
Abstract
Background:
In pediatric anterior cruciate ligament reconstruction (ACLR), there exists a potential to injure the open physis in skeletally immature patients and cause growth disturbance. Thus, there is a need to determine the optimal ACLR technique for this population.
Purpose:
To evaluate the functional outcomes and rates of physeal disturbance, graft failure, and reoperation after transphyseal and physeal-protecting techniques—including extraphyseal intra-articular and partial epiphyseal ACLR—within the skeletally immature population.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients who underwent primary ACLR from June 2018 to April 2023 at a tertiary pediatric hospital were identified. The exclusion criteria included skeletal maturity based on preoperative magnetic resonance imaging, concomitant multi-ligamentous injury, excluding medial collateral ligament sprain that did not require surgical intervention, and <6 months of follow-up. Descriptive, injury, and surgical data; clinical outcomes; and complications were analyzed using the chi-square and Kruskal-Wallis tests. Growth disturbance was assessed using pre- and postoperative standing hip-to-ankle films.
Results:
A total of 87 patients met the study inclusion criteria. A total of 41 (47.1%) patients underwent transphyseal (mean age, 15.2 ± 0.9), 34 (39.1%) underwent extraphyseal intra-articular (12.9 ± 1.7), and 12 (13.8%) underwent partial epiphyseal (14.6 ± 1.2) ACLR. The transphyseal group was significantly older in chronological and skeletal age (P < .001). Autograft types varied significantly across cohorts (P < .001). The partial epiphyseal technique had the highest rate of complications (50%; P = .009), most commonly stiffness (n = 2) and ACL retear (n = 2). Four (4.6%) patients experienced unilateral growth disturbance, with 1 in the extraphyseal intra-articular group. Angular growth disturbance ranged from 3° to 5º of valgus. There were no cases of leg length discrepancy or growth arrest.
Conclusion:
Comparable angular growth disturbance and retear rates were observed across all 3 ACLR techniques in skeletally immature patients, suggesting acceptable outcomes with appropriate surgical technique.
Keywords
Anterior cruciate ligament (ACL) injuries in the pediatric population continue to rise,13,27,37 with the incidence of ACL tears increasing 2.3% annually between 1993 and 2013. 5 Compared with skeletally mature patients, reconstructive surgery to manage ACL injury in skeletally immature patients must account for and protect the open physes. Traditional ACL reconstruction (ACLR) in skeletally mature individuals cannot be easily translated to skeletally immature individuals due to the risk of damage to the distal femoral or proximal tibial physis, which may lead to subsequent growth arrest, leg-length discrepancies (LLD), and angular deformities. 25 Optimal management of ACL injuries in the skeletally immature individual is necessary to minimize these complications.
Historically, pediatric ACL injuries were managed conservatively with activity modification, bracing, and physiotherapy to avoid iatrogenic injury to the physis. 12 However, nonoperative or delayed management often leads to further cartilage damage, secondary meniscal injury, premature knee degeneration, and instability. 35 As a result, early surgical management is now recommended in pediatric ACL tears. Many surgical techniques that avoid or protect the physis have been described—including extraphyseal, intra-articular, and all-or-partial epiphyseal techniques.7,11,17,24,26 Extraphyseal intra-articular ACLR, typically using an iliotibial band autograft, was described by Kocher et al 24 based on a modified Macintosh technique.1,26 In this technique, the physes are avoided by passing the graft “over the top” on the femoral side and under the intermeniscal ligament with fixation to the periosteum of the proximal tibia distal to the physis, without drilling tunnels. All-epiphyseal techniques2,11,17,22 spare the physis by passing the graft only within the epiphysis, while partial epiphyseal/partial transphyseal reconstruction techniques avoid crossing the distal femoral physis but cross the proximal tibia physis.3,6,18 Transphyseal ACLR techniques are the gold standard for skeletally mature patients. This technique has been described in skeletally immature patients but is generally reserved for those with limited growth remaining.4,14,34
While there is a low reported risk of growth disturbance across ACLR techniques, the literature shows a high degree of variability in assessing growth disturbance.10,15,33 A recent systematic review of the literature found that in studies reporting on growth disturbance after ACLR in pediatric patients, only 28% of studies assessed skeletal age, and only 12% obtained a preoperative hip-to-ankle standing alignment film. 15 Similarly, Collins et al 10 concluded that the true incidence of growth disturbance is likely underreported or inadequately assessed.
Few studies compare the different physeal sparing or protecting techniques with respect to rates and types of growth disturbance. This study aimed to evaluate the occurrence of growth disruption, functional outcomes, graft failure, and reoperation rates after transphyseal, partial epiphyseal, and physeal-sparing ACLR techniques in a skeletally immature population. We hypothesized that the transphyseal technique would pose a higher risk of growth disturbance than physeal-protecting techniques in the skeletally immature population.
Methods
Patient Selection
Following institutional review board approval, a retrospective chart review was performed of pediatric patients (age, 0-17 years) who underwent ACLR at a single tertiary pediatric care facility between June 2018 and April 2023. Patients were stratified by ACLR technique. All patients underwent autograft ACLR using either a hamstring (HS), iliotibial band, or soft tissue quadriceps tendon autograft. Patients deemed to be skeletally mature on preoperative magnetic resonance imaging (MRI), those with a concomitant multiligamentous injury—except concomitant medial collateral ligament (MCL) sprain not requiring surgical treatment—patients without postoperative imaging, or <6 months of follow-up were excluded (Figure 1).

Patient inclusion and exclusion pathway. ACLR, anterior cruciate ligament reconstruction; MCL, medial collateral ligament.
Variables Collected
Patient characteristics were collected—including chronological and skeletal age, sex, date of injury, mechanism of injury, and sports participation.
Preoperative MRI was reviewed in all patients to confirm ACL injury as well as open physeal status. Skeletal age was determined using preoperative single-view hand radiographs, with an associated radiologist’s report noting bone age according to the standards of Gilsanz and Ratib. 16 Pre- and postoperative LLD (uninjured minus injured leg length), mechanical axis deviation (MAD), mechanical tibiofemoral angle (mTFA), mechanical lateral distal femoral angle (mLDFA), and mechanical medial proximal tibial angle (mMPTA) were measured on hip-to-ankle standing films. These measurements were obtained using methods that ensured both intra- and interrater reliability. Two independent raters, (A.K., medical student, and E.L.N., attending orthopaedic surgeon), completed measurements 2 weeks apart. Figure 2 demonstrates the method of measurement for mTFA, MAD, mLDFA, and mMPTA utilized in this study. Hip-to-ankle standing films were typically obtained at 6 months, 1 year, and 2 years, but possibly more frequently if there was concern for an evolving growth disturbance. The radiograph taken at the patient’s latest follow-up was used to compare pre- and postoperative LLD and alignment.

Measurements collected from pre- and postoperative imaging. MAD, mechanical axis deviation; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle; mTFA, mechanical tibiofemoral angle.
Surgical variables included surgical reconstruction technique, graft type used, concomitant intra-articular pathology, and whether these concomitant injuries were surgically addressed. Technique selection was at the surgeon’s discretion (94% performed by a single surgeon, E.L.N.) and was primarily guided by the status of the physes on preoperative MRI. In general, physeal-sparing techniques (extraphyseal, intra-articular, and partial epiphyseal) were favored for younger patients with substantial growth remaining. In comparison, transphyseal reconstruction was selected for older patients nearing skeletal maturity.
We collected postoperative final passive range of motion, Lachman test, and ability and time to return to sports (RTS). Patient-reported outcomes (PROs), including the Anterior Cruciate Ligament-Return to Sport after Injury (ACL-RSI) score and Pediatric International Knee Documentation Committee (Pedi-IKDC) score, were collected postoperatively. Outcomes were collected at the latest follow-up for each patient. Complication rates—including ACL retear, return to the operating room, meniscal retear, infection, knee stiffness, and growth disturbance—were collected from chart review of postoperative clinic visits. Growth disturbance was defined as a change in the MAD on the operated knee or a change in LLD >5 mm between pre- and postoperative films.
Statistical Analysis
The nonparametric Kruskal-Wallis test was utilized to analyze continuous variables. Pearson’s chi-square test was used for categorical and binary data. P < .05 was statistically significant, and all analyses were done using R statistical software, Version 4.0.06 (R Foundation for Statistical Computing). 31
Results
Patient Characteristics
A total of 259 pediatric patients who underwent ACLR were initially identified; 87 met the inclusion criteria. The mean chronological age of the cohort was 13.9 ± 1.8 years. A total of 56 (64.3%) patients had preoperative bone age radiographs with a mean skeletal age of 14.2 ± 1.7 years. Also, 61 (70.1%) patients were male, and 26 (29.9%) were female. Also, 73 (83.9%) of all ACL tears were reported as sports-related injuries. In patients with sports-related injuries, the most common sports were soccer (27 patients, 31%), football (21 patients, 24.1%), and basketball (14 patients, 16.1%). Full patient characteristics are presented in Table 1.
Patient Characteristics and ACLR Details a

Data are presented as mean ± SD or n (%). Bold indicates statistical significance. ACLR, anterior cruciate ligament reconstruction; HS, hamstring; ITB, iliotibial band; NR, not reported; STQT, soft tissue quadricep tendon.
Extraphyseal intra-articular.
Surgical Data
A total of 41 (47.1%) patients underwent transphyseal ACLR, with 22 (53.7%) receiving a hamstring autograft and 19 (46.3%) receiving a quadriceps autograft. A total of 34 patients (39.1%) underwent extraphyseal intra-articular ACLR, and all (100%) received an IT band autograft. Twelve (13.8%) patients underwent partial epiphyseal reconstruction, with 6 (50%) receiving a hamstring and 6 (50%) receiving a quadriceps autograft (Table 1). Also, 58 (66.7%) patients had ≥1 concomitant intra-articular pathologies—including lateral meniscal tear (n = 40; 46%), medial meniscal tear (n = 27; 31%), chondral injury (n = 3; 3.4%), and MCL sprain (n = 1; 1.1%). All concomitant injuries were treated during the same operation in which the ACLR was performed, except for the MCL sprain, which did not require surgical treatment.
Postoperative Outcomes
The mean postoperative follow-up was 24.1 months, and the mean chronological age at the final follow-up was 15.9 ± 2.03 years. Final full-length postoperative radiographs were obtained at 17.5 ± 9.7 months after ACLR. No statistically significant differences were found between the technique subgroups in time to RTS, with a mean time of 11.8 months and a mean rate of 85.1%. When comparing PROs, no statistically significant differences in ACL-RSI and Pedi-IKDC scores were detected between surgical techniques at 9 months postoperative (Table 2). The collective average 9-month ACL-RSI score was 89.2, and the average 9-month Pedi-IKDC score was 95.4.
Postoperative Outcomes and Patient PROs After ACLR a

Data are presented as mean ± SD, n (%), or median [IQR]. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, anterior cruciate ligament-return to sport after injury; NR, not reported; Pedi-IKDC, Pediatric International Knee Documentation Committee; PRO, patient-reported outcome; RTS, return to sport.
Extraphyseal intra-articular.
Complications
Sixteen patients (18.4%) experienced a complication within the overall cohort (Table 3). Complications included unilateral growth disturbance (4 patients, 4.6%), ACL retear (4 patients, 4.6%), meniscal retear (4 patients, 4.6%), postoperative stiffness (2 patients, 2.3%), and infection (1 patient, 1.1%). The partial epiphyseal ACLR group had a significantly higher rate of complications (50%; P = .003) compared with transphyseal ACLR (12.2%) and extraphyseal intra-articular ACLR (14.7%).
Complications After ACLR in Skeletally Immature Patients a

Data are presented as n (%). Bold indicates statistical significance. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; OR, operating room.
Extraphyseal intra-articular.
There were 4 unilateral growth disturbances: 1 patient in the transphyseal group, 1 in the extraphyseal intra-articular group, and 2 in the partial epiphyseal group (Table 4). All had angular deformities, with 4 exhibiting increased valgus angulation (3°-5°) and none exhibiting increased varus angulation. Two patients had growth disturbances involving the distal femur and proximal tibia, and 2 had growth disturbances involving only the distal femur. None of these patients underwent subsequent surgery to correct angular deformity. No cases of LLD between the operated and nonoperated limbs occurred after surgery. Three patients with extraphyseal ACLR had bilateral symmetrical growth disturbances that were not attributable to the ACLR. One patient with symmetric bilateral deformity underwent subsequent surgical intervention with guided growth to correct bilateral valgus (Figure 3).
Comparison of Patients Who Experienced Growth Disturbance After ACLR a
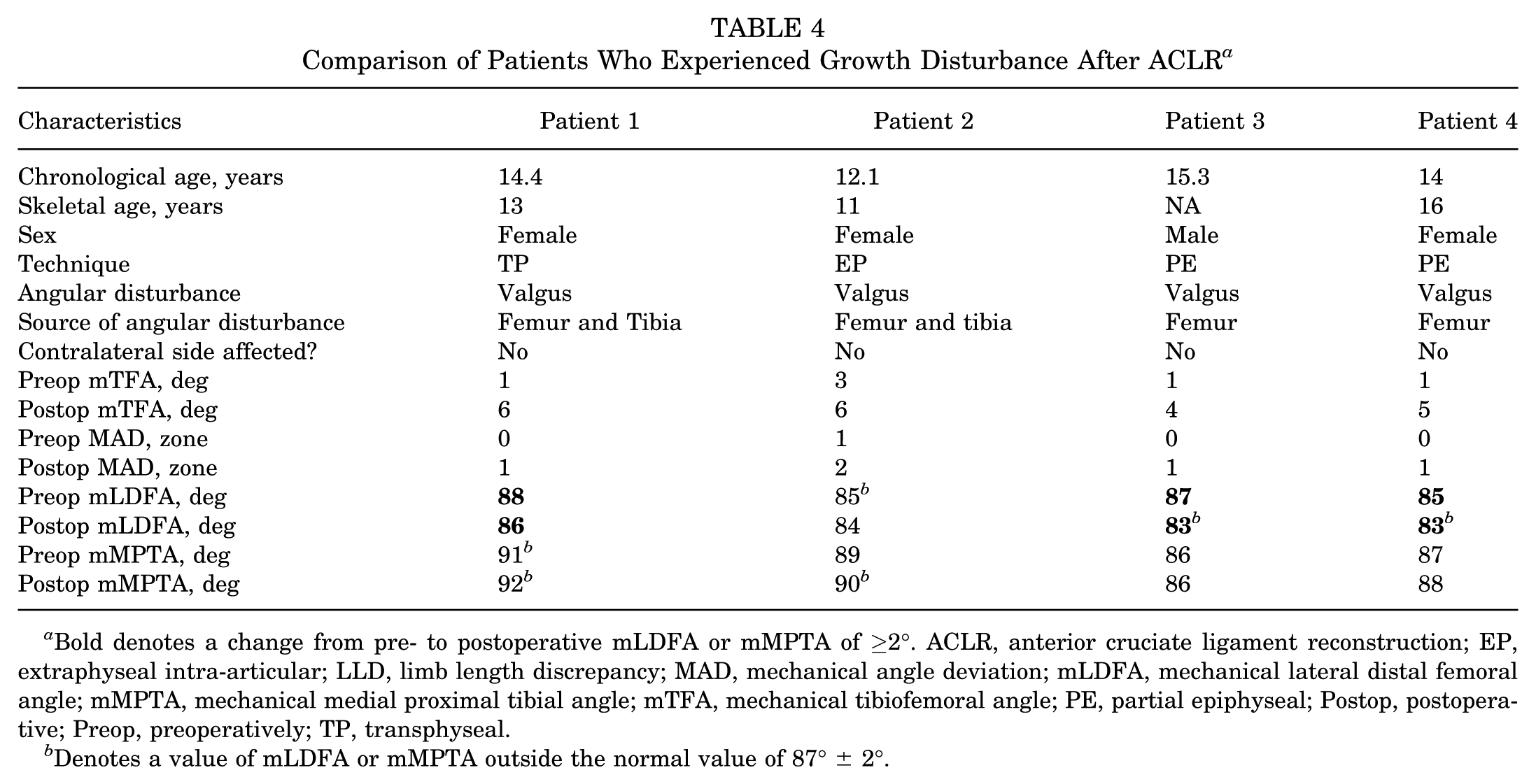
Bold denotes a change from pre- to postoperative mLDFA or mMPTA of ≥2°. ACLR, anterior cruciate ligament reconstruction; EP, extraphyseal intra-articular; LLD, limb length discrepancy; MAD, mechanical angle deviation; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle; mTFA, mechanical tibiofemoral angle; PE, partial epiphyseal; Postop, postoperative; Preop, preoperatively; TP, transphyseal.
Denotes a value of mLDFA or mMPTA outside the normal value of 87°± 2°.
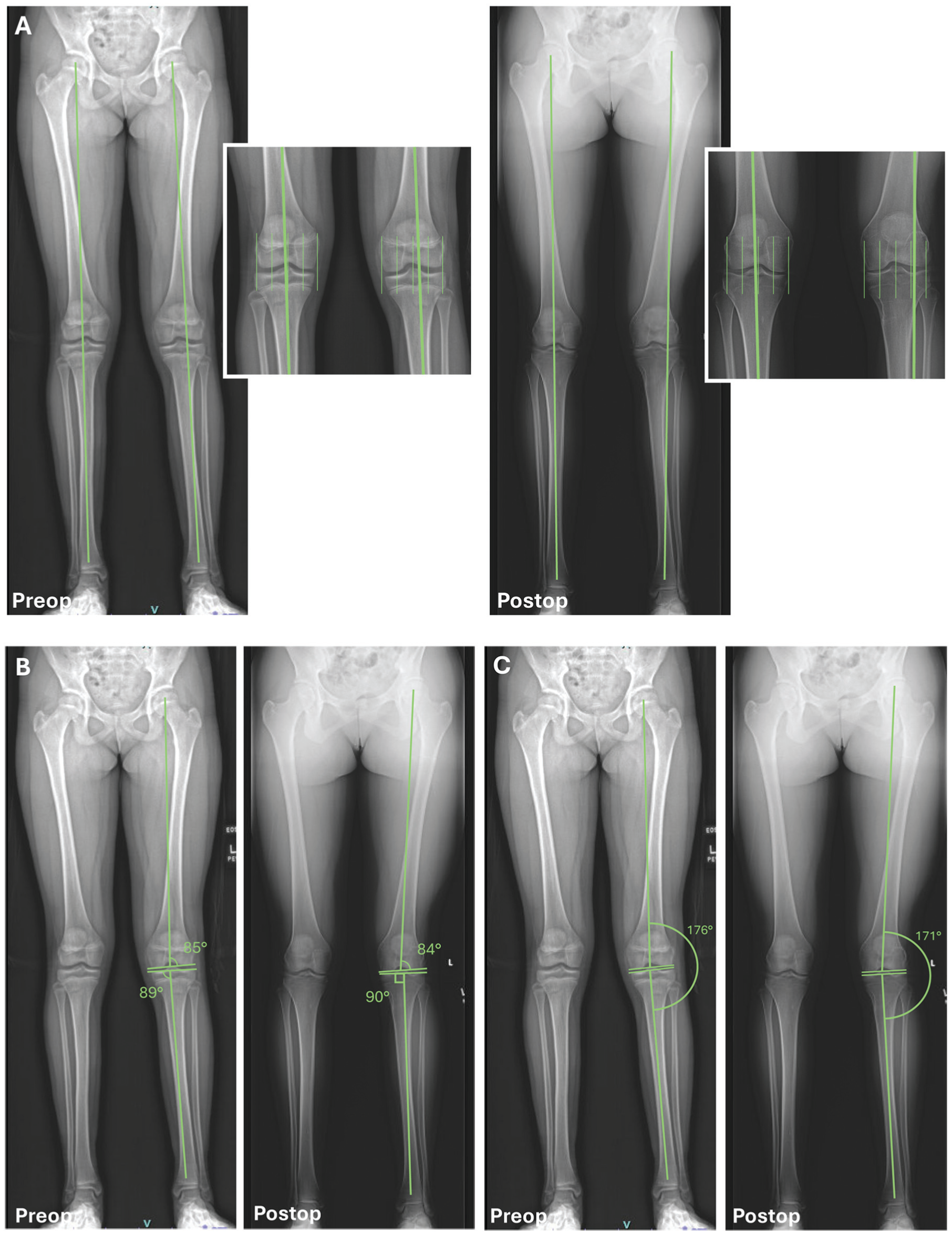
Patient 5 pre- and postoperative films with relative measurements. The patient had left knee reconstruction at age 13.1 years (skeletal age, 12 years) via the EP technique. Postoperative alignment films taken 12 months postoperatively. Note skeletal maturity at the time of the final postoperative film. (A) MAD zone 1 valgus preoperatively and zone 2 valgus postoperatively. (B) The LDA and MPTA were 85° and 89°, respectively, preoperatively, and 84° and 90°, respectively, postoperatively. (C) Hip knee ankle angle (HKA) was 4° valgus (176°) preoperatively, and 9° valgus (171°) postoperatively. LAD, lateral distal femoral angle; MAD, mechanical angle deviation; mLDFA, mechanical lateral distal femoral angle; mMPTA, mechanical medial proximal tibial angle; MPTA, medial proximal tibial angle; mTFA, mechanical tibiofemoral angle; PE, partial epiphyseal.
Discussion
The optimal surgical technique to maximize postoperative function while minimizing complications—including growth disturbance in skeletally immature patients undergoing ACL reconstruction—is an area of ongoing research and debate. Our study compares the rates of growth disturbance and overall outcomes across 3 commonly used techniques in pediatric and adolescent patients.
We found 4 cases of growth disturbance, with 2 in the partial extraphyseal group, 1 in the extraphyseal intra-articular group, and 1 in the transphyseal group. There was no significant difference in the rates of growth disturbances between the techniques. While growth disturbances after ACLR are concerning, they may not be clinically relevant. All 4 growth disturbances resulted in increased valgus angulation, with none exceeding 5°, none requiring surgical intervention, and none causing LLD. No significant differences in PROs were found between the techniques.
Growth arrest is a concern with the standard transphyseal technique because drilling through the physis may result in damage, leading to complete growth arrest, overgrowth due to subsequent hypervascularization, or undergrowth due to excessive graft tension across the physis.9,14,28,29 These disturbances may lead to iatrogenic LLD and angular deformities. However, Yoo et al 39 demonstrated that physeal disruptions on MRI may not result in clinically apparent growth disturbances. Although transphyseal reconstructions are thought to carry the greatest risk of growth disturbance, Holwein et al 19 demonstrated that transphyseal ACLR can be performed with a low risk of growth changes. Volumetric damage to the physis can be minimized by using smaller tunnel diameters, avoiding high-speed drilling, and placing tunnels more vertically across the physis. 21 We found a low rate of growth disturbance after transphyseal ACLR. However, the transphyseal group in this study was significantly older in chronological and skeletal age than the other technique groups, reflecting surgeon bias in technique selection based on the patient’s remaining growth potential. This technique was likely reserved for the subset of patients with limited growth remaining to minimize the risk of growth disturbance. It is possible that this set of patients had minimal remaining growth, and any damage to the physis was unlikely to result in clinically significant deformities.
The partial epiphyseal technique with an all-epiphyseal femoral tunnel and transphyseal tibial tunnel was developed to avoid growth disturbances in skeletally immature patients while preserving an anatomic femoral footprint. This was demonstrated by Willson et al 38 to result in minimal growth disturbances and low morbidity. However, in a case series by Chambers et al, 8 a total of 24 patients undergoing a partial epiphyseal ACLR were found to have a 25% reoperation rate, an 8.3% graft failure rate, and a 20% growth disturbance rate. Specifically, Chambers et al 8 found that in the subset of patients with >5 years of growth remaining, the rate of growth disturbance was 66.7%. This suggests a risk to the physis despite the use of a physeal-protecting surgical technique. Similarly, in a systematic review by Knapik and Voos, 23 the authors found that all-inside, all-epiphyseal reconstructions resulted in more growth disturbances leading to LLD (20/164; 12%) than extraphyseal reconstructions (2/256; 0.8%). They reasoned that, despite not crossing the physis, thermal damage from drilling near the physis led to growth arrest. 23 In a systematic review by Patil et al, 30 the combination of a transphyseal tibial tunnel with an epiphyseal femoral tunnel was found to yield the most growth disturbances (3.7%) compared with other techniques. Our results also showed that growth disturbance occurred with the partial epiphyseal technique (16.7%). This occurred despite reserving this technique for a slightly older age group, with a mean skeletal age of 14.5 years. We theorize that the same reasons as those of Knapik and Voos 23 explain the growth disturbances.
The extraphyseal-intra-articular technique resulted in 1 of the 4 growth disturbances observed in this study. We were unable to find any reports of growth disturbances after extraphyseal intra-articular ACLR in the skeletally immature population. In the systematic review by Patil et al, 30 among 82 extraphyseal procedures, zero growth disturbances were reported. In the systematic review by Knapik and Voos, 23 two cases of growth disturbance were reported after extraphyseal femoral and transphyseal tibia graft passage. One growth disturbance was a genu valgum angular deformity, and the other was a limb-length discrepancy, with the operative limb longer. These were described by Chotel et al 9 as overgrowth phenomena involving both the femur and the tibia. The authors also noted that the risk of overgrowth appears higher in younger patients and that the theoretical risk of overgrowth exists with all surgical techniques. 9 Undergrowth is also possible with extraphyseal reconstructions, highlighting the importance of avoiding excessive graft tension. 30 In our extraphyseal intra-articular cohort, one case of growth disturbance occurred, resulting in valgus deformity and stemming from both the distal femur and proximal tibia, suggesting that both undergrowth at the lateral distal femur and overgrowth at the medial proximal tibia occurred. Additionally, 3 cases of symmetric bilateral growth disturbance occurred in the extraphyseal group and could not be attributed to ACLR alone; these cases were excluded from our analysis. Interestingly, 2 of the 3 cases developed bilateral genu varum after ACLR. While the pathophysiology of this is unclear, the development of bilateral deformity may be reflective of the younger age and larger growth potential of this cohort.
Angular deformities after ACLR result from localized disturbances at the periphery of the physis, whereas central disturbances more likely result in nonangular LLD. 30 Overall, valgus deformities are more commonly reported compared with varus deformities and are thought to be more frequently associated with a lateral distal femoral origin of physeal disturbance.20,30,36 This disturbance can occur even with techniques that avoid crossing the physis and are thought to result from thermal damage in the all-epiphyseal technique, disruption of posterolateral perichondral structures in the “over the top” extraphyseal technique, or eccentric traction of the graft, causing rotational deformity. 32 In our study, valgus deformity occurred in all 4 growth disturbances, and at least 1 occurred in each of the 3 techniques we evaluated.
Despite the significant theoretical concerns regarding physeal injury and growth disturbance, Collins et al 10 asserted that growth abnormalities after ACLR in skeletally immature patients are underreported. In a review by Fury et al, 15 the authors note that although subsequent systematic reviews have identified more growth disturbances, the literature remains inconsistent, and consensus on growth monitoring and reporting is lacking. Previous studies vary in the thresholds set for clinical significance, the type of disturbance reported, and the methods used to determine growth disturbance, whether defined by radiographic measurements, clinical assessment, or both. In our study, growth disturbance was measured using hip-to-ankle standing radiographs, and postoperative images were compared with preoperative images. This ensured that reported LLD or angular deformity on the operative knee occurred or worsened after surgery.
Limitations
Limitations of this study are inherent to its retrospective nature and reliance on provider notes for postoperative outcome data; therefore, data and imaging were collected at varying time intervals. Specifically, 6 months was used as our minimum follow-up threshold because this was the earliest timeframe in which a postoperative hip-to-ankle standing radiograph was obtained. We acknowledge that this limitation may underestimate the true rate of growth disturbance in this cohort. However, most of our patients (88.5%) had a follow-up of >1 year. The surgeries were performed at a single institution, and a single surgeon performed the majority (94%) of procedures. This leads to smaller cohort numbers, particularly in the partial epiphyseal group. The technique used for each patient was at the surgeon’s discretion, leading to age differences between the technique groups. While this discrepancy is expected, given the preference for physeal-protecting techniques in younger patients, it also serves as a potential confounding variable when comparing outcomes and growth disturbance rates, possibly limiting the generalizability of this study. Additionally, skeletal maturity was not confirmed in all patients at the final follow-up. Longer, consistent follow-up times are needed to determine long-term postoperative functional outcomes and to ensure follow-up of patients through skeletal maturity, to ensure no growth disturbances are missed. While skeletal age was collected, additional analysis of predicted remaining growth may be useful in future studies investigating the risk of growth disturbance in ACLR. Finally, the cohort size of 87 limited the ability to perform a pre hoc power analysis. Future studies with larger sample sizes are needed to more rigorously assess statistical significance.
Conclusion
Injury to the physis is a concern in pediatric ACLR, and various techniques have been developed to mitigate that risk. Comparable growth disturbance and retear rates were found between all techniques for ACLR in skeletally immature patients, including physeal sparing techniques, suggesting acceptable outcomes with appropriate application of surgical techniques.
Footnotes
Final revision submitted January 31, 2026; accepted February 10, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Children’s National Hospital (IRB: STUDY00000661).
This paper was presented at the American Academy of Orthopedic Surgeons in March 2025 and as an E-poster at the Arthroscopy Association of North America in May 2025.