
Abstract
Background:
The national opioid epidemic has highlighted the critical importance of opioid stewardship within orthopaedic surgery. Previous research has identified a diagnosis of anxiety disorder as significantly associated with postoperative opioid consumption following upper extremity procedures.
Purpose/Hypothesis:
This study aimed to broaden this understanding by investigating whether measured levels of preoperative anxiety, rather than a broad diagnosis, in patients undergoing arthroscopic rotator cuff repair (ARCR) affected postoperative opioid utilization. It was hypothesized that, in opioid-naive patients, a higher preoperative anxiety score would be associated with increased postoperative opioid consumption.
Study Design:
Cohort study, Level of evidence, 2.
Methods:
Opioid-naive patients undergoing primary ARCR between March 2024 and February 2025 were prospectively enrolled at a multicenter institution. Preoperative patient-reported outcome measures were collected using the American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, Single Assessment Numeric Evaluation, and Patient-Reported Outcomes Measurement Information System Short Form (PROMIS SF) Anxiety 8a. Postoperative opioid use was recorded via a patient-completed pain journal and converted into morphine milligram equivalents (MMEs). General linear models (GLMs) were developed to evaluate the relationship between preoperative anxiety and total MMEs, days of opioid use, and MMEs per day, while controlling for age, sex, and California Area Deprivation Index (ADI). Statistical significance was set at P < .05.
Results:
A total of 64 patients were included with a mean age 63.5 ± 12.2 years (male, n = 32; mean body mass index, 27.1 ± 4.7 kg/m2). The mean total postoperative opioid usage was 119.5 ± 118.7 MMEs over 5.8 ± 4.7 days, with a mean MME per day of 19.0 ± 11.6. Three GLMs showed no significant association between preoperative PROMIS Anxiety T-scores and total MMEs (P = .15), days opioids were taken (P = .13), or MME per day (P = .58). Covariates including age, sex, and ADI were not significant in any model.
Conclusion:
Levels of preoperative anxiety in opioid-naive patients undergoing primary ARCR had no significant effect on total postoperative opioid usage, the number of days opioid medication was taken, or the adjusted daily opioid usage.
Keywords
Rotator cuff tears remain a prevalent shoulder pathology and account for 70% of all shoulder related physician visits, affecting approximately 30% of individuals >60 years and 62% of those >80 years.22,38 Rotator cuff tears can place significant limitations on daily activities due to pain, loss of strength, and functional disability.18,40 Once conservative treatment options fail, ARCR can be an optimal treatment modality with recent advancements providing less postoperative pain and the ability to address complex injuries.8,9,31
As a result of the national opioid epidemic, it is imperative to recognize and minimize opioid misuse within medicine. 25 Many instances of opioid abuse first begin through prescription medications and the opioid-naive have been found to be at an increased risk of long-term misuse.35,37 Despite the decline in overall opioid prescription as a result of local and regional anesthetics and multimodal pain management strategies, prior research indicates that orthopaedic procedures remain the initial event in 8.8% of persistent use cases.11,16,33 Anxiety within the orthopaedic surgical setting is well-documented, with literature suggesting that a preoperative diagnosis of anxiety disorder worsened postoperative mental health outcomes, 2 was a strong predictor of worse functional outcome within ARCR,3,20,24 and caused a significantly higher likelihood of prolonged opioid use.7,15,27 Few studies investigate measured levels of preoperative anxiety, and only recently, MacFarlane et al 26 investigated the presence of preoperative anxiety and postoperative opioid use in the setting of total shoulder arthroplasty.
While existing literature has examined factors affecting postoperative opioid use following ARCR, 29 the extent to which the presence of preoperative anxiety serves as a risk factor for increased opioid use remains unclear. To the authors' knowledge, no prior investigation has specifically explored the interaction between preoperative anxiety levels and postoperative opioid utilization within the ARCR population. Therefore, this study aims to investigate this relationship. It was hypothesized that, in opioid-naive patients, a higher preoperative anxiety score would be associated with increased postoperative opioid consumption.
Methods
Patient Selection
After obtaining institutional review board approval, we conducted a prospective enrollment of patients scheduled to undergo primary ARCR in a multicenter institution between March 2024 and February 2025. Study eligibility was defined as opioid-naive patients undergoing ARCR with an interscalene brachial plexus block using ropivacaine. Opioid-naive patients were defined as those not taking any form of opioid medication prior to their surgery. All eligible patients were approached at their final preoperative visits for study participation. Those who were interested provided informed consent and enrolled in the study. Patients were excluded from this study if they were unwilling or unable to participate, taking any form of opioid medication prior to surgery, underwent a surgical complication postoperatively that significantly altered their opioid usage, did not take any postoperative opioid medication, or received a perioperative nerve block other than interscalene ropivacaine. Patients with a preoperative diagnosis of generalized anxiety disorder (GAD), bipolar disorder, or depression not managed with medication were excluded to mitigate confounding effects from anxiety score increases unrelated to the ARCR procedure.
Procedure Details
All patients underwent ARCR using an interscalene brachial plexus block and general anesthesia. The interscalene brachial plexus block was performed using 20 mL of ropivacaine at 0.5% (5 mg/mL), with the exception of a single patient for whom the ropivacaine injection was diluted to 0.4% (4 mg/mL), to standardize block usage and reduce confounding effects on opioid use. 36 All procedures were performed with standard ARCR techniques using beach-chair positioning with suture anchor fixation determined by intraoperative findings. Additional procedures were performed based on intraoperative findings at the operating surgeon's discretion. Tendon involvement, concurrent pathology, and concomitant procedures are summarized in Table 1. No patient had a rupture involving the teres minor. Evidence of osteoarthritis was determined from preoperative radiographs according to the Kellgren and Lawrence classification system. 21 All patients underwent ARCR procedures at outpatient surgery centers.
Surgical and Pathological Findings (N = 64) a

AC, acromioclavicular; SLAP, superior labrum anterior to posterior.
Data Collection
Patients who consented to participate were asked to complete 3 validated preoperative surveys as standard of care. The American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form survey is a patient-reported outcome measure (PROM) of functional limitations of the shoulder. 28 The Single Assessment Numeric Evaluation asked patients to rate their current shoulder function as a percentage of the preinjury level. 30 The presence and level of preoperative anxiety was collected through the Patient-Reported Outcomes Measurement Information System (PROMIS) Short Form (SF) Adult Anxiety 8a. 34 This consisted of 8 anxiety questions with response options of never, rarely, sometimes, often, and always (Figure 1).4,6 All patients were instructed to complete the survey questions in reference to their feelings toward the procedure. A paper journal was given to patients preoperatively to document their postoperative opioid medication use and dosage. Following a patient's completion of the opioid medication, no further data were recorded, and the pain journals were collected. To account for variance in the prescribed opioid medication, all opioid usage was converted into morphine milligram equivalents (MMEs) according to Centers for Disease Control and Prevention guidelines. 12 Prior to data analysis, PROMIS SF Anxiety 8a scores were converted into T-scores per score analysis guidance from PROMIS. 19

Patient-Reported Outcomes Measurement Information System Adult Short Form Anxiety 8a.
The following patient data were collected and stored in a secure online data sheet: patient name, date of birth, age, sex, race, body mass index (BMI), surgeon, preoperative appointment date, surgery date, California Area Deprivation Index (ADI), survey scores, rotator cuff tear tendon involvement, concurrent pathology, and additional procedures performed. California ADI was used as a proxy for patient socioeconomic status.
Statistical Analysis
Descriptive statistics were used to summarize the sample, including measures such as mean
PROMIS Anxiety T-scores were inspected via scatterplots. These scores exhibited a positive skew and underwent a natural log transformation prior to analysis. The following 3 predictor variables have been evidenced in previous literature to increase opioid usage and were included in the model: age, sex, and ADI.23,39 Forward selection stepwise regression was utilized to assess the interaction of covariates and develop the GLM. The type I error rate used for entry and exit was .15. Analysis of variance–based GLMs were conducted to evaluate the association between preoperative PROMIS Anxiety T-scores and postoperative opioid use outcomes. Separate GLMs were performed with total MMEs, duration of opioid use (in days), and MMEs per day as dependent variables. The significance of each predictor was evaluated using F-tests. All statistical analysis was completed in R statistical software (Version 4.3.2; R Project for Statistical Computing). Partial eta squared (ηp2) was calculated, representing the proportion of variance accounted for by a specific variable while controlling for other variables in the model. Statistical significance was set a priori at P < .05.
Results
A total of 64 patients were included in the analysis (Figure 2). The mean age was 63.5 ± 12.2 years (range, 31-84 years) and 32 patients (50%) were male. The mean BMI was 27.06 ± 4.67 kg/m2 (range, 20.1-42.0 kg/m2) and the mean ADI score was 3.23 ± 1.96 (range, 1.0-9.0). One patient (1.6%) had a documented preoperative diagnosis of GAD managed with 20 mg of escitalopram. All baseline characteristics can be found in Table 2.
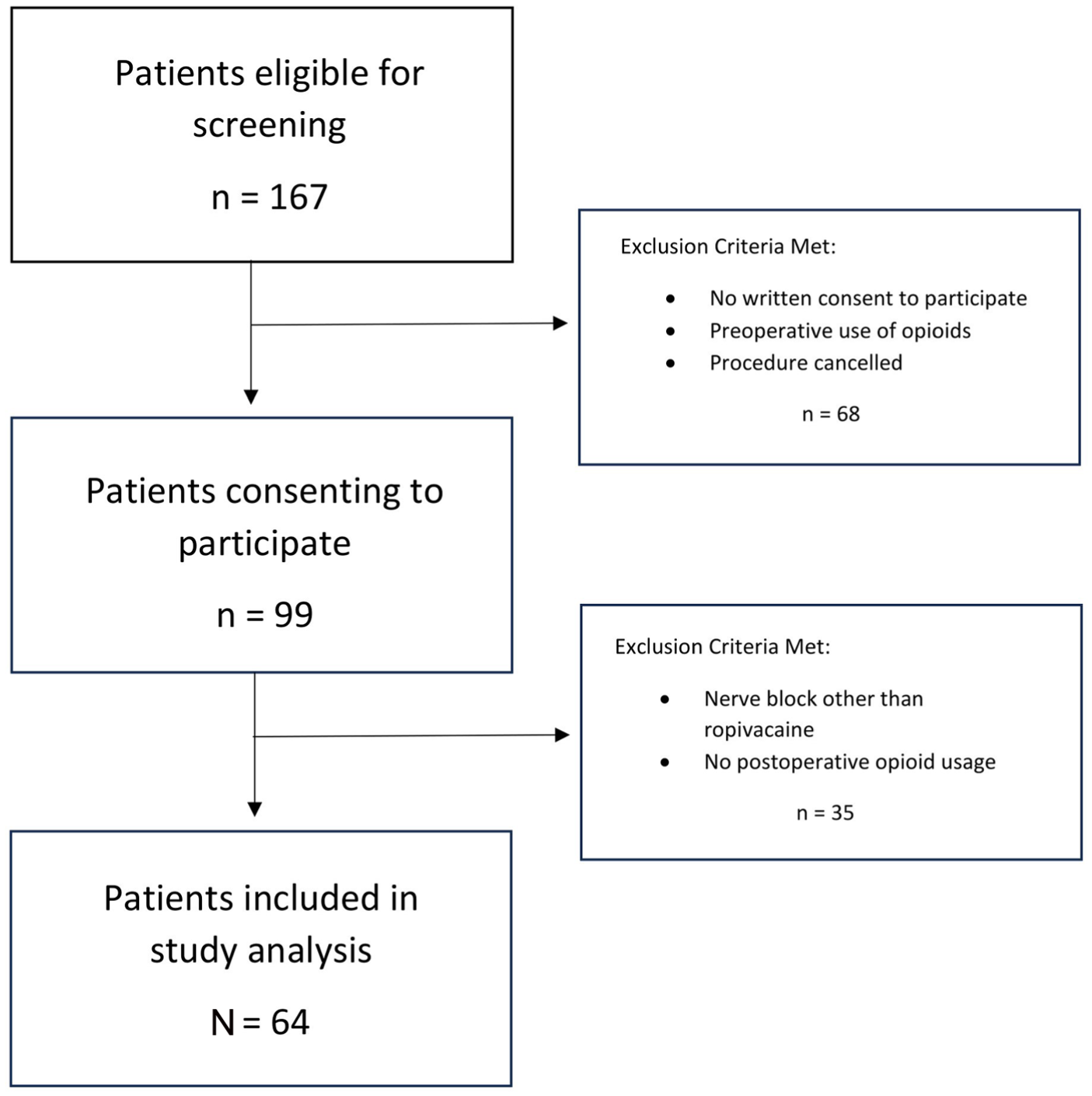
Flow diagram of patients recruited for study participation.
Patient Characteristics a
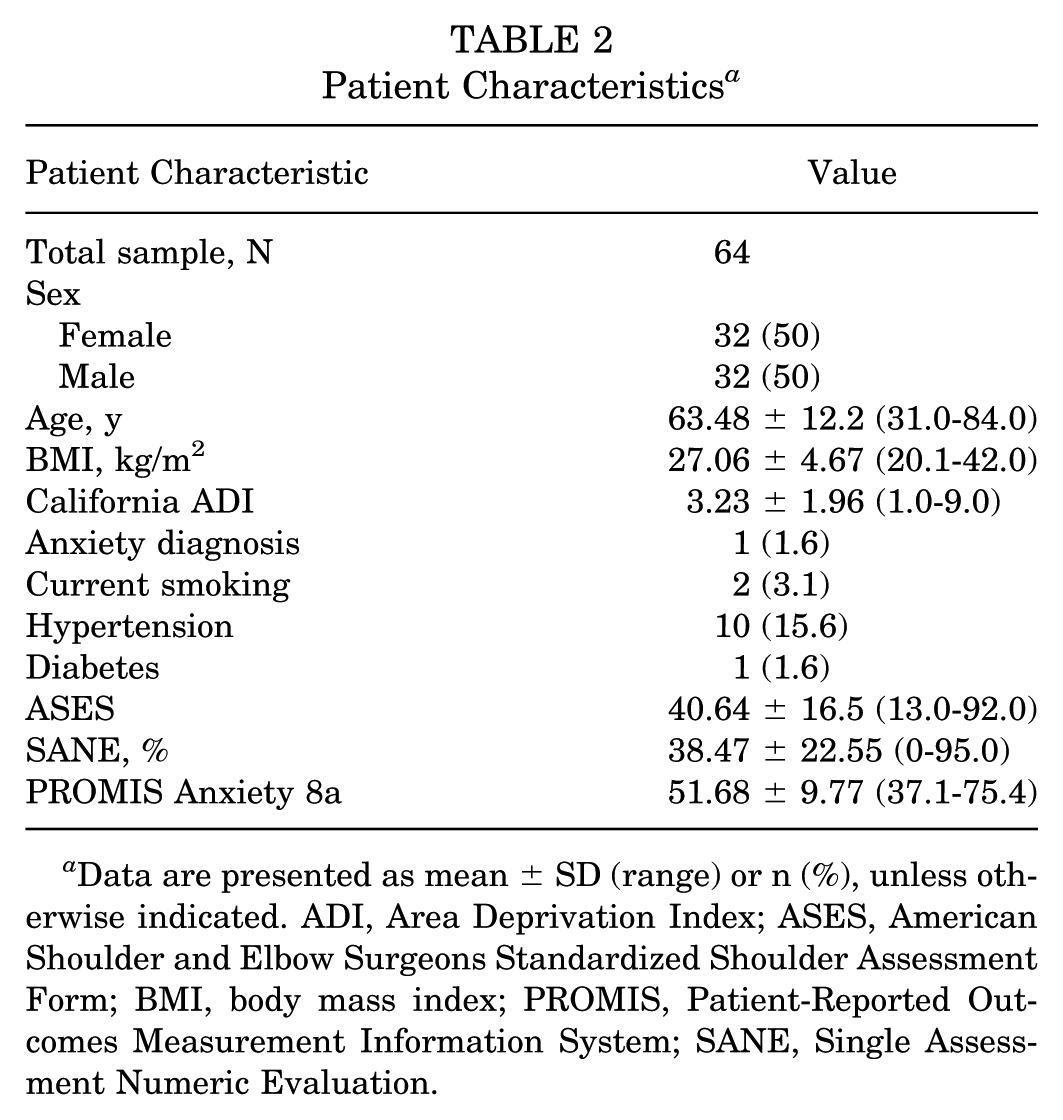
Data are presented as mean ± SD (range) or n (%), unless otherwise indicated. ADI, Area Deprivation Index; ASES, American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form; BMI, body mass index; PROMIS, Patient-Reported Outcomes Measurement Information System; SANE, Single Assessment Numeric Evaluation.
Total Postoperative Opioid Medication Usage
The mean total postoperative opioid usage was 119.46 ± 118.74 MMEs (range, 7.5-495 MMEs), with a median of 90 MMEs (IQR, 26.25-191.25 MMEs). Preoperative anxiety T-scores were not significantly associated with total opioid use (P = .15). The Pearson correlation coefficient was r = 0.22, indicating a weak positive relationship between the presence of preoperative anxiety and total MMEs. No covariates were significant. Results are summarized in Table 3.
GLM for Total Postoperative Opioid Medication Usage a

ADI, Area Deprivation Index; GLM, general linear model; MS, mean squares; PROMIS, Patient-Reported Outcomes Measurement Information System; SS, sum of squares. P < .05 indicates statistical significance.
Days of Opioid Medication Usage
Patients used opioid medication for a mean of 5.75 ± 4.66 days (range, 1-23 days), with a median of 4 days (IQR, 2-9 days). Preoperative anxiety T-scores were not significantly associated with the number of days opioids were taken (P = .13). The Pearson correlation coefficient was r = 0.18, indicating a weak positive relationship between the presence of preoperative anxiety and days opioids were taken. No covariates were significant. Results are summarized in Table 4.
GLM for Days of Opioid Medication Usage a

ADI, Area Deprivation Index; GLM, general linear model; MS, mean squares; PROMIS, Patient-Reported Outcomes Measurement Information System; SS, sum of squares. P < .05 indicates statistical significance.
Adjusted Daily Opioid Medication Usage
The mean MMEs per day was 19.04 ± 11.56 (7.5-61.9 MMEs), with a median of 16.05 MMEs per day (IQR, 10-25 MMEs). Preoperative anxiety T-scores were not significantly associated with MMEs per day (P = .58). The Pearson correlation coefficient was r = 0.13, indicating a weak positive relationship between the presence of preoperative anxiety and MME per day. No covariates were significant. Results are summarized in Table 5.
GLM for Adjusted Daily Opioid Medication Usage a

ADI, Area Deprivation Index; GLM, general linear model; MS, mean squares; PROMIS, Patient-Reported Outcomes Measurement Information System; SS, sum of squares. P < .05 indicates statistical significance.
Discussion
This prospective study investigated the association between levels of measured preoperative anxiety toward an upcoming ARCR and postoperative opioid medication utilization in patients undergoing ARCR. To comprehensively assess various dimensions of postoperative opioid utilization, 3 distinct metrics were analyzed: total postoperative opioid usage in MMEs, the total number of days postoperative opioid medication was taken, and an adjusted MME per day usage metric to account for any discrepancies between the total amount and duration of use. Our findings indicate that the presence of preoperative anxiety was not significantly associated with any of the 3 measurements of postoperative opioid utilization. These findings refute our hypothesis that in opioid-naive patients, a higher preoperative anxiety score will be associated with increased postoperative opioid use.
Previous studies have investigated the presence of preoperative anxiety within shoulder procedures, often focusing on an anxiety disorder diagnosis. Even in recent literature, these analyses have largely been confined to retrospective insurance claims databases, such as the Truven Health Analytics MarketScan database or the Premier Healthcare Database, with data derived from Current Procedural Terminology (CPT) codes, International Classification of Diseases, 9th Revision and 10th Revision (ICD-9 and -10) codes.7,15,27 Similarly, Johnson et al 20 utilized an anxiety diagnosis to identify eligible patients from a single institution registry. Quantifying the levels of patient anxiety in the preoperative setting remains a relatively novel approach with various measurement tools. Andersson et al 2 utilized a visual analog scale–style questionnaire where patients rated anxiety from 1 to 10 and Baker et al 3 employed PROMIS computer adaptive testing, whereas Longo et al 24 used the Hospital Anxiety and Depression Scale, and MacFarlane et al 26 used the patient health questionnaire (7-item GAD questionnaire). In the current study, levels of preoperative anxiety were assessed using the PROMIS SF Anxiety 8a because of the established usage and validity of PROMIS-developed surveys in shoulder surgery.14,32 The mean preoperative anxiety score was found to be 51.68, aligning with the described midpoint (50) of the PROMIS distribution curve. 19 However, despite this mean score's seemingly indicating a normal distribution, an observed positive skew and floor effect were noted. 17 This presents a significant challenge inherent in Likert scale survey designs, necessitating a natural log transformation of the anxiety T-scores to facilitate accurate comparison with postoperative opioid usage within the GLM. 10
Current literature has found that postoperative opioid consumption is influenced by multiple factors. A recent meta-analysis determined that patients >50 years of age and female patients exhibited a significantly elevated risk of increased postoperative opioid usage. 23 Similarly, Wague et al 39 identified an increased risk of prolonged postoperative opioid use in patients with a history of preoperative opioid use or those residing in areas with lower median community income. Further complicating the analysis of postoperative opioid consumption, a randomized controlled trial by Simovitch et al 36 indicated that the administration of liposomal bupivacaine and bupivacaine for an interscalene brachial plexus nerve block during ARCR was associated with a significant and sustained reduction in opioid consumption compared with a combination of ropivacaine and dexamethasone. To mitigate the influence of these confounding variables, the present study accounted for sensitive patient characteristics through interaction testing within the model. Additionally, patient characteristics were further controlled during the enrollment process by excluding individuals with preoperative opioid use or those who received a regional anesthetic block other than ropivacaine. Surprisingly, none of these factors has demonstrated a significant effect on postoperative opioid use. Despite prior literature indicating the effect of these demographic variables on opioid use, the finding of no significant effect has been previously reported. In a retrospective cohort study assessing factors affecting prolonged analgesic use, there were no significant differences in age or sex between prolonged and nonprolonged analgesic users. 29 In the present study, this finding may be attributable to the demographic characteristics of this case series, specifically the equivalent distribution of male and female patients and the low variability in both age and ADI. Similarly, rotator cuff pathology was largely homogeneous within the study cohort. All patients presented with a supraspinatus rupture, and the majority of patients exhibited concomitant involvement (ranging from partial tearing to full-thickness tearing) of the infraspinatus and/or subscapularis.
Consistent with standard practice, all dosages were converted into MME to facilitate uniform measurement across various prescribed medications. 12 In the present study, the mean postoperative opioid usage was 119.46 ± 118.74 MMEs over a period of 5.75 ± 4.66 days. These findings align with existing literature on postoperative opioid consumption following rotator cuff repair. A prospective cohort study on rotator cuff repair reported a slightly higher total of 147.5 ± 163 MMEs, originally reported as 18 (IQR, 6-35) 5 mg oxycodone pills, over 6.9 ± 5.1 days. 13 These values are considerably lower than totals of 387 ± 288 and 742.4 ± 256.5 MME reported in database studies focusing on rotator cuff repair.5,9 The elevated MME totals in these studies may be attributable to the inclusion of inpatient procedures, presenting a separate patient cohort from the present study. Furthermore, as these studies rely on CPT and ICD codes, the reported MMEs may be inflated as patients cannot be longitudinally tracked to verify exact MME usage beyond refill data. As the maximal duration of opioid consumption in this study was 23 days, we did not observe any prolonged opioid use patterns reported in other studies.15,26,29 Interestingly, a multicenter retrospective case-control study following opioid use after ARCR reported an overall median (range) duration of opioid analgesic use after discharge of 21 (5-79) days. 29 While the nonprolonged analgesia cohort reported a duration of 15 (5-15) days, both nonprolonged and prolonged cohorts could have greater duration of opioid analgesic use reflected by their respective cohort proportions of patients with preoperative narcotic analgesic use. A reported postoperative MME per day was not available in the current rotator cuff literature, limiting the ability to directly contextualize this finding. However, extrapolated MMEs per day from Garvey et al 13 provides similar results to the present study (21.38 MMEs/day vs 19.07 MMEs/day, respectively). Total MME and postoperative opioid duration following ARCR exhibited marked heterogeneity, consistent with prior literature. Such variance suggests the multifactorial nature of opioid use, driven by nuanced patient factors including pain tolerance, which remains challenging to measure clinically.
Limited research has directly linked survey-based preoperative anxiety level measurements to postoperative opioid usage. While database studies identify a diagnosed anxiety disorder to have a significant association with postoperative opioid use, this association has not been extended to encompass the presence of preoperative anxiety. MacFarlane et al 26 explored this connection in the context of total shoulder arthroplasty, assessing anxiety, depression, somatization, and pain-catastrophizing scores, and notably, including patients with preoperative opioid use. A mixed-model regression found a slightly positive correlation but no significant association between GAD-7 and total MME or opioid use duration. Like the present study, an a priori sample size estimation was conducted to ensure the validity and reliability of this nonsignificant association. As GAD remains a documented driver of postoperative opioid usage, the findings of the present study indicate that measured preoperative anxiety levels may not be a risk factor for postoperative opioid consumption. Notably, this lack of association was observed within a normal distribution of anxiety scores. Therefore, clinicians should remain vigilant regarding patients whose preoperative anxiety exceeds these normative bounds, as they may represent a distinct risk profile. A mental health diagnosis or preexisting concern should not be used to definitively categorize patients as being high risk for opioid abuse. Rather, the association between mental health conditions, such as anxiety, and opioid use simply warrants increased scrutiny of opioid prescribing practices and highlights the critical significance of vigilant surgical opioid stewardship in the context of ARCR.
Limitations
The findings of this study should be viewed considering its limitations. First, the reliance on a single Likert-type scale questionnaire, such as the PROMIS SF Anxiety 8a, to assess anxiety levels may introduce measurement bias. Quantifying anxiety levels solely through a single score can reduce accuracy and contribute to the observed floor effect in preoperative anxiety scores, potentially limiting generalizability of findings to varying patient populations. Second, the study depended on patient-reported data for pain journal entries. Despite observed patient compliance, the potential for inaccurate data entries could influence the reported postoperative opioid totals. Furthermore, although all procedures were completed in outpatient surgical centers using identical nerve blocks, opioid and multimodal medication administered prior to discharge was not recorded in the pain journal, thus remaining unaccounted for in this analysis. Opioid medication given prior to discharge could introduce a suppression of otherwise significant findings within specific patient groups, such as those with high baseline anxiety scores, thereby underrepresenting total MMEs. Despite a largely homogeneous surgical cohort, variability among surgeons, unreported perioperative factors, and standardized postoperative protocols were similarly unaccounted for in this analysis. To address these limitations, future research should incorporate multiple anxiety questionnaires within a robust randomized controlled setting, ensuring capture of perioperative opioid usage and standardization of multimodal pain control strategies. This approach would help control confounding variables and reduce potential bias. Additionally, subsequent studies could benefit from a larger patient enrollment to enable subgroup analysis, allowing for an investigation into whether the nonsignificant effect of preoperative anxiety levels on postoperative opioid use is uniform across demographic groups, specifically those that fall into distributions of PROMIS Anxiety T-scores classified as high anxiety. Future investigations should incorporate surgical factors and baseline PROM scores into a complex model with greater predictive capacity of covariates to determine the effect that concomitant procedures have on this association. Future research can measure longitudinal anxiety throughout the recovery process to investigate whether fluctuations in postoperative anxiety increase opioid utilization. Last, the baseline anxiety scores must be considered. While the T-scores in this analysis aligned with the midpoint of the PROMIS distribution curve, significantly limited scores in the 4th quartile reduce the ability of the present study to apply results to a high-anxiety population or other populations where demographics may vary significantly.
Conclusion
Levels of preoperative anxiety in opioid-naive patients undergoing primary ARCR had no significant effect on total postoperative opioid usage, the number of days opioid medication was taken, or the adjusted daily opioid usage.
Footnotes
Final revision submitted January 13, 2026; accepted February 9, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was approved by an institutional review board, WCG (study No. 1370158; tracking No. 20240564).