
Abstract
Background:
Despite excellent midterm clinical outcomes in several studies of pediatric anterior cruciate ligament (ACL) treatment, the modified McIntosh ACL reconstruction (ACLR) with iliotibial band (ITB) autograft (ITB ACLR) has been referred to as “nonanatomic” in nature. Moreover, the technique remains underinvestigated in terms of postoperative lower extremity recovery, strength, balance metrics, and hop tests, with little evidence on the effect of time from surgery.
Purpose:
To assess performance parameters between ITB ACLR and contralateral noninjured knees of patients who underwent the procedure at various time points before testing.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent ITB ACLR between 1 and 20 years before study initiation were identified from the surgical database of 3 high-volume ACL surgeons at a tertiary care pediatric hospital. Each patient in the cohort, which was randomly selected to achieve a broad distribution of times from surgery, participated in isometric strength tests (quadriceps, hamstring, and hip abductor), dynamic Y-balance tests, and functional hop tests. The limb symmetry index (LSI) was utilized for comparisons between knees, with equivalence and correlation analyses performed. Patient-reported outcomes (Pediatric International Knee Documentation Committee [Pedi-IKDC] form) and activity level (Hospital for Special Surgery Pediatric Functional Activity Brief Scale [HSS Pedi-FABS]) were recorded on the day of testing.
Results:
A total of 40 patients (9 in 1 to <2 years, 13 in 2 to <5 years, 10 in 5 to 10 years, and 8 in >10 years after ACLR) were enrolled. The mean time at which testing was completed was 5.8 years (SD, 4.8 years; range, 1.1-17.2 years) postoperatively. The mean Pedi-IKDC score was 95.9 (SD, 4.9), and the mean HSS Pedi-FABS score was 22.2 (SD, 6.0). When comparing the operative limb to the contralateral limb, the mean LSI for the single-leg hop test was 100.8% (SD, 13%) and that for the dynamic Y-balance test was 98.4% (SD, 4.8%). Of the strength tests, no significant differences were seen in mean strength testing for the hip abductor (LSI, 97.9%; P = .207), quadriceps (LSI, 97.9%; P = .260), or hamstring (LSI, 102.6%; P = .264). Equivalence analysis confirmed equivalency between limbs for all measures (all P < .05). No correlation between scores and time from reconstruction was observed, other than improvement in hip abductor LSI (r = 1.1; P = .027) and decline in HSS Pedi-FABS scores (r = −0.37; P = .019) with increasing time from surgery.
Conclusion:
Lower extremity strength and functional testing after ITB ACLR demonstrates equivalence or minimal (<3%) variation when comparing ACLR and contralateral noninjured limbs, with functional outcome scores in both short- and long-term follow-up. These findings suggest no discernible performance-based or functional perturbations or adverse effects from the nonanatomic features of ITB ACLR performed in children, even as they age into the skeletally mature and adult years of life.
Several decades ago, anterior cruciate ligament (ACL) tears in the pediatric population were considered extremely rare. Nevertheless, several authors recognized that ACL deficiency in this younger, active population, even with conscientious attempts at activity modification, use of protective bracing, and physical therapy exercises designed to optimize the dynamic stability of the knee, was associated with persistent knee instability episodes.2,12,14,20-24 Such episodes not only limited normal sports participation, but also affected activities of daily living and led to meniscal and chondral injuries, thereby increasing arthritis risk for such patients at alarmingly young ages. To combat these risks, pediatric ACL reconstruction (ACLR) techniques were developed that were designed to provide translational and rotational stability for the knee while also avoiding injury to the proximal tibial and distal femoral physes. As a growing number of reports have indicated that ACL injuries in the pediatric population are steadily increasing,9,29 enhancing our understanding of these reconstruction techniques, and their implications for long-term knee function, has become all the more important for orthopaedic and sports medicine caregivers.
Among the earliest stabilization techniques proposed for children with ACL deficiency was a combined extra-articular and intra-articular physeal-sparing procedure using a segment of the iliotibial band (ITB) as an autograft. Lyle Micheli developed this surgery in 1976 as a modification of the purely extra-articular ITB ACLR popularized by Galway and McIntosh 11 in 1972. The technique includes leaving the distal attachment of the ITB to the tubercle of Gerdy intact, while releasing the central 50% to 90% of the tendon proximally in the midthigh region and tubularizing the free end. Unlike the McIntosh technique, which looped the ITB graft around the LCL proximally and reattached it distally on the tibia, the modified McIntosh technique involved advancing the free end through an aperture in the posterolateral capsule, through the intercondylar notch, under the intermeniscal ligament and out a second capsular aperture on the anteromedial tibia. Through use of suture fixation of the tensioned graft on the posterolateral capsule, the more proximal limb of the graft serves as an extra-articular anterolateral rotational stabilizer, similar to the anterolateral ligament (ALL).7,16,30,38 Just distal to the physis, seating the graft in 2-to 3-mm deep bony troughs in both the intra-articular tibial epiphysis and extra-articular tibial metaphysis is the next step. After that, suturing the tensioned graft to the periosteum adjacent to the metaphyseal trough, the more distal limb of the graft, originating just posterior to the femoral ACL footprint and healing at the anterior aspect of the tibial ACL footprint, follows. This provides translational and additional rotational stability, similar to the construct of the more conventional intra-articular ACLR. The first published report of the procedure appeared in 1999, 21 after having been utilized routinely in the 1980s and 1990s at the study institution and other centers for prepubertal children with complete ACL tears or ACL deficiency.
Several clinical follow-up studies on cohorts of skeletally immature athletes who had undergone ITB ACLR, at both the institution at which the procedure was devised17,18 and other institutions, 40 have indicated that the procedure provides high rates of objective and subjective knee stability, good functional outcome measures, high rates of return to sports, high activity levels, and low rates of retear and other complications. Perhaps most notably, while case reports of limb overgrowth have appeared, 6 clinically concerning rates of growth disturbance associated with the technique are absent from the literature. Despite the favorable level 4 clinical reports, there remains some criticism of the technique, based on the nonanatomic graft construct and a lack of follow-up studies. Moreover, biomechanical studies have suggested that ITB ACLR is superior to other pediatric ACLR techniques in its ability to stabilize anteroposterior translation,15,28 limit rotational torque forces, and withstand the pivot-shift phenomenon. However, these biomechanical studies were performed on cadaveric specimens with fixation techniques quite different from the periosteal suture-based fixation applied in a growing child. Therefore, the technique remains grossly underinvestigated in terms of the true ultimate postoperative knee joint kinematics, lower extremity strength, dynamic balance, and functional hop testing performance, with little published on the effect of time from surgery. The current study was designed to assess these parameters between the ITB ACLR and contralateral noninjured knees of patients who underwent the procedure at various time points before testing. We hypothesized that little difference would be found between the postsurgical physeal-sparing ITB limb and the contralateral noninjured limb.
Methods
Study Design
The current investigation was conducted at a single pediatric tertiary care center using a cross-sectional design. Institutional review board approval was obtained before commencement of the study.
Patient Selection
Patients who had been previously identified for participation in a separate long-term clinical follow-up study of ITB ACLR, 17 published in 2018, were arranged in a database according to their time of reconstruction. Additional patients who underwent ITB ACLR were identified by querying a departmental database utilizing billing codes for ACLR. A sample of the 125 patients living closest to the study institution was selected and contacted by telephone and email recruitment based on a projected estimate of a 33% success rate with recruitment.
These patients were incorporated into the current study database along with the previous study's patients, for a cumulative cohort of study participants. A medical record and imaging review was performed to confirm appropriate inclusion criteria of all patients, which was skeletal immaturity at the time of a primary ITB ACLR procedure. Exclusion criteria were postoperative follow-up of <1 year, additional surgery of any kind on the ITB ACLR limb, multiligamentous knee reconstruction at the time of ITB ACLR, and any major injury or surgery on the contralateral knee. This component was an essential exclusion criterion, in that use of the limb symmetry index (LSI) was an essential analytical feature for the current study, and contralateral surgery or injury could create a confounder for the normal health and function of a patient's non-ITB ACLR side.
To study the effect of ITB ACLR on knee function over a broad period of time, the study design was developed to include approximately equal patients in each of 4 subcohorts structured according to time from surgery: 1 to <2 years postoperatively, 2 to <5 years postoperatively, 5 to 10 years postoperatively, and >10 years postoperatively. Because recruitment was felt to be optimized through greater geographic proximity, patients were further stratified according to their home address zip code, and recruitment was initiated from the zip codes closest to the study institution, moving outward over time, depending on the number recruited in each of the follow-up time-based cohorts. Research personnel contacted eligible participants by telephone and asked their willingness to participate in this study. As a means of incentivization for patients who had already completed their full course of clinical follow-up visits after their procedure, all potential participants were offered $100 in the form of an Amazon.com gift card, which was provided at the end.
Testing
All data were collected by 1 of 3 different certified athletic trainers with >1 year of experience in the current protocol while working at the injury prevention research and training center affiliated with the host study institution. A handheld dynamometer (Hoggan Scientific) was used to evaluate the isometric strength of each patient's quadriceps, hamstrings, and hip abductors. For quadriceps strength, participants were asked to sit down on the edge of the treatment table with 90° of knee flexion and arms crossed in front of their chest. Then, the dynamometer was applied to the anterior side of the distal tibia above the dome of the talus, and participants were asked to extend their knees with maximum effort. For hamstring strength, participants were asked to lie down on their stomach with 90° of knee flexion. The dynamometer was applied at the posterior side (Achilles tendon side) of the distal tibia, and participants were asked to further flex their knees toward the hip with maximum effort. For hip abductor strength, participants were asked to lie down on their side, and the targeted leg was slightly pulled toward the posterior and downward directions. The dynamometer was applied to the lateral aspect of the leg just above the lateral malleolus, and participants were asked to move their legs to the ceiling with maximum effort (direction of hip abduction). The strength test was performed 2 times per muscle group bilaterally. Intraclass correlation coefficients were obtained to evaluate interrater and intrarater reliability before the study, which indicated the following: interrater reliability of muscle strength (96.6%; 95% CI, 88.6%-99.3%) and intrarater reliabilities of testers A (90.8%; 95% CI, 71.6%-97.0%), B (98.9%; 95% CI, 96.8%-99.7%), and C (99.5%; 95% CI, 98.5%-99.8%).
In the single-leg hop test, participants hopped with a single leg and were instructed to maintain balance on landing for 3 seconds. Consistent with previous studies,31,32,42 a tape measure and stopwatch were used to perform the test. All hop tests were performed twice on each leg, and the mean value was calculated for data analysis. Dynamic balance was quantified using a commercially available Y-balance assessment system (Functional Movement Systems) as previously described.31,32 Participants were instructed to stand at the center of the equipment and push a plastic piece in the anterior, posteromedial, and posterolateral directions. This was performed 3 times in each direction, and based on the measurements of the 3 directions, a composite score was calculated.
Patient-reported outcomes included the Pediatric International Knee Documentation Committee (Pedi-IKDC) form, a region-specific survey of knee function, and the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS), a measure of activity, both of which are validated for children and have been shown to be usable in adult populations as well.10,25 These 2 surveys were provided to the patients and recorded on the same day of testing.
Statistical Analysis
Basic demographic features of the study population were analyzed by descriptive statistics. To evaluate the involved limb's recovery based on the uninvolved limb, LSI scores were used. The LSI score is calculated by dividing the performance of the ACLR limb by the performance of the uninvolved limb and multiplying by 100, with 100% indicating perfect symmetry between the ACLR and uninvolved limbs. 8 This technique has been used frequently when reporting postoperative recovery status using lower extremity functional tests in previous studies with patients who have undergone ACLR.8,13 Deficits were calculated by subtracting 100 from each LSI score. Percentages were used to express both LSI scores and deficits, with negative scores indicating a deficit.
Paired t tests were used to compare the strength, balance, and functional test results in the surgical and nonsurgical limbs, with a P value <.05 considered statistically significant. However, paired t tests that did not detect statistically significant differences (P > .05) were not considered to confirm equivalent function between surgical and nonsurgical limbs. Equivalency analysis was therefore utilized to better assess this statistical concept. Equivalence testing was performed based on the two 1-sided tests of Schuirmann. 27 A margin of equivalence of −8% to 8% was chosen a priori. The overall P value for the equivalence testing was the maximum P value from 2-sided paired t tests. A threshold of .05 was considered as statistically significant; however, unlike typical statistical interpretation, a P value <.05 confirms equivalency between the 2 limbs. Also, instead of typical 95% confidence intervals, 90% confidence intervals were used. The 90% confidence intervals provide more confidence than the traditional 95% confidence intervals in the equivalency analysis, and this cutoff value was used in a previous study with equivalency analysis. 34 Pearson correlation coefficients and linear regression analyses were used to assess for a relationship between the time from surgery to testing and various outcome variables. The threshold for statistical significance for these tests was taken as a P value <.05. All statistical analysis was performed using SAS (SAS Institute).
Results
After the recruitment process, 40 participants were included in the strength, function, and balance analysis (9 in 1 to <2 years, 13 in 2 to <5 years, 10 in 5 to 10 years, and 8 in >10 years after ACLR). Figure 1 depicts the recruitment of participants in a flow diagram including the reasons for exclusion at each stage. Of the 40 included patients, there were 8 females and 32 males with a mean age of 16.8 years (range, 7-15 years) at time of reconstruction and 16.8 years (range, 10-30 years) at the time of testing. Characteristics of the participants, including age, height, weight, and body mass index, are expressed in Table 1. The mean time at which testing was complete was 5.8 years (SD, 4.8 years; range, 1.1-17.2 years) postoperatively. Figure 2 illustrates time between ACLR and time of testing.
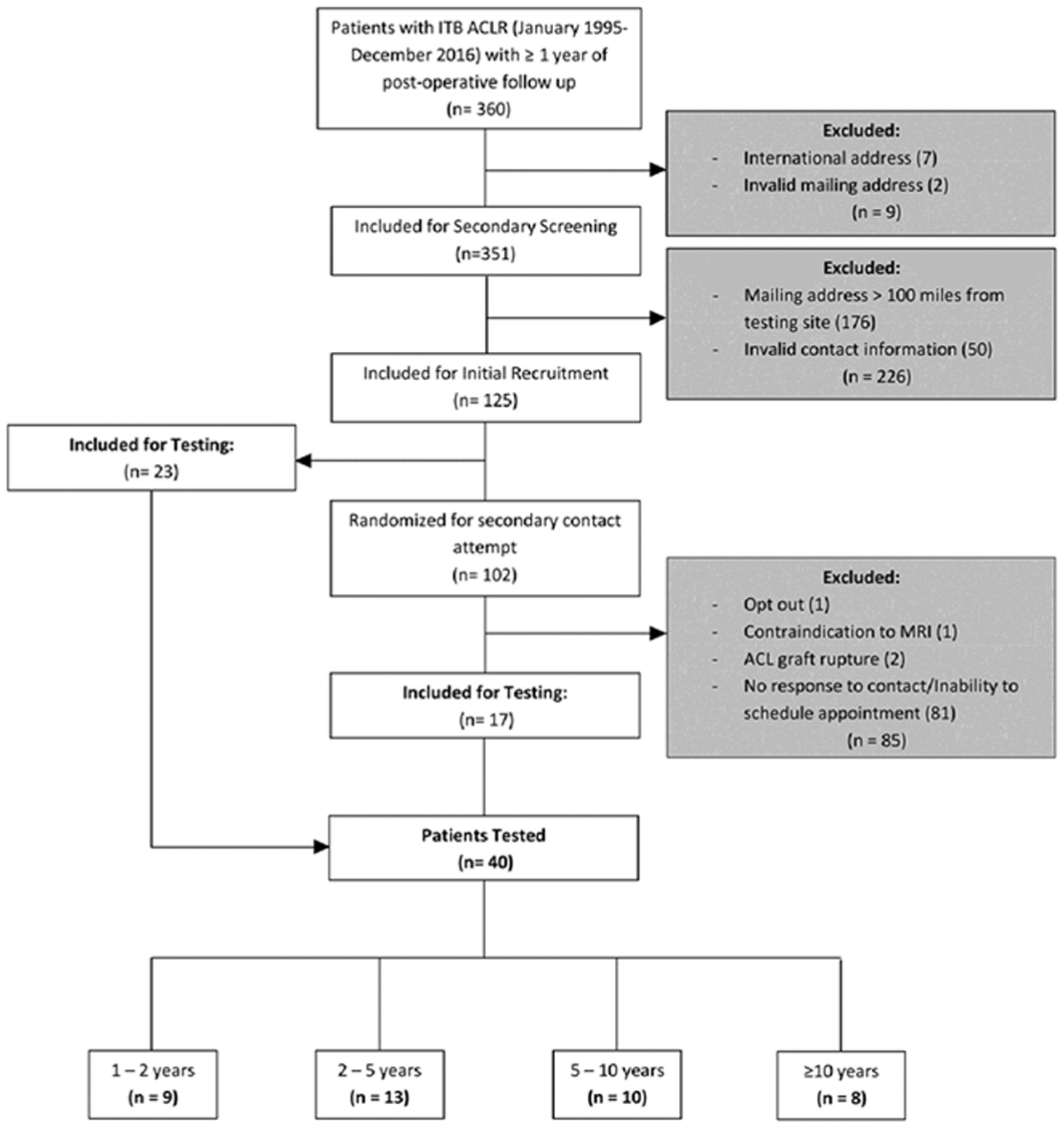
Flow diagram depicting the patients included in the study along with reasons for exclusion at each stage. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; ITB, iliotibial band; MRI, magnetic resonance imaging.
Characteristics of Included Participants a

Data are presented as mean ± SD. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; F, female; M, male.

Distribution of follow-up for patients who underwent primary iliotibial band (ITB) anterior cruciate ligament reconstruction (ACLR) during skeletal immaturity.
When comparing the operative limb to the contralateral side, the mean LSI for the single-leg hop test was 100.8% (SD, 13%) and that for the dynamic Y-balance test was 98.4% (SD, 4.8%). Equivalence analysis confirmed statistical equivalency with a margin of equivalence of −8% to +8% between limbs for the single-leg hop (P = .001) and Y-balance (P < .001) tests. For isometric strength tests, no significant differences between the operative and nonoperative limbs were seen in mean strength testing for the hip abductor (LSI, 97.9%; P = .207), quadriceps (LSI, 97.9%; P = .260), or hamstrings (LSI, 102.6%; P = .264). Equivalence analysis confirmed statistical equivalency with a margin of equivalence of −8% to +8% between limbs for hip abductor strength (P = .01), quadriceps strength (P = .033), and hamstring strength (P = .01). The mean LSI scores along with their associated 90% confidence intervals, in relation to the −8% to +8% margin of error, are depicted in Figure 3.

Mean limb symmetry indices for function, balance, and strength testing, with their associated 90% confidence intervals depicted in the −8% to +8% margin of error. Abd., abduction.
There was no significant correlation between the time from surgery to testing and single-leg hop scores (P = .804), Y-balance scores (P = .33), quadriceps strength (P = .948), or hamstring strength (P = .272). Hip abduction strength was significantly correlated with the time from surgery to testing (regression coefficient = 1.1; P = .027), indicating that, on average, hip abduction strength LSI scores were 1.1% higher for each 1-year increase in time from surgery to testing. At the time of testing, the mean Pedi-IKDC score was 95.9 (SD, 4.9) and the mean HSS Pedi-FABS score was 22.2 (SD, 6.0). There was a significant decline in HSS Pedi-FABS scores (r = −0.37; P = .019) with increasing time from surgery.
Discussion
In the current study, lower extremity functional assessments of strength, balance, and hop testing after ITB ACLR demonstrated equivalence when comparing ACLR and contralateral noninjured ACLR limbs, with differences of <3% between sides. The strength and patient-reported outcome scores were collected at both short- and long-term follow-up. The reported nonanatomic features of the ITB ACLR procedure do not appear to translate into clinically meaningful limitations in performance or function, which were not noted at any time point sampled in this study.
Previous studies have reported promising functional outcomes after ITB ACLR in pediatric patients, in comparison to ACLR with other graft types. Wren et al 41 assessed 145 pediatric patients after ACLR with either ITB (20 patients), hamstring tendon (HT), quadriceps tendon (QT), or bone–patellar tendon–bone (BTP) autografts. Notably, patients who had undergone ITB ACLR were younger (mean age, 11.3 years) than those who had undergone ACLR with other graft types. The authors assessed knee extensor recovery with biomechanical testing of dynamic function during vertical drop jump and side-step cutting tasks within 18 months postsurgery. They found that the deficit in dynamic knee extensor function between the operative and nonoperative limbs was smallest in the ITB ACLR group, and this was significantly smaller than the deficit in the QT ACLR and BTP ACLR groups (maximum moment in drop vertical jump and cutting; ITB: −0.4, QT: −1.8, BTP: −1.2 [N·m/kg as a unit]). 41 Similarly, Sugimoto et al 31 compared functional performance between the operative and nonoperative limbs in 160 male pediatric patients after ACLR with either ITB (33 patients), BTB, or HT at 6 to 9 months postoperatively. The deficits for the ACLR-ITB group, with respect to the functional hop test and balance performance in the operative limb, ranged from 0% to 17.9%, which was comparable, or more favorable, to the deficits identified in the BTB ACLR (1%-34%) and HT ACLR (0%-29.5%) groups. 31 In another study, Sugimoto et al 33 assessed 164 adolescent males after ACLR for strength deficits at 6 to 9 months postoperatively. Patients in the ITB ACLR group showed a significantly smaller mean quadriceps deficit (1.2%) than patients in the BTB ACLR group (12.2%) (P = .002), and demonstrated significantly smaller mean hamstring deficits (7.7%) than patients in the HT ACLR group (31.7%) (P = .001). 33 In the present study, patients who underwent ITB ACLR had no significant deficit in single-leg hop test performance and a mean Y-balance deficit of only 1.6% at follow-up testing ranging from 1 to 17 years. Furthermore, strength testing revealed no significant deficits in hamstring (higher in the operative leg, 2.6% surplus), quadriceps (2.1% deficit), and hip abductor (2.1% deficit) strength. To provide a quantitative perspective for these small differences, equivalency testing was performed and confirmed statistical equivalence between the operative and nonoperative limbs for each of these functional, balance, and strength testing parameters.
The substantially lower extremity strength, functional, and balance test performance outcomes recorded in this study cohort are remarkable because <10% of deficits in the ITB ACLR limb relative to the contralateral noninjured limb are often reported in the prepubescent group. Greenberg et al 13 assessed strength and functional performance in 16 patients who had undergone ACLR with an all-epiphyseal approach. At a mean of 15.4 months postoperatively, 75% of patients had not yet reached the commonly used threshold of 10% deficits across all strength and functional test parameters. 13 In a study of adolescent patients who had been cleared to return to sport post-ACLR with a mean age of 17.1 years, 21.7% to 56.5% of participants did not meet the individual strength and functional hop test threshold of 10% deficits, while 87.1% of participants did not meet the 10% threshold across all strength and functional assessments. 35 The poor performance with strength and functional assessments in skeletally immature patients postoperatively may have been related to a different and possibly slower recovery in this prepubertal population. 43 In adults, the initial gain in strength after ACLR is thought to be caused by less muscular inhibition and better motor unit functioning, while subsequent strength gains are caused by actual muscle hypertrophy. 1 However, in skeletally immature patients who lack androgens, muscle hypertrophy does not occur to the same extent, and most of the strength recovery occurs with improvements in motor unit coordination and activation.5,26 Because of this, rehabilitation for skeletally immature patients must be modified to focus on dynamic, multijoint neuromuscular control. 3 Furthermore, psychological factors may play a larger role in the delayed recovery in younger children, including anxiety relating to extensive or painful rehabilitation, as well as fear of reinjury.3,4 Generating or maintaining focus and motivation during home exercise programs may also be more difficult in prepubescent patients, and unsupervised exercises are often not performed correctly. 19 Given these rehabilitation challenges in youth athletes, ITB ACLR, which does not involve the harvesting of, and subsequent weakness of, the hamstring or quadriceps tendon, may provide these patients with strength and functional advantages during the rehabilitation phase. Thus, ITB ACLR appears to have a very different profile of functional donor site morbidity than ACLR involving hamstring or quadriceps autograft.
At times, ITB ACLR has been cited as nonanatomic, given the configuration of the technique. However, several biomechanical studies have shown equivalent or superior biomechanical or kinematic characteristics of the post-ITB ACLR knee, when compared to other ACLR techniques. For example, in one cadaveric study, Kennedy et al 15 found that ITB ACLR better restored anteroposterior stability and rotational control compared to all-epiphyseal or transtibial over-the-top physeal-sparing ACLR. Similarly, Trentacosta et al, 36 in another cadaveric study, found that ITB ACLR better restored anteroposterior translation in ACL-deficient knees compared to ACLR with all-epiphyseal techniques. Furthermore, the authors found that when both the ACL and ALL were deficient, ITB ACLR best restored rotational stability to the level of the intact state, while ACLR combined with ALL reconstruction using all-epiphyseal techniques resulted in residual rotational instability at 60° and 90°, despite the attempted extra-articular stabilization component. 36 Some have argued, based on findings in cadaveric studies, that the superior constraint provided with ITB ACLR may also result in rotational overconstraint at some flexion angles, which may further lead to adverse long-term joint health and potentially degenerative joint disease in the lateral weightbearing compartment of the knee.15,28 A recent study on the same cohort of patients who underwent ITB ACLR as in the present study was designed to assess the kinematic parameters of the knee after ITB ACLR using 3-dimensional motion analysis. 34 The study found equivalency between the operative and nonoperative knees, with respect to mean peak normalized knee moments, as well as ground-reaction forces. 34 The restoration of normal symmetric physiological kinetic and kinematic function, coupled with the findings in the present study of restoration of normal strength, function, and balance test performance, demonstrates that if there is any component of increased rotational constraint provided by ITB ACLR, it does not appear to translate into deleterious kinematic function or performance at short- or long-term follow-up.
Limitations
Limitations of the current study include the wide range of follow-up times, from 1 to 17 years postoperatively. Also, the number of male patients was significantly greater than that of female patients, which may not make the findings completely generalizable to female patients. The contralateral limb was used for comparison to determine the strength deficits of the operative limb. Because patients can experience de-training of the uninvolved limb after ACLR, these LSI values could overestimate the strength and function of the operative limb compared to the true preinjury capacity level. 39 However, because the patients’ follow-up time points ranged from a minimum of 1 year postoperatively to >15 years postoperatively, the design of the study likely eliminated a significant influence of de-training on the nonoperative side. The current strength, balance, and hop test assessments after ACLR have been established for use in the general population and have not yet been validated or standardized for the pediatric population. Further research is needed to assess whether standardized, pediatrics-specific testing procedures with further verbal and visual demonstrations are needed to ensure the accuracy of these results. 19 Moreover, there are a number of other important factors that play a role in the recovery post-ACLR, rather than simple performance levels, such as a patient's psychological readiness. 37 Therefore, the results of this study should be taken in context of the larger rehabilitation considerations that include an athlete's mental and physical readiness as well as the level and type of physical activity.
Conclusion
Lower extremity strength and functional testing after ITB ACLR demonstrated equivalence or minimal (<3%) variation, when comparing ACLR and contralateral noninjured ACLR limbs, with patient-reported functional outcome scores in both short- and long-term follow-up. The reported nonanatomic features of the ITB ACLR procedure do not appear to translate into clinically meaningful limitations in performance or function, which had resolved at 1 to 17 years postoperatively.
Footnotes
Final revision submitted January 21, 2026; accepted January 31, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Boston Children's Hospital (IRB-P00022690).