
Abstract
Background:
Rotator cuff tears commonly cause shoulder pain and limited mobility. Despite advances in arthroscopic repair, failures persist, often due to poor proximal humeral bone quality. While magnetic resonance imaging assesses cuff tissue, bone quality at the footprint is frequently overlooked.
Purpose:
To evaluate whether proximal humeral mean cortical bone thickness (CBTmean) on standard anteroposterior (AP) shoulder radiographs predicts anchor stability during arthroscopic repair.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This retrospective case-control study was conducted at a tertiary orthopaedic center. A retrospective evaluation was made of a consecutive series of 228 patients (46 male, 182 female; mean age, 58.32 ± 9.06 years) who underwent arthroscopic surgery for full-thickness rotator cuff tear between 2020 and 2025. Patients were separated into 3 groups based on intraoperative anchor stability: group 1 (stable anchors), group 2 (anchor repositioning required), and group 3 (anchor placement impossible due to poor bone quality managed with mini-open transosseous repair). CBTmean was measured on preoperative AP radiographs (radiographic CBTmean) and postoperative computed tomography (CT) scans (CT CBTmean) in unstable cases. Logistic regression and receiver operating characteristic curve analysis were used to determine CBTmean cutoff values.
Results:
Radiographic CBTmean was the only independent predictor of anchor instability (P = .001; odds ratio, 0.088). Cutoff values were ≤5.26 mm (sensitivity, 94.12%; specificity, 94.06%) for group 2 and ≤3.45 mm (sensitivity, 77.78%; specificity, 100%) for group 3. Age, pseudoparalysis, femoral bone mineral density (BMD), and massive tears were associated with instability, but CBTmean was most significant. CBTmean did not correlate with lumbar/femoral BMD, but radiographic and CT CBTmean showed near-perfect correlation (r = 0.992; P = .001). Intraobserver (intraclass correlation coefficient [ICC], 0.865) and interobserver (ICC, 0.898) reliability were excellent.
Conclusion:
Proximal humeral CBTmean on standard radiographs independently predicts anchor stability. Risk increases at ≤5.5 mm and becomes pronounced at ≤3.5 mm. Radiographic CBTmean assessment is a practical preoperative tool for predicting anchor stability and guiding surgical planning.
Rotator cuff tears represent a prevalent clinical challenge, frequently causing significant shoulder pain and functional limitation. With an aging population, the incidence of degenerative tears continues to rise, making effective surgical solutions increasingly important. The prevalence of degenerative tears is increasing with increased aging in society. When nonoperative treatment has not succeeded, arthroscopic treatment is now established as the standard of care for full-thickness rotator cuff tears and is commonly performed even in older patients, depending on their activity level.8,18 Despite advanced arthroscopic techniques and anchor technologies, arthroscopic repair methods can fail in some cases. Detecting the presence of severe retraction, atrophy, and fatty degeneration in the cuff tissue with preoperative magnetic resonance imaging (MRI) can provide a preoperative estimate of the repairability and success of the repair; however, the critical factor of bone quality at the anchor footprint remains largely unaddressed in preoperative planning, creating a significant gap in our ability to predict surgical outcomes. 25 The majority of patients with degenerative cuff tears are elderly, and the prevalence of osteoporosis is quite high in these patients, particularly in postmenopausal women.3,10 Traditionally, bone mineral density (BMD) is determined by dual-energy x-ray absorptiometry (DEXA) scanning of the lumbar and proximal femoral regions. However, studies have shown that proximal humeral bone density differs from that of the lumbar and proximal femur in patients with rotator cuff tears because of the development of local osteoporosis in the proximal humerus.11,12,19,28 Proximal humeral bone density measurement in these patients can be performed with DEXA specifically for this region, but this method is not standardized and is not available in most centers.11,12,19 More recently, opportunistic assessment of bone quality using Hounsfield units on shoulder computed tomography (CT) 16 and machine learning–based prediction models applied to plain radiographs 14 has been proposed. However, these promising approaches still rely on specialized imaging protocols, dedicated software for analysis, or algorithmic processing, limiting their immediate practicality in routine clinical workflows. Previous studies have reported that the more practical method of mean proximal humeral cortical bone thickness (CBTmean) measured on a standard shoulder anteroposterior (AP) radiograph, predicts greater tuberosity bone density.17,23,27
One of the most important bone-related problems that can be encountered during cuff repair in osteoporotic patients is insufficient anchor stability and, consequently, decreased arthroscopic repair success. Although Lee et al 11 reported that greater tubercle bone density is a risk factor for lateral row anchor cutting-through in the arthroscopic suture bridge technique, all patients in that study were successfully treated arthroscopically. Therefore, it is not yet clear which osteoporotic patients will have problems with anchor stability and which will not, even with proximal humeral bone density measurements, and there are insufficient data on this subject in the literature. 15 This gap in preoperative predictive capability represents a significant clinical challenge. Therefore, the aim of this study was to determine the risk factors for patients who underwent arthroscopic surgery for full-thickness rotator cuff tears but who could not achieve adequate stability even with titanium screw anchors because of insufficient bone quality, using preoperative proximal humeral radiographic CBTmean values, lumbar and proximal femoral BMD measurements, and tear- and patient-specific parameters. The hypothesis of this study was that the proximal humeral CBTmean value would be the primary determinant of anchor stability, while femoral and lumbar BMD might also be associated with it. Additionally, age, sex, the presence of pseudoparalysis, and tear size were expected to influence anchor stability.
Methods
This study examined intraoperative anchor stability as the primary outcome, with proximal humeral CBTmean as the primary predictor. Potential confounders included age, sex, tear size, BMD, and pseudoparalysis. This retrospective analysis included a consecutive series of patients who underwent arthroscopic repair for full-thickness rotator cuff tears at a tertiary orthopaedic and traumatology center between January 2020 and December 2025. The study setting included both inpatient and outpatient surgical services at this academic referral center. The study protocol received approval from the institutional review board (IRB). In accordance with IRB policy for retrospective studies, the requirement for individual patient consent was waived because of the use of anonymized data extracted from electronic health records (EHRs). The study adhered to the ethical tenets outlined in the Declaration of Helsinki. Patient data were retrospectively extracted from the institution's EHR system. The inclusion criteria were (1) patients with full-thickness atraumatic rotator cuff tear detected on preoperative MRI and treated with primary arthroscopic surgery and (2) patients who had lumbar spine and proximal femoral DEXA. The exclusion criteria were (1) patients with partial rotator cuff tears; (2) patients with full-thickness rotator cuff tears treated conservatively or with other surgical procedures; (3) patients with a history of ipsilateral shoulder surgery, infection, or trauma; and (4) patients determined to have ipsilateral benign or malignant proximal humeral bone lesions. The patients were separated into 3 groups based on the stability of the titanium anchors placed in the greater tuberosity for the repair of the supraspinatus and infraspinatus tendons, as assessed at the time of surgery. Group 1 comprised patients with stable anchor fixation. Group 2 included patients who required anchor repositioning to an alternative site within the greater tuberosity because of insufficient primary stability upon intraoperative testing. Group 3 consisted of patients in whom stable arthroscopic anchor placement was deemed impossible because of severely compromised bone quality; these cases were converted to and successfully managed with a mini-open transosseous suture tape repair. The flowchart of patient selection is shown in Figure 1.

Flowchart of patient inclusion in the study. DEXA, dual-energy x-ray absorptiometry.
Radiological Evaluations
Proximal humeral CBTmean measurements were performed on preoperative standard shoulder radiographs. In accordance with the radiographic positioning described in the foundational methodological literature, 21 the images were standard AP views acquired with the beam perpendicular to the torso and the humerus positioned to maximize the projection of the greater tuberosity, implying a neutral to slightly internal rotation. All measurements were made using calibrated digital imaging software (Synapse Radiology PACS; Fujifilm) and the previously described technique for CBTmean calculation.17,23,27 The technique involves 2 measurement levels. The first level (M1/M2) is defined as the most proximal point on the humeral diaphysis where the medial and lateral cortical borders are parallel. At this level, a perpendicular line from the outer medial to the outer lateral cortex defines the total bone diameter (M1). The width of the intramedullary canal at the same level is measured as M2. The second measurement level (M3/M4) is located precisely 20 mm distal to the first level, where the outer cortical diameter (M3) and the intramedullary canal width (M4) are measured analogously. The CBTmean is then calculated using the formula ([M1 - M2] + [M3 - M4]) / 2 (Figure 2). For patients with intraoperative anchor instability (groups 2 and 3), a postoperative shoulder CT was arranged during the study period to validate radiographic measurements, regardless of the time elapsed since surgery. CT scans were acquired on a (Siemens) scanner using a standardized protocol (slice thickness, 0.5 mm). To ensure precise anatomical correspondence between radiographic and CT-based measurements, we applied the coregistration method described by Schmidutz et al. 17 First, the perpendicular distance from the apex of the humeral head to the first radiographic measurement level was measured on the AP radiograph. This exact distance was then transferred to the multiplanar reformatted CT images. Using the coronal and axial CT reconstructions in tandem, we identified the exact coronal slice corresponding to this distance and confirmed the centering of the measurement by verifying the alignment of the medial and lateral cortices on the axial view at that level. The second measurement level was subsequently defined as 20 mm distal to this first CT level. This imaging was performed solely for research purposes and was not part of routine clinical follow-up (Figure 2). Intraobserver and interobserver reliability tests were performed using intraclass correlation coefficients for radiographic CBTmean and CT CBTmean measurements taken twice by 2 observers (S.I., O.Y.) at different times. CBTmean measurements were carried out on 2 separate occasions by 2 orthopaedic surgeons, both fellowship trained in shoulder and elbow surgery and routinely involved in preoperative radiographic planning for rotator cuff repair (S.I., O.Y.). The observers who performed the measurements were unaware of the patients’ DEXA values. All patients underwent preoperative DEXA scanning (Lunar Prodigy; GE Healthcare) using standard techniques in accordance with guidelines, and the BMD measurements were taken of the proximal femur and lumbar spine. 13 Supraspinatus muscle fatty degeneration was determined using preoperative shoulder MRI according to the Goutallier classification modified by Fuchs et al. 7 To minimize selection bias, consecutive patients meeting inclusion criteria were enrolled during the study period.

Early postoperative radiological images of the patient in whom suture anchor placement was not possible due to poor bone quality. (A) Mean proximal humeral cortical bone thickness (CBTmean) measurement from calibrated shoulder anteroposterior radiograph. The asterisk indicates knotless anchor of subscapularis tendon. (B) Proximal humeral CBTmean measurement from computed tomography scan. Identical locations were used. The arrowhead indicates the bone defect caused by failed placement of the anchor. M1 and M4, outer cortical diameter; M2 and M3, inner cortical diameter.
Surgical Procedures and Intraoperative Evaluations
All surgical procedures were performed by experienced fellowship-trained shoulder surgeons at the same tertiary center to reduce performance bias (S.I., O.Y., S.B.C.). After entering the joint through the posterior portal, subscapularis tendon tears identified during diagnostic arthroscopy were repaired with 5.5-mm knotless anchors (Doratek). The subacromial region was then accessed. During surgery, tears identified as small according to the Cofield classification were repaired in a single row, while medium, large, and massive tears were repaired with a double-row transosseous equivalent repair. 5 For the medial row, 5.0-mm titanium screw anchors (Doratek) were inserted using a standardized technique (Figure 3A). A dedicated punch (or drill) matching the anchor diameter was used to create a pilot hole at an insertion angle (“deadman's angle”) of approximately 45° relative to the bone surface. The anchor was then manually inserted until the more distal of the 2 black depth markings on the anchor body was flush with the cortical bone surface, ensuring consistent insertion depth. For the lateral row, 5.5-mm knotless polyether ether ketone anchors (PressLock Knotless Anchor; Doratek) were inserted. The number of anchors placed in the medial and lateral rows was determined during surgery according to the tear type and size. After the titanium anchor was properly inserted in the medial row, anchor stability was tested by applying mild traction to the sutures before passing the suture through the cuff tissue. If the anchor was stable (group 1), the double-row repair was performed in a routine fashion. If minimal movement or pullout was detected in the anchor (group 2), the anchor was considered unstable and removed, then placed in another location (Figure 3B). If the targeted repair was completed, the surgery was terminated, but if the titanium anchor could not be placed appropriately because of insufficient bone quality (group 3), a transosseous cuff repair was performed with a mini-open technique using suture tape.
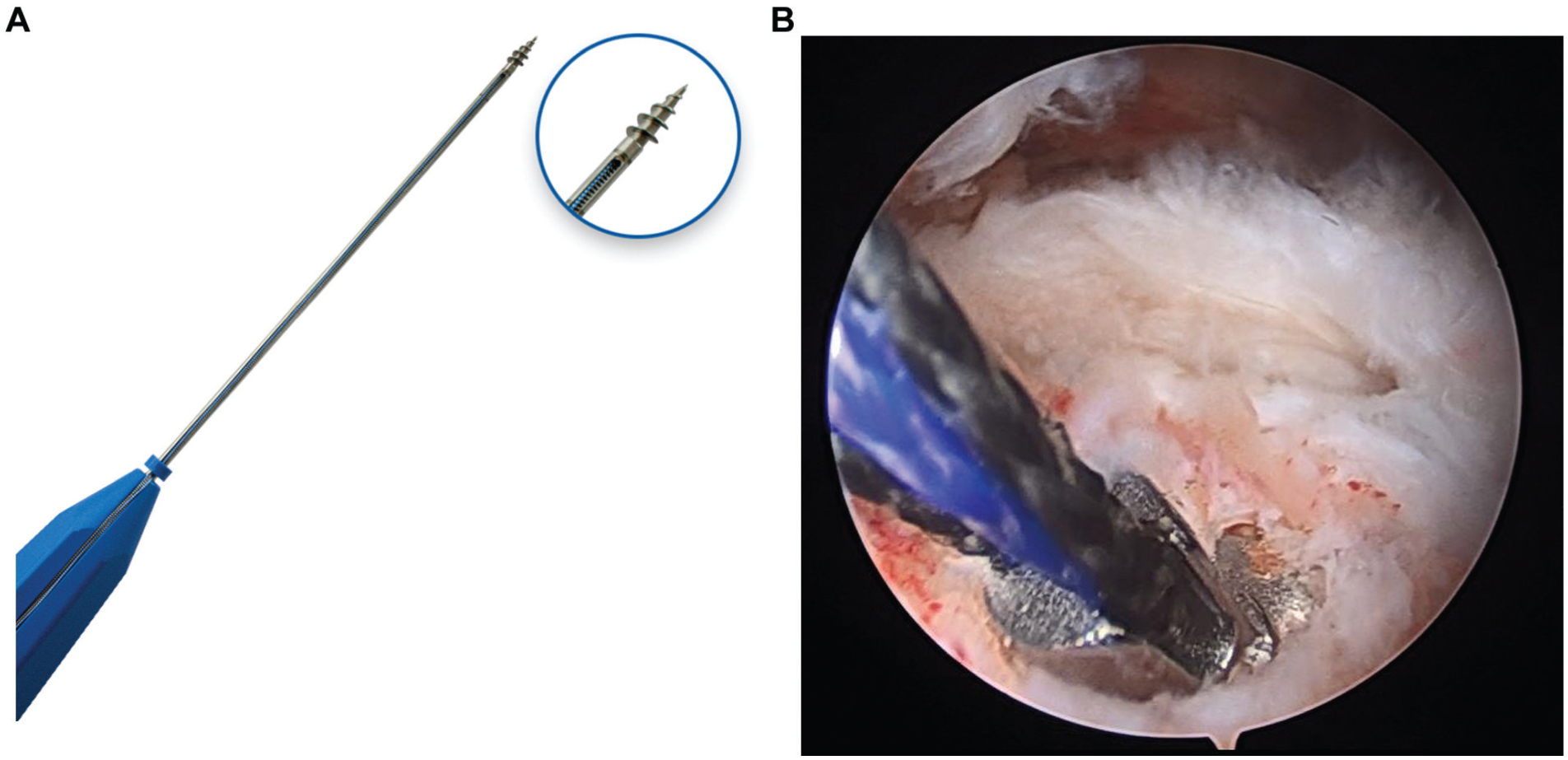
(A) The 5.0-mm titanium screw anchor used in the study. (B) Pullout of the metal screw-type anchor after applying mild traction to the sutures during surgery.
Statistical Analysis
Data analysis was performed using SPSS software (Version 29; Statistical Package for the Social Sciences). Missing data were handled using complete-case analysis, as the rate of missing values was <5% for all variables. A consecutive series of eligible patients were categorized into 3 groups based solely on intraoperative anchor stability assessment. A priori sample size calculation was performed using G*Power 3.1. Based on pilot data indicating a large effect size (d = 0.8) in CBTmean between stable and unstable anchor groups, with α = .05 and power = 0.95, a minimum of 210 patients was required. Our final cohort of 228 patients exceeded this target. Descriptive statistics were first used to summarize the data set, including measures of central tendency and dispersion (mean, median, standard deviation), as well as frequency distributions, percentages, and minimum-maximum values. The normality of quantitative variables was assessed both statistically, using the Shapiro-Wilk test, and visually, through graphical inspection.
As the assumption of normality was violated, nonparametric tests were applied for group comparisons. The Mann-Whitney U test was used to compare 2 independent groups, while the Kruskal-Wallis test, followed by post hoc Dunn-Bonferroni pairwise comparisons, was used for comparisons involving >2 groups. Categorical variables were analyzed using the Fisher-Freeman-Halton exact test. Correlations between quantitative variables were examined using Spearman rank correlation coefficient.
Multivariate analyses were conducted to adjust for potential confounding factors. The effects of various risk factors on the radiography-derived CBTmean measurement were evaluated using a linear regression model. Independent predictors of anchor stability were determined through a backward stepwise logistic regression analysis. The discriminatory ability and optimal cutoff value of CBTmean were identified using receiver operating characteristic (ROC) curve analysis. A 2-tailed P value of <.05 was considered statistically significant. To address potential concerns related to unequal group sizes, a post hoc sensitivity analysis was performed by excluding outliers (values >3 SD from the group mean). The results remained statistically significant (P < .01). Additionally, the observed effect size for CBTmean between group 1 and groups 2/3 was large (Cohen d > 1.0), supporting the clinical relevance of the findings despite smaller subgroups.
Results
Evaluations were made of 228 patients, comprising 46 male and 182 female patients, with a mean age of 58.32 ± 9.06 years (range, 37-79 years). Based on intraoperative anchor stability, patients were categorized into 3 groups: group 1 (stable anchors; n = 195), group 2 (anchor repositioning required; n = 17), and group 3 (anchor placement impossible; n = 9) (Table 1). All eligible patients meeting the inclusion criteria during the study period were included, with no exclusions because of missing data or loss to follow-up. A statistically significant difference in patient age was observed between the cohorts (P = .001), with patients in group 1 being notably younger than those in the remaining groups. Conversely, the intergroup comparisons revealed no significant disparities in sex distribution (P = .93) or the degree of fatty degeneration (P = .34) relative to anchor stability outcomes. Group 3 demonstrated a significantly higher prevalence of massive rotator cuff tears compared with the other cohorts (P = .02). In contrast, the analysis revealed no statistically significant intergroup difference in the incidence of tendon rupture (P = .06). The incidence of pseudoparalysis was higher in patients in group 3 than in the other groups, and it was higher in group 2 than in group 1 (P = .001, P = .02). The radiographic CBTmean values were statistically significantly higher in group 1 compared with the other groups, and the CT CBTmean value was significantly lower in group 3 than in group 2 (P = .001, P = .001). In the analyses comparing anchor stability between the groups, lumbar BMD showed no significant difference, whereas femoral BMD values were significantly lower in group 3 (P = .10, P = .01) (Table 1).
Demographic, Radiological, and Clinical Parameters of Patients According to Anchor Stability a

Data are presented as n (%) unless otherwise indicated. Significant values are marked with asterisks: *P < .05, **P < .01. Dashes indicate not applicable. BMD, bone mineral density; CBTmean, mean cortical bone thickness; CT, computed tomography; IS, infraspinatus tendon; SS, supraspinatus tendon; SSC, subscapularis tendon.
Kruskal-Wallis test.
Fisher-Freeman-Halton test.
Mann-Whitney U test.
Risk factors affecting anchor stability, including age, the presence of pseudoparalysis and fatty degeneration, radiographic CBTmean, femoral BMD, and lumbar BMD measurements, were evaluated using backward stepwise logistic regression analysis. After adjustment for all covariates, the only independent risk factor for anchor instability was determined to be a decreasing radiographic CBTmean measurement (P = .001; OR, 0.088; 95% CI, 0.034-0.229). Because of the statistical relationship between anchor stability and radiographic CBTmean measurements, a cutoff value was determined for this parameter related to each group. ROC curve analysis and diagnostic screening tests were used to determine the cutoff value. The cutoff value for radiographic CBTmean was determined as ≤5.26 mm for differentiation between group 1 and group 2. For the 5.26-mm cutoff value of CBTmean, sensitivity was 94.12%, specificity was 94.06%, positive predictive value (PPV) was 57.10%, and negative predictive value (NPV) was 99.50%. The area under the obtained ROC curve (AUC) was found to be 97.7% with SE of 1.9%. The ROC curve analysis established a cutoff value of ≤3.45 mm for discriminating between group 2 and group 3. This threshold demonstrated a sensitivity of 77.78%, a specificity of 100%, a PPV of 100%, and an NPV of 89.50%. The AUC was 87.9%, with an SE of 9% (Table 2 and Figure 4).
Cutoff Values for CBTmean Between Groups and Results of ROC Curve Analysis a

Significant values are marked with an asterisk: *P < .01. CBTmean, mean cortical bone thickness; ROC, receiver operating characteristic.

Receiver operating characteristic (ROC) curve analysis for cortical bone thickness (radiographic CBTmean) in predicting anchor instability. (A) ROC curve for discriminating between patients with stable anchors (group 1) and those requiring anchor repositioning (group 2). The optimal cutoff value was ≤5.26 mm, with an area under the curve (AUC) of 0.977. (B) ROC curve for discriminating between patients requiring anchor repositioning (group 2) and those in whom anchor placement was impossible (group 3). The optimal cutoff value was ≤3.45 mm, with an AUC of 0.879.
Correlation analyses revealed a moderate negative statistical correlation between age and radiographic CBTmean measurements (r = −0.460; P = .001 and P < .01, respectively). No statistically significant correlation was found between the radiographic CBTmean values and femoral BMD and lumbar BMD measurements (P > .05). A high positive statistical correlation was found between the radiographic CBTmean values and CT CBTmean values (r = 0.992; P = .001 and P < .01, respectively) (Table 3).
Correlation Analysis Between Radiographic CBTmean and Other Parameters a

Significant values are marked with asterisks: *P < .05, **P < .01. Dashes indicate not applicable. BMD, bone mineral density; CBTmean, mean cortical bone thickness; CT, computed tomography.
The reliability assessments for both radiographic CBTmean and CT CBTmean measurements demonstrated excellent intra-(0.865 (95% CI: 0.807-0.907); P < .001) and inter-observer reliability (0.898 (95% CI: 0.850-0.932); P < .001).
Discussion
The most important finding of this study was that the proximal humeral CBTmean measured on a standard AP shoulder radiograph was a significant risk factor for anchor instability during surgery. According to 2 separate cutoff values, the risk of anchor instability began when the radiographic CBTmean value was approximately ≤5.5 mm, while anchor placement was significantly more difficult when it was ≤3.5 mm. Tear size, the presence of pseudoparalysis, advanced age, and low femoral BMD were identified as risk factors for anchor instability. However, among all evaluated parameters, the radiograph-derived CBTmean measurement was the only independent predictor of anchor stability in the multivariate analysis. Anchor stability was negatively affected in patients with advanced age and reduced femoral BMD. No significant association was found between anchor stability and either sex or the presence of fatty degeneration. Furthermore, an inverse correlation was observed between age and CBTmean, whereas no correlation was detected between femoral or lumbar BMD measurements and CBTmean.
The most significant problem that can develop during arthroscopic repair due to bone tissue insufficiency is anchor pullout and repair failure.10,15 Determining the presence of local osteoporosis in this area before surgery can enable precautions to be taken regarding potential difficulties that may be encountered during surgery. Various techniques, such as using fully threaded anchors, not performing pre-anchor tapping, changing the anchor insertion angle, and performing cement augmentation, are recommended to avoid complications in the presence of osteoporotic bone. 15 Tingart et al 26 reported superior pullout strength for metal screw-type anchors over biodegradable hook-type anchors in a cadaveric model. In a retrospective study, Jung et al 9 reported that anchor pullout occurred during surgery in 3.3% of patients in the screw-type anchor group. In this study, despite the use of metal screw-type anchors with high pullout resistance, 26 anchor pullout was observed in 3.95% of patients.
Proximal humeral bone density can be measured using DEXA and quantitative CT (QCT), but the lack of use in routine practice and the high radiation exposure associated with QCT are the most significant disadvantages of these methods.11,12,19,20,23 In this study, proximal humeral CBTmean was measured, as it is a highly practical method for assessing proximal humeral bone density. Mather et al 17 reported that proximal humeral CBTmean was strongly correlated with femoral BMD. In a cadaveric study, Tingart et al 27 demonstrated a relationship between CBTmean and proximal humeral bone density. Schmidutz et al 23 found a strong relationship between CBTmean and proximal humeral bone density measured using DEXA and QCT, also in a cadaveric study. Although many studies have evaluated proximal humeral bone density, to the best of our knowledge, the current study is the first to have thoroughly evaluated the relationship between proximal humeral bone density and intraoperative anchor stability. Lee et al 11 evaluated proximal humeral bone density and cortical fractures observed during fixation of lateral anchors, reporting that all patients in that study underwent successful surgery with no anchor pullout observed during follow-up. In contrast to their findings, our study identified patients in whom anchor pullout was detected intraoperatively despite the use of metal screw-type anchors. This discrepancy may be explained by differences in anchor type (lateral knotless vs medial screw anchor), failure mechanism (cortical fracture vs anchor instability), and the bone quality metric examined (areal BMD vs cortical thickness). While Lee et al 11 highlighted the role of local BMD in cortical fracture during lateral anchor fixation, our findings emphasize that cortical thinning (CBTmean) is a critical and independent risk factor for medial-row anchor failure even before repair tension is applied. The CBTmean value, in particular, was found to be the most important and independent risk factor affecting anchor stability. In studies on the reliability of this value measured from proximal humeral AP radiographs, Schmidutz et al compared the values measured from radiographs with those obtained from CT scans and found a high correlation between the measurements. Similarly, Tingart et al, 27 in a cadaveric study, compared the CBTmean measured from radiographs with anatomical cortex thickness measurements made by cutting specimens at the same levels and found a high correlation between the 2 methods. In the current study, the correlation was analyzed between the CBTmeans measured on radiograph and on CT scans of 26 patients with intraoperative anchor instability, and a high correlation was found between the 2 methods. These data demonstrated that the radiographic CBTmean value is a practical and reliable method.
Previous studies have found different cutoff values for the CBTmean to exclude osteoporosis. Tingart et al 27 suggested a cutoff value of 4 mm, Mather et al 17 a cutoff value of 6 mm, and Skedros et al 24 a cutoff value of 5 mm. These differing values only provided information about the presence of proximal humeral osteoporosis but did not correlate with intraoperatively assessed bone quality. The current study presented 2 different cutoff values for intraoperative anchor stability and CBTmean. It was determined that even screw-type metal anchor stabilization may be quite inadequate during surgery in patients with CBTmean values of approximately ≤3.5 mm. However, with CBTmean values of approximately ≤5.5 mm, the anchor may not provide adequate stabilization at all desired locations in the humerus, and therefore, insertion at different points may be necessary. To our knowledge, this finding represents a novel contribution to the literature, though these results should be interpreted within the context of the study limitations. Its clinical significance is 2-fold: it enables the formulation of a preoperative surgical strategy by anticipating potential intraoperative challenges, and it facilitates informed patient consent by allowing for a preoperative discussion regarding the probable success of arthroscopic treatment and alternative surgical options.
Previous studies in the literature have shown that proximal humeral bone density differs from that of the lumbar and proximal femur.12,19,20 Numerous studies have shown that localized osteoporosis develops in the proximal humerus, particularly in patients with rotator cuff tears, due to limited motion and the resulting lack of mechanical stimulation.11,12,19,20 Proximal humeral DEXA and QCT measurements performed in patients with unilateral rotator cuff tears have demonstrated that bone density on the torn side was lower than on the unaffected side.12,19,20 In support of the literature, the current study results showed inadequate anchor stabilization in patients with pseudoparalysis and massive tears, demonstrating that limited motion and a lack of mechanical stimulation may lead to osteoporosis of the proximal humerus.
Lee et al 11 found that female sex, older age, and the presence of fatty infiltration were higher in cases with cutting-through, while proximal humeral bone density and tear size were independent risk factors for cutting-through. However, in the current study, the only independent factor for anchor stability was CBTmean, and anchor stability was determined to be affected in cases with older age and decreased femoral BMD. No association was found between sex and the presence of fatty degeneration. The current study results showed an inverse correlation between age and CBTmean, but no correlation was found between femoral and lumbar BMD measurements and CBTmean. Mather et al 17 found a strong correlation between proximal humeral CBTmean and femoral BMD, but a moderate correlation with lumbar BMD localized osteoporosis in the proximal humerus in patients with cuff tears has been reported to show regional differences.12,20 Lee et al 11 found that the anterior part of the greater tubercle had lower bone density than the posterior part due to cortical fracture during anterior lateral anchor fixation. Thus, the reason for the need to reposition the anchor in 7.45% of patients in this study because of instability may be explained by regional bone density differences in the proximal humerus.
Our study provides clinically actionable thresholds that can directly guide preoperative planning. When a preoperative radiograph reveals a CBTmean value at or below the identified cutoffs, surgeons should anticipate potential anchor instability and consider modifying their surgical strategy accordingly. For patients with CBTmean ≤5.5 mm, which signals an increased risk of instability, several technical adjustments can be contemplated to optimize fixation. These include (1) strategic anchor placement in regions of the greater tuberosity with higher cortical bone density, such as the proximoanterior and middle regions, as biomechanical studies suggest these areas offer superior pullout strength15,26; (2) utilizing anchors with enhanced design features for poor bone quality, such as fully threaded screws or larger diameters, to increase the bone-implant contact area4,26; and (3) considering cement augmentation techniques, where bioabsorbable or fiber-reinforced calcium phosphate cement injected through fenestrated anchors can significantly increase pullout strength, offering a valuable salvage or even primary option in compromised bone.1,21,26 For the high-risk cohort with CBTmean ≤3.5 mm, where achieving stable arthroscopic anchor fixation is highly improbable, alternative techniques that do not rely solely on screw-type anchor purchase should be planned as the primary procedure. The most robust options in this scenario include (1) the mini-open transosseous repair (with or without suture tape), which was successfully employed as a salvage procedure in all group 3 patients in the present study when arthroscopic anchor fixation was impossible6,26; (2) arthroscopic transosseous knotless techniques, which provide true transosseous fixation without anchors, thereby eliminating the risk of anchor pullout22,26; and (3) The use of broad, 2-mm braided suture tape in transosseous constructs to distribute force over a larger cortical surface area and minimize the risk of bone cutting.2,26 Proactively integrating this radiographic assessment into the preoperative workflow allows for individualized surgical planning, appropriate implant selection, and improved patient counseling regarding the likelihood of successful arthroscopic repair versus the potential need for alternative, more robust fixation methods.
Generalizability
Regarding generalizability, these findings are most applicable to patients with full-thickness rotator cuff tears undergoing arthroscopic repair at tertiary orthopaedic centers. The results may be generalizable to similar patient populations, though validation in multicenter studies would strengthen external validity.
Limitations
This study has several limitations. First, the retrospective design may introduce selection bias. Second, postoperative functional analysis was not performed, and there was no long-term follow-up. Third, although the total patient number was high compared with the literature and an a priori power analysis was performed, the number of patients with anchor instability (groups 2 and 3) was significantly smaller than in the stable group (group 1). This imbalance may reduce the statistical power of subgroup comparisons and could affect the stability of multivariate regression estimates. Nevertheless, we employed nonparametric tests and conducted sensitivity analyses to mitigate these limitations. Fourth, the inclusion criterion requiring a preoperative DEXA scan, combined with the resulting high proportion of female patients, likely biased our cohort toward individuals with a higher baseline risk of osteoporosis. This may limit the generalizability of our findings to populations with better bone quality, such as younger male patients. Additionally, we do not have data on whether patients were receiving pharmacological treatment (eg, bisphosphonates) for osteoporosis at the time of surgery, which could potentially influence proximal humeral bone quality and anchor stability. The absence of these treatment data is an acknowledged limitation of our retrospective design. Fifth, the variations of bone density in different regions of the proximal humerus were not examined in detail. Sixth, the force applied to the anchor during the stability test was not measured with a dedicated device. Finally, anchor instability was assessed only with a single anchor type, and no comparison was made with different anchor types.
Conclusion
This study demonstrated that CBTmean, measured on standard shoulder radiographs, is a reliable and independent predictor of anchor stability during rotator cuff surgery. A CBTmean value of ≤5.5 mm was associated with an increased risk of anchor instability, while values of ≤3.5 mm indicated significant difficulty in achieving stable fixation. Although advanced age, larger tear size, pseudoparalysis, and low femoral BMD also contributed to instability, only the radiograph-derived CBTmean remained an independent determinant in multivariate analysis. These findings suggest that simple radiographic assessment of proximal humeral CBTmean may serve as a practical preoperative tool for predicting anchor stability and guiding surgical decision making.
Footnotes
Final revision submitted January 25, 2026; accepted February 2, 2026.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kartal Dr. Lutfi Kirdar City Hospital institutional review board (approval No. 2025/010.99/18/10)).