
Abstract
Background:
Ramp lesions, tears at the posteromedial meniscocapsular junction, often accompany anterior cruciate ligament injuries and compromise stability. The all-inside repair is gaining popularity for its minimally invasive approach, though comparative data with suture hook (SH) repair remain limited.
Purpose:
To compare clinical outcomes of all-inside suture implant (SI) versus SH repair technique for ramp lesions.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
A PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses)-guided search of PubMed, EMBASE, Cochrane Library, and Google Scholar identified studies comparing all-inside SI versus SH repair for ramp lesions. Two reviewers independently screened, extracted data, and assessed quality with the Risk Of Bias in Non-Randomized Studies–of Interventions. Pooled mean differences and odds ratios (ORs) were calculated, with heterogeneity evaluated by Q-test and I2, applying random-effects models when appropriate.
Results:
Five studies (2 case-control and 3 cohorts) with 901 patients were included; 388 underwent all-inside SI repair. The mean age was 28.71 years, with follow-up ranging from 12 to 24 months. There was a significant difference in overall repair failure between groups, with 99 failures out of 388 cases (25.5%) in the all-inside SI group compared with 55 failures out of 513 cases (10.7%) in the SH group (OR, 2.36; P < .01). Specifically, all-inside SI repair demonstrated a greater likelihood of secondary meniscectomy (OR, 2.40). Postoperative International Knee Documentation Committee, Tegner, Lysholm, and return-to-sport rates showed no significant differences. Preoperative laxity >7 mm and age ≤20 years did not significantly affect failure risk.
Conclusion:
SI repair for ramp lesions shows higher failure and secondary meniscectomy rates than SH repair. Functional outcomes appear largely comparable between the 2 repair techniques. Results should be interpreted cautiously, as outcomes depend on surgical technique, visualization, suture configuration, and rehabilitation. More high-quality studies are needed to define the optimal repair method.
Keywords
Meniscal ramp lesions commonly occur in conjunction with anterior cruciate ligament (ACL) ruptures. Initially described by Strobel 16 in 1988, these lesions involve the disruption of the posterior horn of the medial meniscus and its peripheral attachments with the capsule at the meniscotibial junction. This is thought to occur as a result of increased anterior translation of the tibia in the setting of ACL rupture, which leads to increased laxity and secondary forces on the posterior horn of the medial meniscus. Historically, this intra-articular pathology has been underdiagnosed because of its location within the blind spot of the posteromedial knee when viewing through the standard anterolateral and anteromedial viewing portals of arthroscopy.3,7
In recent years, it has become increasingly recognized when considering surgical intervention for ACL ruptures. Multiple studies have reported a prevalence rate of 16% to 40% when identifying ramp lesions concomitant with ACL rupture.9,14 These ramp lesions have been shown to significantly affect knee stability, with a biomechanical study by DePhillipo et al 6 showing that ramp lesions involving the posterior horn of the medial meniscus at the meniscocapsular and meniscotibial attachments resulted in significant anterior tibial translation, rotational instability, and the pivot-shift phenomenon. As a result, it has become standard practice to accurately diagnose these lesions when treating ACL ruptures and address appropriately with repair to ensure better postoperative outcomes.2,6,11
Treatment options include observation, primary repair with local abrasion or trephination to stimulate a vascular healing response at the meniscal periphery, and suture repair. When it comes to primary suture repair, multiple surgical techniques have been described. Recently, an all-inside approach has gained popularity as the go-to option for repair, as it offers several advantages over a traditional inside-out approach, including a lower level of technical difficulty compared with other techniques and a minimally invasive approach because of the avoidance or requirement of a posteromedial portal.1,5,19 The all-inside repair can be accomplished by the use of a posteromedial working portal and curved SH or with an anteromedial approach using an all-inside meniscal repair system.10,15
Despite its growing popularity, the current literature is limited when comparing the effectiveness of the all-inside technique versus other traditional repair techniques. The lack of comparative studies may be due to multiple factors, including variability in the degree of instability, lesion size, and the presence of concomitant pathology that may influence the choice of surgical approach. 1 The primary goal of this systematic review and meta-analysis was to compare the overall failure rates of the all-inside SI technique versus all-inside SH repair technique used to address meniscal ramp lesions. Secondary objectives include comparison of patient-reported outcome measures and assessment of factors related to failure. We hypothesize that the all-inside SI repair technique has a failure rate comparable with that of the all-inside SH repair technique, with patient-reported outcomes largely similar between the 2 groups.
Methods
Search
This meta-analysis was conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A comprehensive multidatabase search was performed using PubMed, EMBASE, the Cochrane Library, and Google Scholar (pp 1-20), covering the period from database inception to February 3, 2025. The Medical Subject Headings and Boolean operators used in the search were (Ramp Lesion OR Ramp lesions OR Ramp meniscus tear OR posteromedial meniscus tear) AND (all-inside OR all inside OR Fast Fix). Articles identified through this search, along with their references, were reviewed for inclusion based on specific eligibility criteria.
Studies were included if they reported on patients with ramp lesions who underwent surgical repair and directly compared the clinical outcomes and complication rates of the all-inside SI repair technique with all-inside SH repair method. Studies were excluded if they were not peer reviewed, focused on other types of meniscal tears, did not make a direct comparison between all-inside repair and another technique, or compared the all-inside technique with nonoperative treatment. Studies solely describing the all-inside technique without comparison were also excluded. All studies using the all-inside SI technique had utilized the Fast-Fix (Smith & Nephew) meniscal repair device, which has polyetheretherketone anchors and a nonabsorbable 2-0 ultra–high molecular weight polyethylene suture. Two independent reviewers (B.K., K.C.V.) screened all records retrieved from the initial search and assessed them for eligibility. Discrepancies between reviewers were resolved through discussion and consensus with the senior author (Y.R.).
Data Extraction
Data extraction was independently performed by 2 reviewers (M.M., B.K.) and included details on study design, publication year, study period, patient demographics, sample sizes, functional outcomes, and complications. Functional outcomes assessed included the International Knee Documentation Committee (IKDC) score, Tegner activity scale, Lysholm score, return-to-sport rates, and failure of repair as defined in each individual study.
Quality Assessment
The quality of the included studies was evaluated by 2 independent reviewers (M.M., B.K.) using the Risk Of Bias in Non-Randomized Studies–of Interventions (ROBINS-I) Version 2 tool. 12 Seven domains were assessed for each study to determine the overall risk of bias and study quality.
Statistical Analysis
Statistical analyses were conducted using SPSS Version 29.02 (IBM Corp). For continuous variables, mean differences with 95% CIs were calculated. For dichotomous variables, odds ratios (ORs) were used. Heterogeneity was assessed using the Q test and I2 statistic. When substantial heterogeneity was detected (P≤ .05 or I2 > 50%), a random-effects model was applied; otherwise, a fixed-effect model was used. A P value ≤ .05 was considered statistically significant.
Results
Figure 1 illustrates the PRISMA flowchart outline of the study selection process. The initial search yielded 511 studies, of which 114 were excluded due to duplication. The remaining 397 studies underwent title and abstract screening, resulting in the exclusion of 299 studies based on predefined inclusion and exclusion criteria. Full-text screening was conducted for 98 studies, and ultimately, 5 studies were included in the final analysis.4,8,13,18,20 Reasons for exclusion of the remaining 93 studies are detailed in Figure 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram illustrating the selection and designation of study cohorts.
Risk of bias was assessed using the ROBINS-I tool. Of the 5 studies, 4 were rated as low risk, while 1 study (Cheng et al 4 ) was rated as having moderate risk (Figure 2).

Risk-of-bias assessment across all domains for each included study.
This meta-analysis included 901 patients with ramp lesions and concomitant ACL deficiency, of whom 388 underwent SI repair and 513 underwent SH repair. The mean age of participants was 28.71 years (Table 1). Mean follow-up duration ranged from 14.9 months (Cheng et al 4 ) to 108.3 months (Gousopoulos et al 8 ), while the minimum follow-up ranged from 12 to 18 months (Cheng et al) to 24 months across all other included studies. Further details are provided in Table 1.
Characteristics of Included Studies a

Data are presented as mean, mean ± SD, or n. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; NA, not available; PDS, polydioxanone; SH, suture hook; SI, suture implant.
A range of clinical outcomes was assessed. The primary outcome was repair failure, as defined by each individual study; detailed definitions are provided in Table 2. Only 3 studies reported Kaplan-Meier survival analysis with a minimum follow-up of 4 years. The mean survival rate for the all-inside SI repair group was 0.74, compared with 0.86 for SH repair technique.
Outcomes of Interest Reported in Included Studies a

Data are presented as n. MRI, magnetic resonance imaging; NA, not available.
There was a significant difference in overall repair failure between groups, with 99 failures out of 388 cases (25.5%) in the all-inside SI group compared with 55 failures out of 513 cases (10.7%) in the SH group (OR, 2.36; P < .01) (Figure 3A). Figure 3B demonstrates that SI repair was associated with a statistically significant 2.40-fold increase in the odds of requiring a secondary meniscectomy compared with SH repair technique. However, there was no significant difference in the odds of failure to heal between all-inside SI and SH techniques.
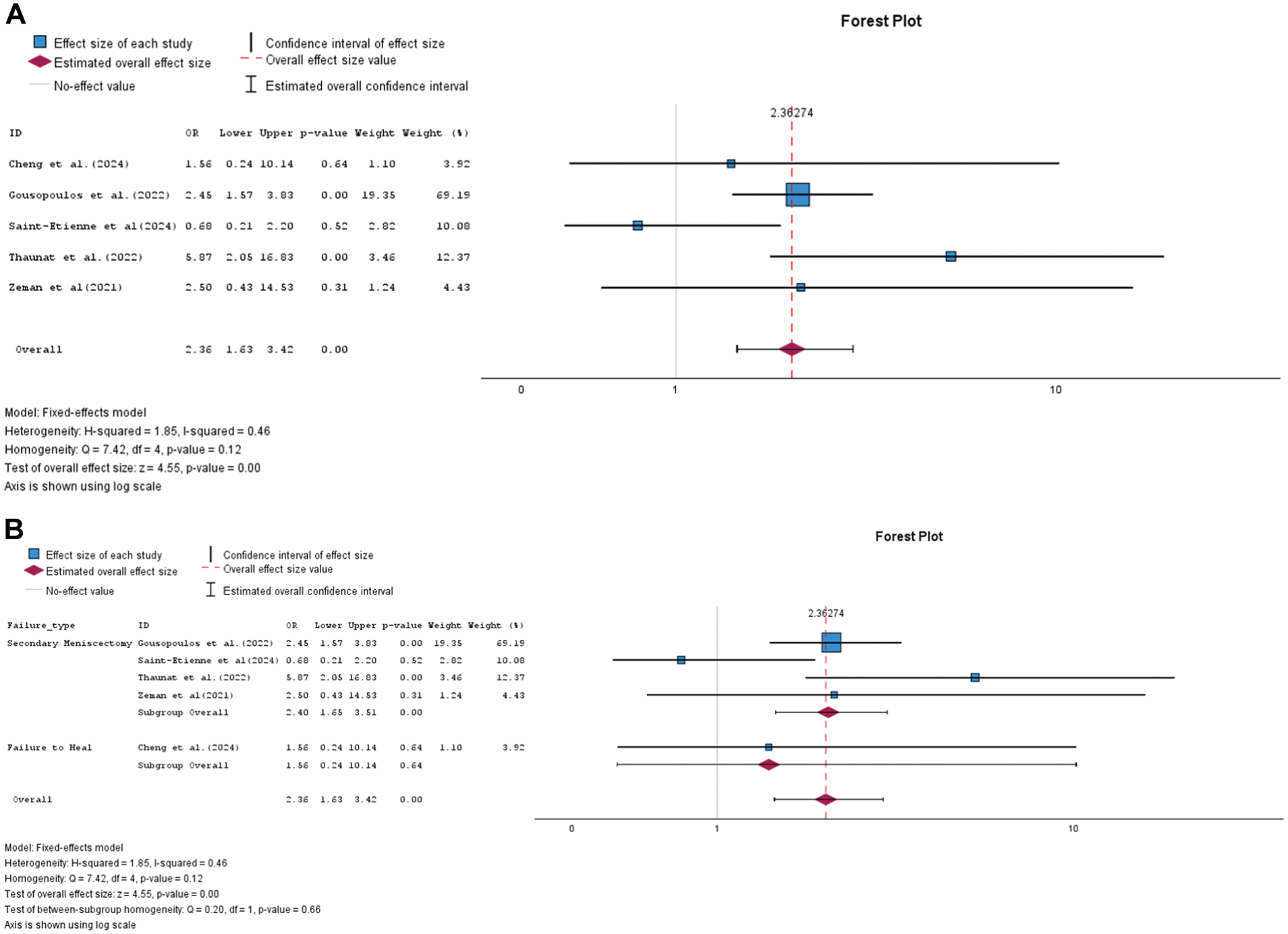
Forest plot. (A) Comparison of odds of failure between all-inside repair and other repairs combined. (B) Subgroup analysis comparing odds of failure between all-inside suture implant and suture hook based on the failure type. OR, odds ratio.
SI repair did not show any significant difference in terms of IKDC score, with a mean difference of −3.22 compared with the SH techniques. Additionally, no significant differences were observed between all-inside SI repair and SH repair methods in terms of postoperative Tegner (5.06 ± 1.96 vs 5.33 ± 2.02; P = .48) and Lysholm scores (88.27 ± 13.19 vs 89.22 vs 11.31; P = .97), or in the odds of returning to sports (65/85 (76.5%) vs 81/97 (83.5%); P = .22) (Figure 4).
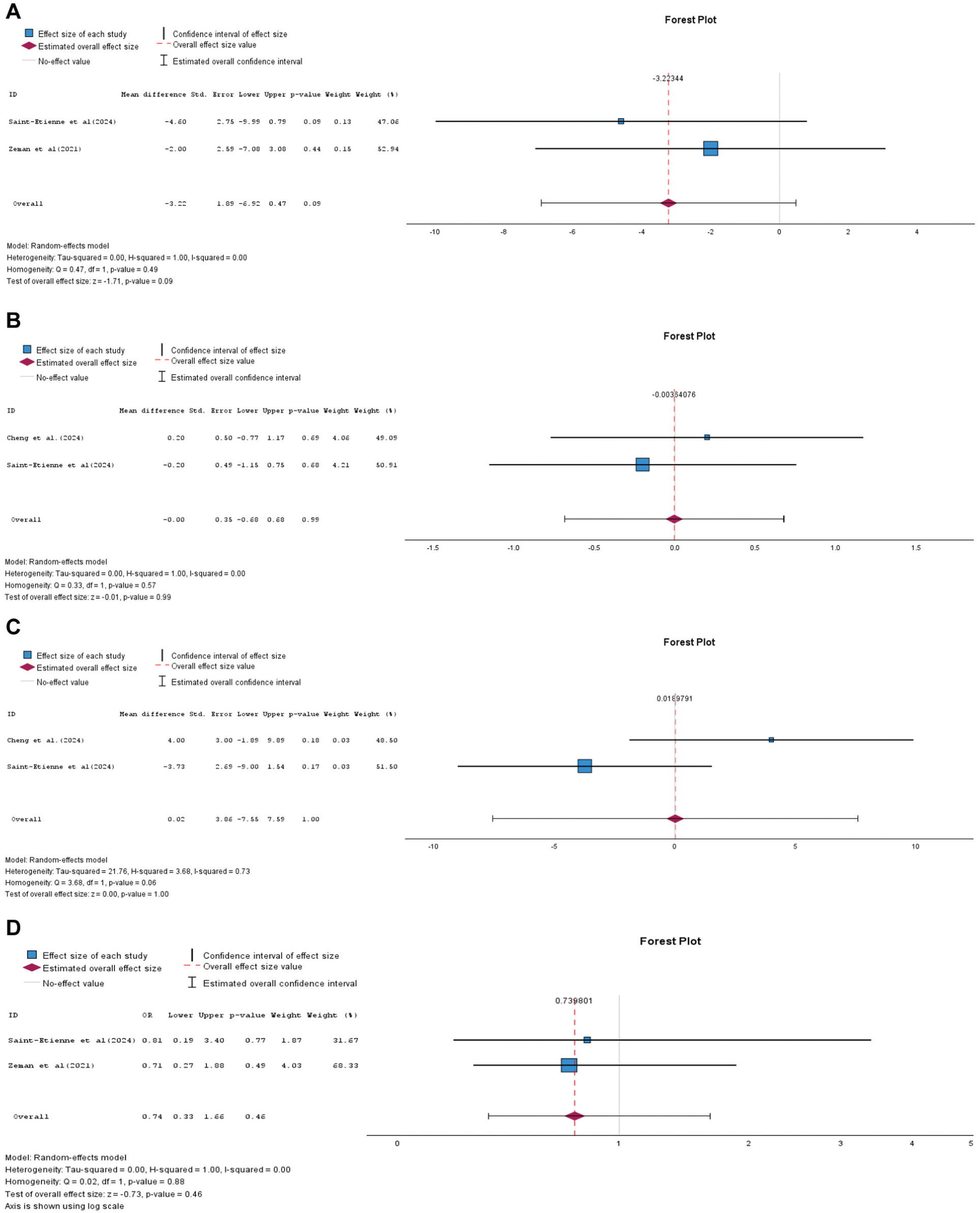
Forest plot illustrating outcomes of interest comparing all-inside suture implant repair to suture hook repairs. (A) Mean difference in International Knee Documentation Committee score. (B) Tegner activity score (C) Lysholm score. (D) Odds of return to sports. OR, odds ratio.
Figure 5 shows that preoperative side-to-side laxity >7 mm and patient age ≤20 years do not significantly increase the odds of failure following ramp lesion repair.

Forest plot illustrating the effect of preoperative factors on odds of failure following ramp lesion repair. Top panel: side-to-side laxity >7 mm vs ≤7 mm. Bottom panel: age ≤20 vs >20 years. OR, odds ratio.
Discussion
The importance of diagnosing meniscal ramp lesions and the effect these injuries have on knee stability has been demonstrated in recent literature. 6 This study evaluated a newer technique, the all-inside SI approach, and compared outcomes with SH technique. In this meta-analysis, 41.5% of patients (388/934) treated across all studies underwent repair of meniscal ramp lesions with the all-inside SI repair technique.
All-inside SI repair has demonstrated a significantly higher failure rate as compared to the All-inside SH repair. The SI repair group was associated with higher odds of failure and secondary meniscectomy compared to SH repair. Failure was defined as either need for secondary meniscectomy8,13,18,20 or failure to heal. 4 However, when this was further stratified by failure type, it was found that there was a significantly higher odds that the all-inside SI technique would require secondary meniscectomy as compared to the SH repair techniques (Figure 3B). Postoperative IKDC, Tegner, Lysholm scores, and return-to-sport rates showed no significant differences between the groups.
There are several explanations to consider as to why our analysis reported a higher failure rate when comparing all-inside to the SH technique. The SH technique utilizes a posteromedial working portal and a transnotch viewing portal that can enhance the field of view for these lesions when facilitating repair. Modern all-inside SI techniques should also demand comparable visualization to achieve optimal results; however, it is unclear if this was achieved with earlier all-inside SI techniques.4,8 In addition, all-inside SI technique requires a more robust stitch pattern that provides circumferential compression both above and below the meniscus, similar to SH constructs. It is also important to note that many of the included studies likely evaluated earlier-generation plastic-based all-inside implants rather than contemporary all-SIs.
It is also important to consider anatomic factors associated with ramp lesions including the meniscotibial ligament, a critical structure in anchoring the posterior meniscus to the tibial plateau. The SH technique with its posteromedial portal may allow for direct access of the entirety of the lesion, which may allow for better preparation of the tear surfaces and the perimeniscal synovium, when, in comparison, an all-inside SI technique from a transnotch view may be more limited. 8 As a result, the SH technique can facilitate more accurate assessment and suture passage, leading to an anatomic reduction. Additionally, it can allow for placement of sutures that are oriented perpendicular to the longitudinal fibers of the meniscus, leading to greater fixation. 18 This is critical when considering the hidden nature of these lesions. The study by Saint-Etienne et al 13 highlights this, as its cohort consisted of type 3 meniscal ramp lesions.
A classification system for meniscal ramp lesions previously proposed by Thaunat et al 17 attempts to separate these lesions into 5 categories based on location and stability. Type 3 lesions are defined as partial inferior tears that involve the interior portion of the meniscocapsular junction. As a result, they are not readily identifiable from standard arthroscopic anterior or posteromedial viewing portals; thus, careful probing is crucial in finding these lesions. Although the study by Saint-Etienne et al did not demonstrate a significant difference in failure rates between all-inside and SH techniques for type 3 lesions, it does bring to question what factors should ultimately be considered when deciding an appropriate technique to address meniscal ramp lesions. Stability may be one of these factors. Type 1 and type 2 ramp lesions, defined as peripheral meniscocapsular separations located within the synovial sheath and partial superior lesions, respectively, are generally considered stable. Because of their stable nature, they may not require the use of an SH technique for accurate suture placement or anatomic repair. In contrast, type 3 through type 5 lesions are typically unstable. Type 3 lesions involve a partial inferior tear; type 4 lesions represent a complete tear within the red-red zone; and type 5 lesions are characterized by a double tear affecting both the meniscocapsular junction and the meniscotibial ligament, resulting in 2 distinct disruptions in the posterior horn of the medial meniscus. These unstable lesion types may benefit from an SH technique over all-inside or other repair methods to ensure optimal anatomic restoration. 20
Saint-Etienne et al 13 and Thaunat et al 18 also refer to the Tachibana effect when considering a higher risk of failure seen with the all-inside SI technique compared with SH. The Tachibana effect refers to iatrogenic tears that develop as a result of needle and suture passage when performing a repair. More precise placement with the SH technique may minimize this effect and could potentially explain the difference in failure between the 2 techniques.
The Tachibana effect may also explain increased rate of secondary meniscectomy in all-inside meniscal repair device technique. Multiple passes of suture may lead to further degradation of already damaged tissue at which point a secondary repair may not be a feasible option. Additionally, because of the advantages of the SH repair, reinjury may result in a tear that is usually more anterior to the prior site of ramp lesions, necessitating a smaller meniscectomy. All-inside techniques with the standard anterior approach may have a tendency to fail posteriorly, which would require a larger area of meniscectomy subsequently. 8
Although the SH technique offers several advantages, it also has drawbacks, including greater technical demands, a steep learning curve, longer operative times, the need for skilled assistance, and arthroscopic suture tying. It also carries a small risk of damage to surrounding structures such as the saphenous nerve and vein. 18
All-inside SI repair has gained popularity in part due to its minimally invasive nature, with proponents hypothesizing that this technique would result in increased functional outcomes as compared with older techniques such as inside-out repair. This study also reported on differences in patient-reported outcome measures (PROMs). PROMs standardize subjective responses into objective data that can enable hypothesis-driven comparison. All-inside SI repair was shown to have a significantly lower IKDC score, whereas other PROMs such as Tegner, Lysholm, and return to play did not demonstrate any difference. Although there is some overlap in areas that each PROM survey assesses, these mixed results demonstrate that overall patient satisfaction can be open to different methods of data collection and interpretation. Nonetheless, it is important to consider when attempting to identify a surgical technique that could offer significantly improved functional outcomes. Overall, our analysis did show relatively similar functional outcomes between all-inside repair and other repair techniques.
This study showed that patient age (<20 years of age) and preoperative laxity as defined as >7 mm when compared with the contralateral side showed no significant difference in failure rates (Figure 5). This is important to consider especially in a pediatric population with higher Beighton score, as it could further elucidate different treatment guidelines for this particular cohort. Preoperative laxity seen in younger patients could confer higher risk of failure.
Limitations
To our knowledge, this is one of the first studies to compare the all-inside meniscal repair device technique to other traditional techniques for meniscal ramp lesions. However, there are several limitations. First, only 5 studies met our inclusion criteria, none of which was a randomized controlled trial, and several had small sample sizes (3 with <100 patients). All included studies were conducted outside the United States, limiting generalizability. There were also inconsistencies among studies, such as varying definitions of failure and lack of information on lesion stability or pattern, which may affect technique choice and outcomes. Additionally, injuries were not standardized for such factors as chronicity, concomitant knee pathology, graft choice, postoperative protocols, or sex, all of which could influence failure rates.
Furthermore, based on currently available data as of 2025, anchor-based repairs have been associated with a higher failure rate, though the technique is still early in its learning curve, particularly for ramp tears, which have only relatively recently become the focus of these treatments. The studies included in this review are all from 2021 or later, reflecting this early experience. It is possible that with improved techniques, instrumentation, and visualization, the all-inside SI technique may achieve better efficacy and outcomes in the future.
A key limitation of this study is the variability in surgical techniques and implant types included across studies. Many of the all-inside SI repairs analyzed likely involved earlier-generation plastic-based implants rather than modern all-suture devices, which may not reflect current practice. Furthermore, the quality of repair in the included studies may have been influenced by factors such as adequacy of visualization, suture configuration, and use of circumferential compression stitches above and below the meniscus, techniques that are now considered critical but may not have been consistently employed. Additionally, the included studies were performed by high-volume, experienced surgeons, and the reported outcomes in the SH cohort may not be generalizable in other settings.
Last, the included studies by Thaunat et al 18 and Saint-Etienne et al 13 originated from the same institution, raising the theoretical possibility of partial patient overlap, which could introduce bias and disproportionately influence the pooled results. However, the likelihood of meaningful overlap appears limited, as the studies differed in their enrollment periods and inclusion criteria. Specifically, Saint-Etienne et al focused exclusively on type 3 ramp lesions, whereas Thaunat et al 18 included all ramp lesion subtypes. Nonetheless, the potential for residual overlap cannot be entirely excluded and should be considered when interpreting the findings.
Future research should include prospective randomized trials with standardized definitions, matched cohorts, and uniform postoperative protocols to address these limitations.
Conclusion
All-inside SI repair for ramp lesions has been associated with higher reported failure rates and a higher incidence of secondary meniscectomy compared with SH repair. Functional outcomes appear largely comparable between the 2 repair techniques. These findings should be interpreted with caution, as outcomes are likely influenced by surgical technique, visualization, suture configuration, and rehabilitation protocols. Further high-quality studies are needed to better define the optimal repair strategy.
Footnotes
Final revision submitted January 15, 2026; accepted January 22, 2026.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.