
Abstract
Background:
Recurrent lateral patellar instability is common in adolescent patients, often requiring surgical intervention. Medial quadriceps tendon femoral ligament reconstruction (MQTFLR) has emerged as an alternative to medial patellofemoral ligament reconstruction, avoiding patellar fixation and its associated complications. However, data on short-term clinical outcomes and return to activity (RTA) following MQTFLR in adolescent patients remain limited.
Purpose:
To evaluate short-term clinical outcomes and RTA following MQTFLR in adolescent patients with recurrent lateral patellar instability.
Study Design:
Case series; Level of evidence, 4.
Methods:
Adolescent patients (≤19 years) who underwent primary allograft MQTFLR at a single institution between 2017 and 2023 were retrospectively reviewed. Inclusion criteria required both pre- and postoperative patient-reported outcomes (PROs) with a minimum 1-year follow-up. The primary outcome was the change from baseline in PROs, including scores on the Pediatric International Knee Documentation Committee Subjective Knee Evaluation Form (Pedi-IKDC), the Tegner Activity Scale, and the Lysholm Knee Scoring Scale. RTA rates and complications were also assessed. A Wilcoxon signed-rank test was used to compare pre- and postoperative PROs, with P≤ .05 considered statistically significant.
Results:
A total of 43 patients (mean age 15 ± 1.8 years, 58% female) underwent MQTFLR. Multiple preoperative dislocations were reported in 63%, and 23% underwent simultaneous tibial tubercle osteotomy. Median follow-up was 24.0 months (IQR, 12.6-24.3). RTA data were available for 33 patients, with 82% attempting to return to their primary activity and 89% of those returning at the same or higher level. Statistically significant improvements were observed in Pedi-IKDC (58.70 [50.55-67.94] to 95.65 [80.98-98.37]; P < .001), Tegner (3.00 [2.00-4.00] to 8.00 [5.50-9.00]; P < .001), and Lysholm (74.00 [54.50-83.50] to 95.00 [85.00-100.00]; P < .001) scores. Three patients (6.9%) experienced recurrent patellar instability at an average of 33.4 months postsurgery.
Conclusion:
MQTFLR is a safe and effective surgical option for adolescent patients with recurrent lateral patellar instability, resulting in significant improvements in PROs and a high rate of RTA at the same or higher level. Further research is needed to assess long-term outcomes and identify factors that may influence postoperative recovery.
Keywords
Lateral patellar dislocation with associated patellar instability is a common acute knee injury in adolescent populations and a prevalent developmental knee pathology, with an annual incidence of 23 to 43 per 100,000.1,2,19,25 Beyond causing discomfort and functional limitations, recurrent instability can lead to long-term patellofemoral joint degeneration and arthritis if untreated.14,24,26,36 The primary clinical challenge is preventing further dislocations while preserving knee function, particularly in physically active patients.
The medial patellofemoral ligament (MPFL) plays a crucial role in stabilizing the patella during early flexion, and its insufficiency is a major contributor to recurrent patellar dislocation.2,10 MPFL reconstruction (MPFLR) has long been the surgical standard for managing patellar instability by restoring the ligament's integrity.11,17,18 While MPFLR has demonstrated favorable outcomes in reducing instability and improving function, it has also been associated with persistent patellar morbidity in up to 21% of cases.13,35 Additionally, the use of bone tunnels for patellar fixation increases the risk of complications such as patellar fractures, especially in younger patients with smaller patellae.12,15,20
Recent anatomic and biomechanical studies have identified the medial quadriceps tendon femoral ligament (MQTFL) as a key secondary stabilizer of the patella, particularly in full extension.4,7 MQTFL reconstruction (MQTFLR) offers an alternative approach that avoids patellar fixation by anchoring the graft to the quadriceps tendon, potentially reducing complications.30,32,37 Compared with MPFLR, MQTFLR has demonstrated a closer restoration of native patellofemoral stability and may provide a more anatomically favorable option for patellar stabilization. 34 Although research has shown no statistical advantage between MQTFLR and MPFLR in recurrence rates or patient-reported outcomes, advocates of MQTFLR highlight its ability to restore native knee function without patellar fracture risk. 33
MQTFLR has been described as a promising alternative to traditional MPFL reconstruction, but evidence in adolescent populations remains limited. This study builds on existing work by specifically evaluating short-term clinical outcomes and return to activity in adolescents following MQTFLR. We hypothesize that MQTFLR is a viable surgical option that minimizes complications while optimizing knee function and patella stability.
Methods
Patient Selection
Prior to the initiation of this retrospective study, institutional review board approval was obtained. Adolescent patients who underwent allograft MQTFLR between March 1, 2017, and August 1, 2023, at a single children's hospital were identified. Patients aged 10 to 19 years were included, consistent with World Health Organization guidelines of adolescence. 1 Patients were included in this study if they (1) underwent primary hamstring allograft MQTFLR, (2) had both pre- and postoperative patient-reported outcomes (PROs), and (3) had a minimum of 12-month follow-up. Patients with additional pathology, such as meniscal and chondral/osteochondral injuries and loose bodies, were included, as well as those with concomitant procedures (eg, tibial tubercle osteotomy, hemiepiphysiodesis). Patients with bilateral patellar instability at the initial evaluation or those who later developed contralateral instability prior to their 12-month follow-up were excluded from this study. Additional exclusion criteria for this study included (1) a history of ipsilateral or contralateral lower extremity surgery and (2) trochleoplasty. A detailed flow diagram is included in Figure 1. In total, 44 patients met the inclusion criteria.

Patient selection.
Surgical Technique
All surgical procedures were performed by a pediatric and sports medicine fellowship-trained orthopaedic surgeon. Surgeries were performed using combined general and regional anesthesia; tourniquets were used to control blood loss. Intraoperative examination under anesthesia induction included applying lateral forces to the patella at 30° of knee flexion and beyond to determine the degree of lateral subluxation. The decision for concomitant correction of genu valgum was determined at the discretion of the senior author (M.G.S); when indicated, hemiepiphysiodesis was performed prior to arthroscopy.
Next, an arthroscopic evaluation was performed by assessing patellar stability, patellofemoral motion, and the necessity for a lateral realignment procedure. 29 At this time, chondral/osteochondral injuries were identified and addressed if needed. Additionally, concomitant tibial tubercle osteotomy with or without distalization was conducted at this time. 27 The decision for distal realignment was made at the discretion of the senior author on a case-by-case basis, as determined by preoperative (physical examination and radiologic assessment) and arthroscopic evaluation. Strict numerical cutoffs of radiologic parameters (eg, tibial tubercle–trochlea groove [TT-TG] distance) were not incorporated into a treatment decision-making algorithm.
MQTFLR was performed using the technique described by Bui et al. 6 Typically, a gracilis allograft tendon was used to reconstruct the MQTFL. 13 In some cases, depending on the size and age of the patient, a semitendinosus tendon was chosen. Following a longitudinal incision centered over the length of the patella, two 1-cm parallel incisions approximately 1 cm apart were made along the central-most aspect of the quadriceps tendon just proximal to the patella. A hemostat was used to develop an interval between the 2 incisions, and a passing suture was placed. A longitudinal incision was then made in the medial retinaculum just distal to the level of the vastus medialis obliquus. A tunnel was created to develop the plane between the second and third layers of the knee, with care taken to ensure it remained superficial to the joint capsule. Next, a 3- to 4-cm longitudinal incision was centered along the adductor tubercle and the medial epicondyle. The insertion of the MQTFL was palpated at the valley between the adductor tubercle and the medial epicondyle, and the femoral tunnel was created with a passing pin and cannulated reamer. The allograft was woven through the 2 parallel slits in the quadriceps tendon to create a pulley along the intact segment of the quadriceps tendon; the free ends of the graft were shuttled through the retinacular tunnel, exiting at the MQTFL insertion site and passed into the femoral tunnel. After cycling the knee through full range of motion, the knee was placed on a radiolucent triangle in approximately 45° of flexion with the patella reduced in the trochlea. The graft was secured with an interference screw in standard fashion.
Postoperative Rehabilitation
Postoperative rehabilitation began 3 to 7 days after surgery and followed a structured 6-phase protocol. Patients were allowed weightbearing as tolerated while ambulating in a hinged knee brace locked in extension; the brace was removed for home exercises, physical therapy, and bathing. When approved by insurance, continuous passive motion was initiated immediately until 120° of knee flexion was achieved. Emphasis was placed on proprioceptive training and closed-chain quadriceps strengthening to enhance limb confidence and normalize gait patterns. After week 12, rehabilitation continued with progressive strengthening, plyometric drills, and jump progression exercises. In the final return-to-sport phase, patients engaged in sport-specific drills and simulated practice situations. When applicable, patients underwent formal strength and functional testing to assess readiness for return to sports and activities. 28 The ultimate decision for clearance to return to activity (RTA) was determined by the senior author based on the overall performance on the RTA assessments (when applicable), discussions with the patient/family and rehabilitation team, and consideration of the patient's sport and activity level.
Data Collection
Medical records were reviewed, and demographics (eg, age, sex, primary activity, and presence of bilateral instability) were recorded. Radiographic data and surgical details (eg, graft type, additional diagnoses, additional procedures, tourniquet time) were documented. PROs were collected using validated instruments, including the Lysholm Knee Scoring Scale, Pediatric International Knee Documentation Committee Subjective Knee Evaluation Form (Pedi-IKDC), and Tegner Activity Scale. RTA data were obtained through structured clinical questioning during routine postoperative visits, including time from surgery, when patients attempted return to primary activity, level of return, and reasons for not attempting or returning at a lower level of activity. Validated RTA scales or predefined criteria were not used. Postoperative complications were identified through clinical documentation and recorded according to the Clavien-Dindo classification scale. 9
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation or median and interquartile range, depending on their distribution, and categorical data were expressed as frequencies and percentages. Due to the nonnormal distribution of the data, a Wilcoxon signed-rank test was used to assess the pairwise difference between pre- and postoperative PROs, and P values <.05 were considered statistically significant. 23 All statistical analyses were conducted using R (version 4.4.1; R Foundation for Statistical Computing).
Results
Patient Characteristics
Patient characteristics are summarized in Table 1. In total, 43 individuals underwent MQTFLR during the study period and met the inclusion criteria. The mean age at the time of surgery was 15 years (range, 12-19 years). Few patients (26%) reported no primary activity, indicating many were involved in structured sports. Among those who did report a primary activity, basketball was the most common (21%), followed by soccer (19%). A variety of secondary sports were mentioned, with gymnastics, martial arts, and volleyball being the most frequent, each accounting for 3% to 5% of responses. Other activities, such as baseball, softball, skiing/snowboarding, dance, and swimming, appeared less frequently, each representing a small portion of the sample.
Demographic Data a
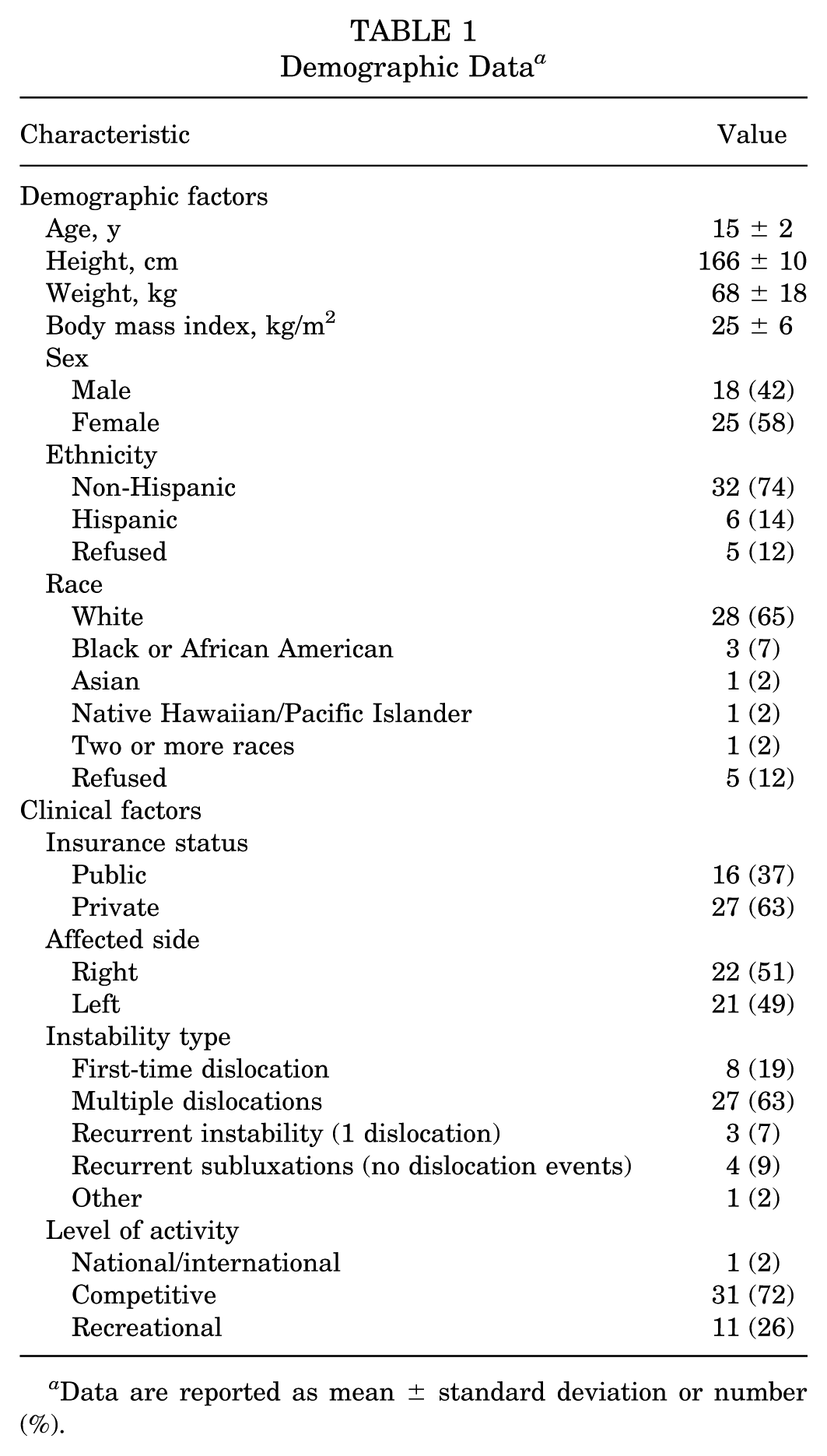
Data are reported as mean ± standard deviation or number (%).
Surgical Findings
Surgical findings are reported in Table 2. Gracilis allografts were used in 95.3% of patients. The most performed concomitant procedures were chondroplasty (77.3%) to address osteochondral injuries and lateral release and repair (65.9%).
Surgical Variables a

Data are reported as mean ± standard deviation or number (%). LFC, lateral femoral condyle; LR&R, lateral release and repair; TTO, tibial tubercle osteotomy.
Imaging Characteristics
Imaging characteristics are summarized in Table 3. Presurgical radiologic findings found average mean measurements for magnetic resonance imaging–based TT-TG distance and Caton-Deschamps Index of 14 ± 5.9 mm and 1.2 ± 0.18, respectively.
Radiological Characteristics a

Data are reported as number (%). MRI, magnetic resonance imaging.
Type A: shallow or symmetric convex trochlea.
Type B: flat or convex trochlea.
Type C: asymmetry of the trochlear facets, convex lateral facet, and hypoplastic medial facet.
Type D: asymmetry of the trochlear facets and vertical slope “cliff” pattern.
Outcomes
RTA data were available in 33 patients; median follow-up time was 24.0 months (IQR, 12.6-24.3). In total, 27 patients (81.8%) attempted return to activity postoperatively, and 6 (18.2%) did not attempt return, with 3 (50%) citing personal reasons, 1 (16.7%) due to fear, 1 (16.7%) due to pain, and 1 (16.7%) not reported. Of the patients who attempted return, 16 (59.3%) were able to return at the same level and 8 (29.6%) at a higher level of activity. Three patients (11%) did not return to their primary activity after attempting: 1 (33.3%) due to personal reasons, 1 (33.3%) due to pain, and 1 (33.3%) not reported. PROs were obtained at a median follow-up of 24 months (IQR, 12.7-24.3; n = 43). Statistically significant improvements were observed in Pedi-IKDC, Tegner, and Lysholm scores. Table 4 compares pre- and postoperative PROs to evaluate functional and clinical improvements following surgery.
Pre- and Postoperative Patient-Reported Outcome Change a
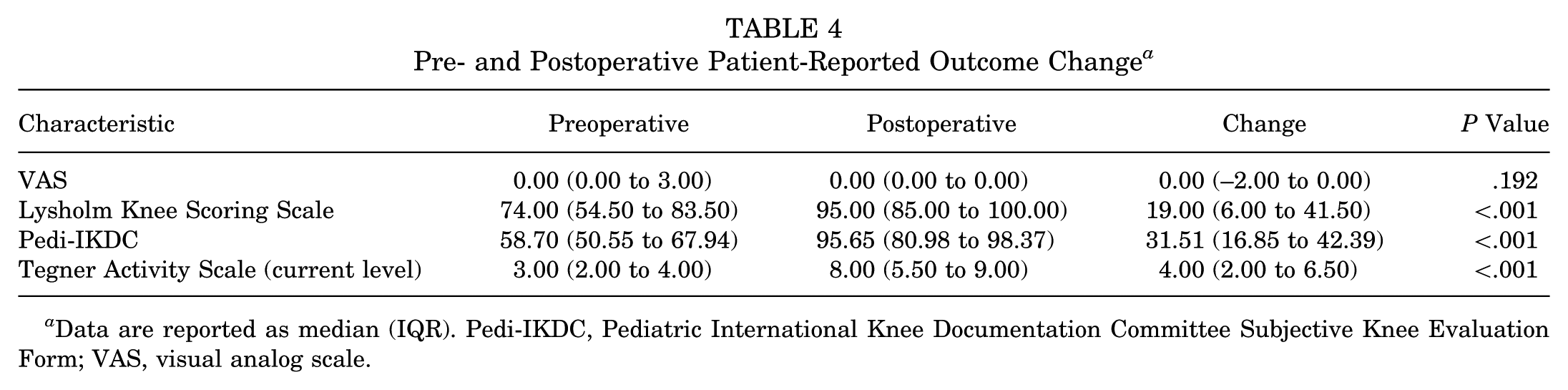
Data are reported as median (IQR). Pedi-IKDC, Pediatric International Knee Documentation Committee Subjective Knee Evaluation Form; VAS, visual analog scale.
Complications
Observed complications included 3 cases (6.9%) of recurrent instability, occurring at 13.1, 33.1, and 53.9 months postoperatively. Additionally, 1 patient (2.3%) underwent MQTFLR with a concomitant tibial tubercle osteotomy (TTO) and developed a transverse, nondisplaced fracture 5.2 months postoperatively at the base of the inferior TTO screw. All 4 complications were classified as Clavien-Dindo grade III and required surgical intervention.
Discussion
The findings of this study support MQTFLR as a safe and effective surgical intervention for adolescent patients with recurrent lateral patellar instability. Patients demonstrated significant postoperative improvements in Lysholm, Pedi-IKDC, and Tegner scores, supporting the effectiveness of MQTFLR in restoring knee function and stability. These findings align with prior MQTFLR studies, including Bowman et al, 5 who reported a mean Lysholm score of 97 at 29 months postoperatively, with Tegner scores returning to preoperative levels.
By securing the graft to the quadriceps tendon, MQTFLR preserves native biomechanics while eliminating the need for patellar fixation.3,5,8,35 These results align with previous studies that have advocated for this technique as a reliable alternative for addressing patellar instability. 5 Although MPFLR remains a widely used procedure, its reliance on patellar fixation introduces the potential for fixation-related complications, particularly in skeletally immature patients.20,31,32 Given these findings, MQTFLR emerges as a reliable alternative that effectively addresses patellar instability while maintaining anatomic integrity and promoting favorable clinical outcomes.
With 81.8% of patients attempting return and 88.9% returning at the same or higher level of performance, the RTA rates observed in this study are comparable to, and in some cases exceed, previously reported outcomes for MPFLR. Of the patients, 18.2% chose not to attempt RTA, a decision predominantly driven by personal preference (50%) rather than surgery-related factors (ie, fear of reinjury), with only 1 patient (16.7%) citing pain as a deterrent. Prior MPFLR meta-analyses have cited RTA rates ranging from 55.6 to 84%. 22 Platt et al 21 reported MPFLR RTA rates exceeding 90%, although 30% of those patients returned at a lower level of activity. A previous MPFLR meta-analysis identified fear of reinjury as the primary barrier to return, with 6 of 12 studies identifying fear of reinjury as the most common factor and 39.7% of patients citing it as their main reason in another.21,22 This suggests that while MQTFLR successfully restores physical function, nonsurgical factors such as psychological readiness or personal priorities can influence the decision to return to activity.
Notable complications included 3 cases (6.9%) of recurrent instability, occurring at 13.1, 33.1, and 53.9 months. These rates are comparable to or lower than recurrence rates reported in the MPFLR literature. Shah et al 32 reported a 3.7% failure rate and 8.3% of patients showing patellar hypermobility, episodic instability, and apprehension. Similarly, in a meta-analysis from Jackson et al, 16 failures following MPFLR were reported as high as 10.7%, with fractures occurring at rates up to 8.3%. One individual (2.3%) in our dataset experienced a tibial fracture at the site of the inferior TTO screw, underscoring the potential for stress-related complications following MQTFLR with TTO. These finding suggests that MQTFLR provides stable patellar fixation in most cases, with recurrence rates in line with existing MPFL data. However, future studies will need to explore whether specific technical factors, concomitant procedures, and patient demographics contribute to the observed complications.
Several important limitations should be considered when interpreting these findings. Retrospective design and reliance on available clinical records resulted in exclusion of a large proportion of patients who underwent MQTFLR due to incomplete data or loss to follow-up, introducing a meaningful risk of selection bias. Patients lost to follow-up may have experienced inferior outcomes compared to the analyzed cohort, potentially leading to an overestimation of favorable PROs and RTA rates. Second, the relatively short duration of clinical follow-up limited the ability to detect late adverse outcomes, such as recurrent instability. Notably, the median time to recurrent instability exceeded the median follow-up time, suggesting failures may have occurred after the final clinical follow-up, resulting in underestimation of the true recurrence rates. Third, although PROs were obtained using validated, standardized instruments, RTA and complication data were derived from structured, although nonvalidated, clinical questioning during routine postoperative visits rather than formalized follow-up interviews. Clinicians assessed whether patients had returned to their primary activity and inquired about postoperative complications; however, the absence of predefined criteria or standardized measurement tools increases the likelihood of detection and measurement bias. While clinically significant complications requiring further evaluation or intervention were likely captured, minor, delayed, or subclinical instability events may have been underrepresented. Additionally, the lack of a control or comparison group limits causal inference regarding MQTFLR effectiveness. Improvements in RTA and PROs found in this analysis may reflect rehabilitation, natural recovery, or concurrent surgical interventions rather than the reconstruction itself. Furthermore, potential variability introduced by concomitant procedures and diagnoses represents an important source of confounding. Patients undergoing additional intra- and extra-articular procedures, such as TTO, may experience a different trajectory of recovery and functional outcomes. Coexisting pathologies, such as cartilage defects, have the potential to influence RTA timelines and PRO scores, posing a challenge to isolate the improvement from MQTFLR alone. The available sample size lacked sufficient power to permit subgroup analysis stratified by these factors. Finally, the exclusive use of allograft tissue limits the generalizability of these findings. While allografts were selected to minimize donor site morbidity, variability in graft incorporation and biological healing may influence both short- and long-term outcomes.
Conclusion
MQTFLR is a safe and effective surgical option for adolescent patients with recurrent lateral patellar instability, resulting in significant improvements in PROs and a high rate of RTA at the same or higher level. Further research is needed to assess long-term outcomes and identify factors that may influence postoperative recovery.
Footnotes
Final revision submitted January 24, 2026; accepted January 31, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.G.S. received educational support from Arthrex and Smith & Nephew. Research reported in this publication was supported by Seattle Children's ASPIRE program. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Seattle Children's Research Institute (STUDY00004152).