversion; however, our study found no association with BMI and Tönnis grade, owing to patients with a BMI ≥35 kg/m2 and Tönnis grade ≥2 being excluded to control for potential confounders.
Anterosuperior tears were the most common acetabular labral tear observed in our cohort, as well as in the broader literature. 15 Superior and anterosuperior labral tears are commonly caused by forces transmitted because of the physiologic anterior orientation of the acetabulum combined with anteversion of the femur. 14 Given the anatomic location of cam and pincer lesions, the superior and anterosuperior labrum is impinged with the hip in flexion, further increasing the incidence of tears in these regions. 5 Additionally, posterior and posterosuperior tears tend to occur in the setting of forced extension and external rotation caused by trauma, which is one potential reason for the 10% incidence of these tears in our study. 14
Limitations
As this is a retrospective study, there are inherent limitations with the potential for response bias, with 32.4% (166/513) of eligible patients returning completed surveys, but we attempted to minimize within-group confounding through multivariable regression models, although selection bias from differential response rates cannot be fully addressed through statistical adjustment. Another inherent limitation is that we did not have access to baseline PROMs, making it difficult to assess patient improvement. Additionally, there was a small number of patients in the posterosuperior tear cohort. Although this is expected since posterosuperior tears are relatively uncommon in the general population, the sample size limited our statistical power and ability to draw conclusions for this group, highlighting the need for further prospective studies. Studies have also shown interrater reliability for the location of acetabular labral tears to be quite low, which could limit the generalizability of this study; however, all classifications of labral tear location were performed by a single surgeon. 10 Finally, all operations were done by a single surgeon within a single institution, with all patients following a specific postoperative protocol, which can also limit the generalizability of findings.
Conclusion
Acetabular labral tear location was not a significant predictor of functional or clinical outcomes after hip arthroscopy. However, while labral tear location was not predictive of conversion to THA, age and tear size were significant predictors of conversion. Overall, the location of a labral tear is not a predictor of long-term results after hip arthroscopy.
Footnotes
Acknowledgements
The authors thank the Conine Family Fund for Joint Preservation for its continued research support.
Final revision submitted January 7, 2026; accepted February 13, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Brigham and Women's Hospital Institutional Review Board (2011P000053).