
Abstract
Background:
Mechanical symptoms, such as catching, locking, and giving out, are common concerns for patients with acetabular labral tears prior to hip arthroscopy. Yet the rate at which they resolve following hip arthroscopy remains poorly understood.
Purpose:
To use the Nonarthritic Hip Score (NAHS) to evaluate the rate at which mechanical symptoms resolve after primary hip arthroscopy for patients with symptomatic labral tears.
Study Design:
Case series; Level of evidence, 4.
Methods:
This was a retrospective review of prospective data for patients who underwent primary hip arthroscopy from May 2014 to March 2023. Mechanical symptoms were assessed using 3 NAHS items: catching or locking, giving out, and stiffness, each rated on a Likert scale (0-4). Patients who reported preoperative scores of ≤3 were classified as symptomatic, while patients with a 4 were classified as asymptomatic. Symptom resolution was defined as improvement to a score of 4 after surgery at 24 months postoperatively. Univariate analyses identified factors associated with symptom resolution, and a multivariate logistic regression was used to determine independent predictors. Functional outcomes were compared between groups with resolved and persistent symptoms using NAHS subscales.
Results:
Among 228 patients (age range, 18-64 years), stiffness was the most common preoperative symptom (85.5%), followed by catching/locking (65.8%), and giving out (36.4%). At 24 months, resolution rates were 80.7% for giving out, 59.3% for catching/locking, and 29.7% for stiffness. For patients who were asymptomatic at baseline, very few patients developed symptoms of catching/locking or giving way (14.1% and 4.1%, respectively); however, 45.5% of patients who reported no stiffness at baseline reported some at 24 months. Multivariable analysis identified lower Tönnis angle and higher center-edge angle as independent predictors for resolution of giving out. Patients with resolved mechanical symptoms demonstrated significantly higher NAHS subscores for the majority of items at 2 years compared to those with persistent symptoms (P < .05).
Conclusion:
Hip arthroscopy efficiently resolves mechanical symptoms such as catching/locking or giving out while significantly improving functional outcomes. However, persistent stiffness was a common postoperative issue. Patients should be informed preoperatively that residual stiffness may improve with surgery but not be completely alleviated.
Hip arthroscopy is commonly employed for patients with symptomatic labral tears secondary to femoroacetabular impingement (FAI). 13 The diagnosis of labral tears often depends on a combination of clinical examination, physical findings, and imaging. Symptoms can include hip or groin pain, accompanied by complaints of mechanical symptoms such as catching, locking, instability, giving out, and stiffness. 30 The primary objectives of hip arthroscopy are to alleviate the pain and mechanical symptoms associated with labral tears, while restoring the hip to its normal function and morphology. 27 While hip arthroscopy is often successful in alleviating pain and correcting pathological morphology, 6 the extent to which hip arthroscopy can alleviate mechanical symptoms remains poorly understood and is not routinely measured in outcome studies.
Mechanical symptoms often arise in the hip due to structural abnormalities. FAI can cause pathological contact between the acetabular rim and femoral head, creating damage to the labrum, articular cartilage, and bone. 28 As a result of this damage, small fragments of bone or cartilage can dislodge into the joint space, which can cause a grinding sensation. 39 Additionally, the abnormal contact between the articulating surfaces in the hip joint can cause the mechanical symptoms of catching, clicking, or locking. 1 Other possible pathologies such as capsular laxity, ligamentum teres tears, chondral lesions, or synovial inflammation may alter joint mechanics and result in symptomatic giving way. 7 Furthermore, patients with pathological hips may experience comparatively limited range of motion, contributing to feelings of stiffness.9,14
Most hip arthroscopy outcome studies emphasize improvements in pain and range of motion using validated scoring systems, such as the modified Harris Hip Score, Hip Outcome Score, or the International Hip Outcome Tool. However, these scales do not explicitly capture the presence, severity, or resolution of mechanical symptoms such as catching, clicking, or instability. 34 Thus, the relief of mechanical symptoms is often not explicitly reported in most functional outcomes studies of hip arthroscopy. Mechanical symptoms are commonly cited by patients as preoperative complaints, yet their clinical significance and trajectory after surgery remain poorly studied. A more comprehensive understanding of how these symptoms respond to arthroscopic treatment could help refine surgical indications, manage patient expectations, and improve postoperative counseling.
Mechanical symptoms have been extensively studied in the context of knee arthroscopy, with prior work by Sayegh et al 32 demonstrating their prevalence and resolution following surgical intervention. This study uses a similar methodological approach to investigate whether comparable patterns of symptom resolution are observed in patients undergoing hip arthroscopy. Thus, the purpose of this study is to (1) evaluate the prevalence of mechanical symptoms in hip arthroscopy patients and the rates at which they resolve, (2) evaluate possible independent predictors of symptom resolution or persistence, and (3) assess the effect of symptom resolution using the Nonarthritic Hip Score (NAHS), thus assessing overall hip function.
Methods
Study Design
This was a retrospective review of prospectively collected data from May 2014 to March 2023 of patients who underwent hip arthroscopy by a single surgeon. This study was approved by our institutional review board (IRB# 2013P001442 & 2019P002191). Inclusion criteria for this study were patients undergoing primary hip arthroscopy for treatment of symptomatic acetabular labral tears or FAI, those who were ≥18 years of age at the time of surgery, and patients with completed patient-reported outcome measure data on mechanical symptoms at baseline and 2-year follow-up. Patients were excluded if they had a Tönnis grade >2 or hip dysplasia defined by a lateral center-edge angle (CEA) of <20°. This study was carried out in accordance with relevant regulations of the US Health Insurance Portability and Accountability Act.
All patients who visited the clinic for assessment of acetabular labral tears underwent the same physical evaluation. This included flexion-adduction-internal-rotation and flexion-abduction-external rotation to identify limitations of pain or motion. 12 Patients also received hip radiographs (anteroposterior pelvic view, anteroposterior lateral view of the affected hip, and Dunn lateral view). Patients were administered a diagnostic and therapeutic intra-articular corticosteroid injection, magnetic resonance arthrography, and a minimum of 3 months of formal physical therapy. Patients whose symptoms did not resolve with conservative treatment were indicated for hip arthroscopy.
Abbreviated Surgical Technique
Throughout this study, the senior surgeon (S.D.M.) exclusively used the puncture capsulotomy technique for hip arthroscopy.11,29 Under general anesthesia, patients were placed supine on a hip distraction table. First, the anterolateral portal was created using intra-articular distention under fluoroscopic guidance, followed by the midanterior, anterior, and Dienst portals. In order to enhance visualization of anteromedial or lateral cam lesions, an additional portal was made to enhance visualization. The hip was arthroscopically assessed for damage to the labrum and chondrolabral junction breakdown. Labral repair was performed if adequate tissue remained for suture fixation. Bone marrow aspirate concentrate (BMAC) was used as an adjuvant for hip arthroscopy for chondrolabral junction breakdown, chondral lesions, or Outerbridge grade ≥2 lesions, as well as shared decision-making between the patient and the senior surgeon. All additional costs associated with the use of BMAC were covered by the Conine Family Fund for Joint Preservation, a philanthropic organization without financial ties to industry.
Postoperative Rehabilitation Protocol
All patients underwent the same 5-step 6-month self-guided rehabilitation protocol. 24 This protocol did not include any formal physical therapy or bracing. Patients were given crutches to allow for immediate weightbearing with a flat-foot gait following surgery. At 6 weeks, patients were instructed to use a stationary bicycle with no resistance. At 10 weeks, patients could swim or use an elliptical on light resistance as tolerated. At 4 months, low-weight, high-repetition hamstring curls and leg press exercises were encouraged. Patients could resume impact-loading activities at 6 months postoperatively.
Data Collection
Demographic data were collected from the electronic medical record at the time of surgery, including age, sex, body mass index (BMI), and hip laterality. Intra-articular pathology, including acetabular cartilage condition, labral condition, and chondrolabral junction breakdown were assessed arthroscopically using the Outerbridge classification. Surgical procedures performed, including labral debridement, repair, or augmentation and acetabular and/or femoral osteoplasty, were recorded from the operative note. 26 Preoperative radiographs were also evaluated for osseous pathology (cam or pincer lesions), Tönnis grade, and CEA. Patients were sent the NAHS survey at enrollment and postoperatively at 3-, 6-, 12-, and 24-month intervals.
Mechanical Symptoms and Statistical Analysis
Three items from the NAHS were used to assess mechanical symptoms: (1) "Catching or locking of the hip?", (2) "Does your hip give out on you?", and (3) "Stiffness in your hip?" Responses to each item were graded on a 0- to 4-point Likert scale, with scores assigned as follows: 4 = none, 3 = mild, 2 = moderate, 1 = severe, and 0 = extreme. 4 The proportion of patients reporting mechanical symptoms prior to hip arthroscopy was calculated by stratifying individuals based on their responses to the relevant NAHS items. Patients were classified as symptomatic preoperatively if they reported a score of ≤3 for any of the mechanical symptom questions, and patients were classified as asymptomatic if all responses were scored as a 4. Symptom resolution was defined as a change from a preoperative symptomatic score (<4) to an asymptomatic score (4) postoperatively. If there was no change in score from preoperative to postoperative reporting (eg, a patient reported 2 for stiffness both preoperatively and postoperatively) then that symptom was classified as persistent. Any change from a lower score to a higher score of <4 (eg, 0 to 2) was interpreted as partial improvement, but not complete resolution of the symptom. Additionally, new onset symptoms were calculated as any change from a preoperative asymptomatic score (4) to a postoperative symptomatic score (<4).
To identify predictors of symptom resolution, univariate analyses were performed using independent-samples t tests or Mann-Whitney U tests for continuous variables and chi-square or Fisher exact tests for categorical variables, as appropriate. Variables demonstrating significant associations in univariate analysis were further evaluated using multivariate logistic regression to determine independent predictors of symptom resolution.
Finally, of patients who indicated preoperative symptoms, 2 cohorts were created based on whether they reported symptom resolution or persistence for each individual mechanical symptom. Independent-samples t tests were conducted to assess for significant differences in functional outcome scores across all subscales of the NAHS (Pain, Symptoms, Physical Function, and Sports Activities). The NAHS was selected for its specificity to mechanics, morphology, and overall function rather than secondary factors to mechanics that other common hip patient-reported outcome measures may evaluate, such as emotional well-being or overall lifestyle.
Results
Out of 376 patients enrolled, 228 were included in the final analysis. Seven were excluded for Tönnis grade >2, and 141 were excluded due to incomplete survey data at baseline or 2-year follow-up (Figure 1). The mean age of the included patients was 36.1 years (range 18-64 years), 51.3% were female, and the mean BMI was 25.4 kg/m2 (Tables 1 and 2).
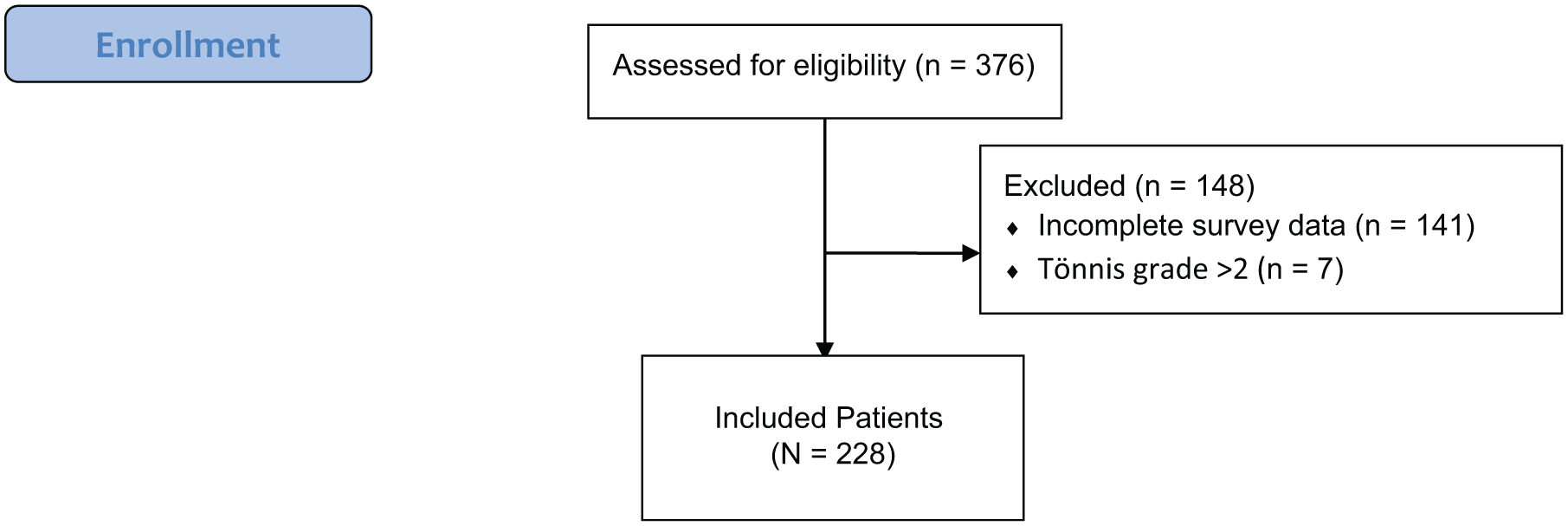
Flowchart of included patients.
Patient Characteristics (N = 228) a

Data are presented as n (%) or mean (95% CI). BMI, body mass index; FAI, femoroacetabular impingement.
Intraoperative Findings and Procedures (N = 228) a
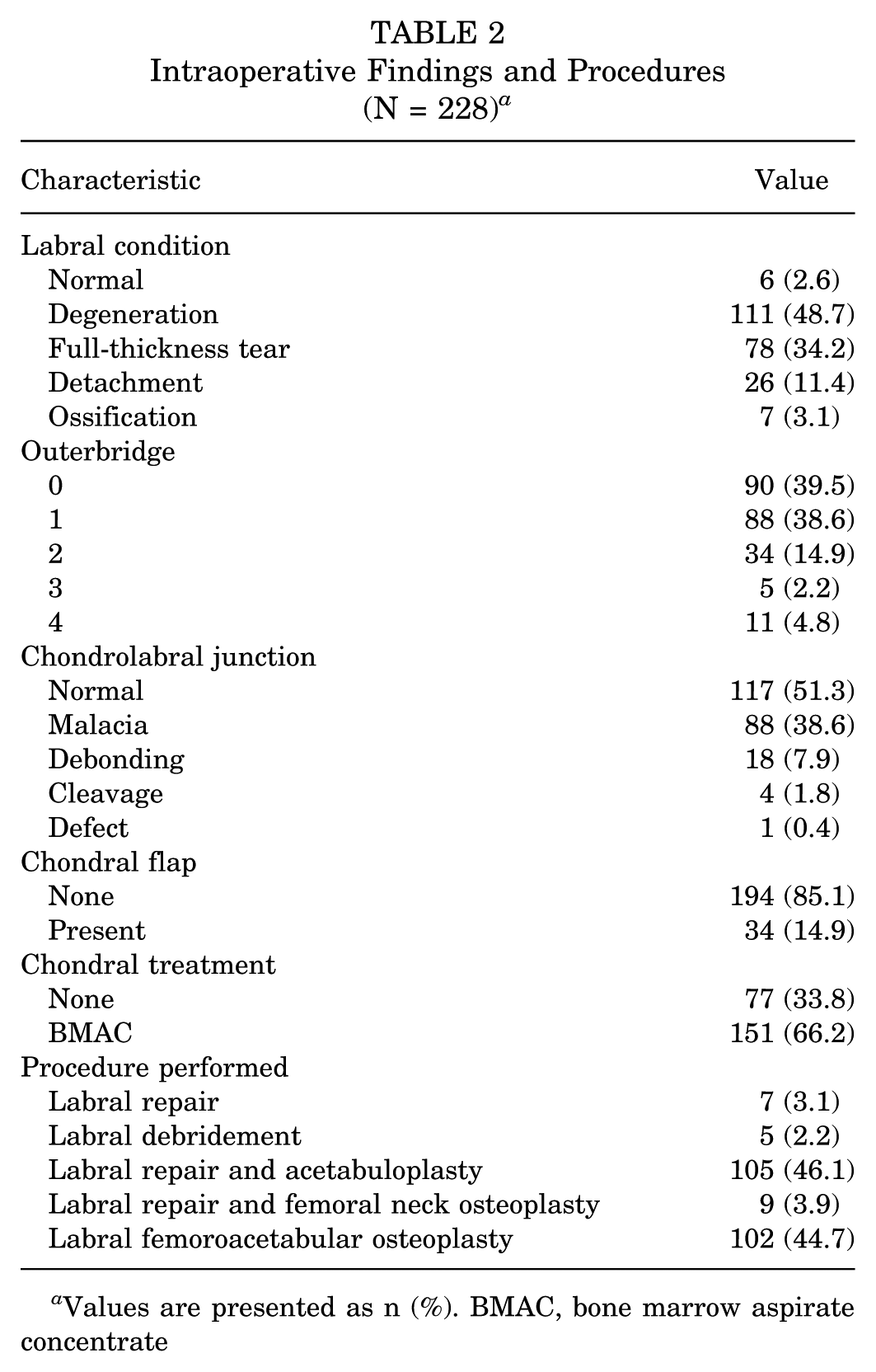
Values are presented as n (%). BMAC, bone marrow aspirate concentrate
Symptom Prevalence, Resolution, and Persistence
Among the 228 patients included in the analysis, the most commonly reported preoperative mechanical symptom was stiffness (85.5%), followed by catching/locking (65.8%) and giving out (36.4%) (Table 3). Of the original cohort of 228 at enrollment, 18 patients (7.9%) reported no mechanical symptoms, 61 (26.8%) reported only 1, 80 (35.1%) reported 2 overlapping symptoms, and 69 (30.3%) reported all 3. Of the patients who initially reported symptoms, resolution by 24 months postoperatively was individually observed in 80.7% of patients with giving out, 59.3% of those with catching/locking, and 29.7% of those with stiffness. Of patients whose symptoms persisted but did not fully resolve, 56.2% reported some improvement in catching or locking, 54.1% of patients reported improvement in giving out, and 59.9% of patients reported improvement in stiffness. For patients who were asymptomatic at baseline, very few patients developed symptoms of catching/locking or giving way (14.1% and 4.1%, respectively); however, 45.5% of patients who reported no stiffness at baseline reported some at 24 months.
Prevalence and Resolution of Mechanical Symptoms at 24 Months a

Data for symptoms at baseline are presented as n (%) of the total cohort.
Data for symptoms resolved, improved, and persistent are presented as n (%) of patients who had the symptom at baseline.
Data for symptoms with new onset are presented as n (%) of the asymptomatic population for the respective symptom.
Distribution at baseline and 24 months is based on the total sample.
Predictors of Symptom Persistence
Of patients who had mechanical symptoms at baseline, most baseline variables resulted in no significant association with symptom resolution on a univariate analysis (Tables 4 and 5). However, for patients with giving out symptoms, several baseline characteristics were significantly associated with persistence at 24 months. These included higher Tönnis angle, higher BMI, and lower CEA. Additionally, acetabular cartilage thinning was significantly associated with persistent stiffness symptoms (P = .019), though no such association was found for the other 2 symptom domains. No significant associations were observed between symptom resolution and sex, age, or Tönnis grade across symptom types (all P > .05) (Table 4).
Univariate Analysis of Continuous Symptom Persistence/Resolution Predictors a
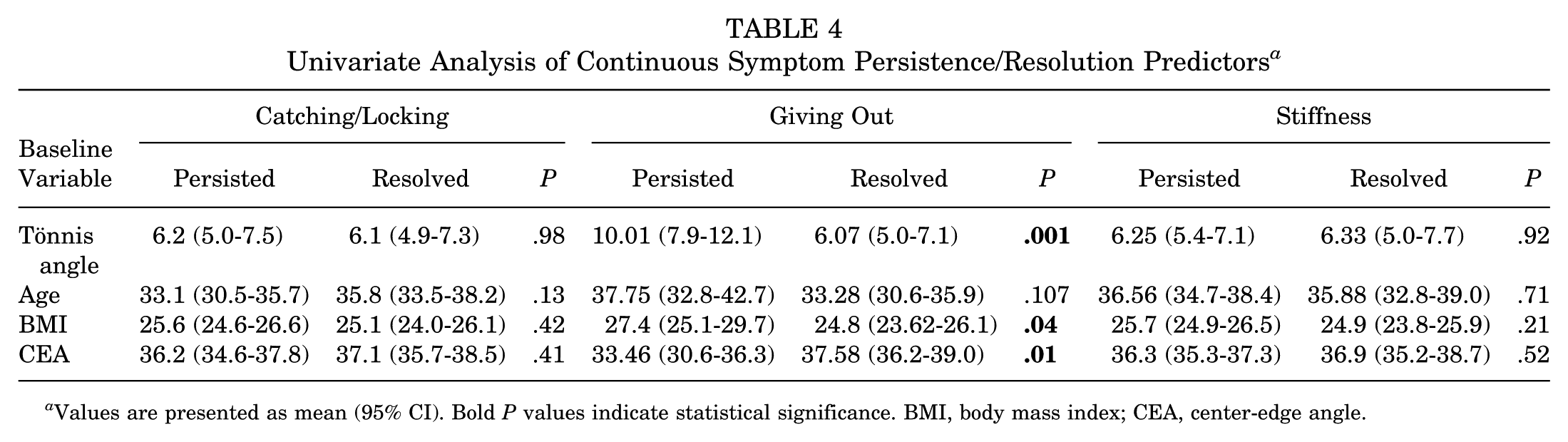
Values are presented as mean (95% CI). Bold P values indicate statistical significance. BMI, body mass index; CEA, center-edge angle.
Univariate Analysis of Categorical Symptom Persistence/Resolution Predictors a
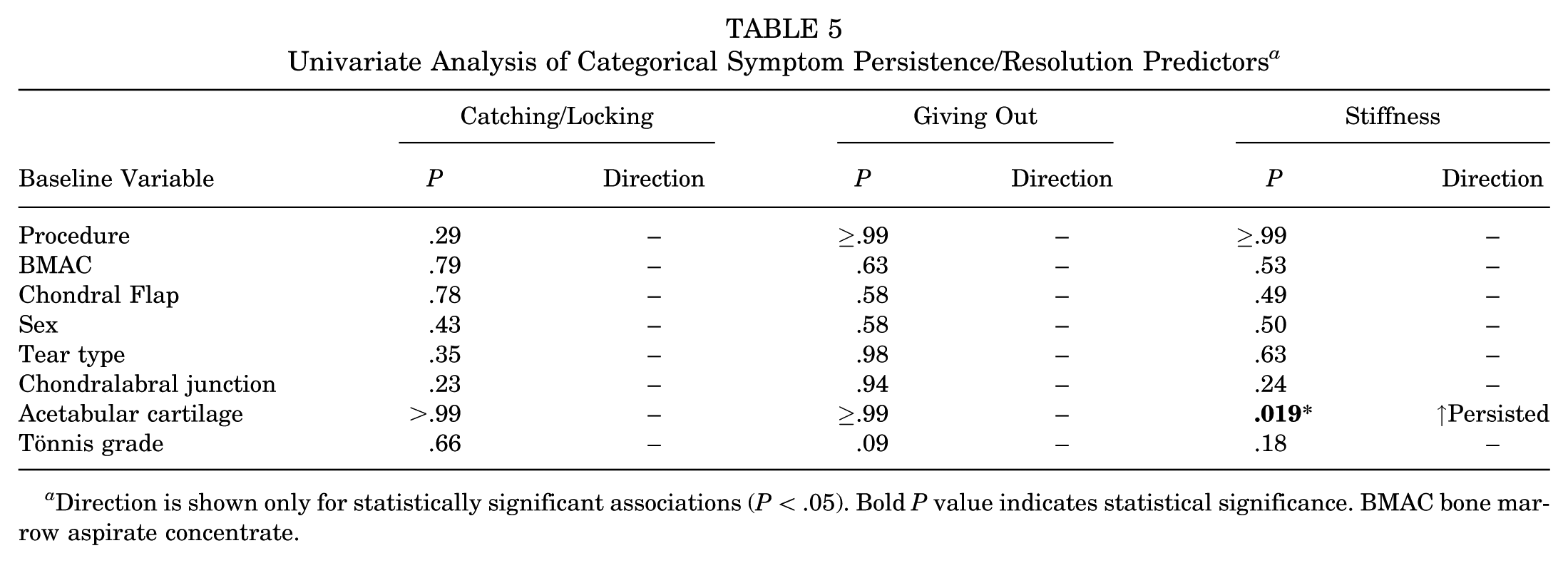
Direction is shown only for statistically significant associations (P < .05). Bold P value indicates statistical significance. BMAC bone marrow aspirate concentrate.
On multivariable logistic regression for significant univariate predictors of giving out symptom resolution at 24 months, lower Tönnis angle (odds ratio [OR], 0.79; 95% CI, 0.66-0.92; P = .01) and higher lateral CEA (OR, 1.19; 95% CI, 1.05-1.39; P = .014) were independently associated with symptom resolution. BMI (P = .11) and acetabular cartilage thinning (P = .67) were not significantly associated with resolution.
NAHS Subscores
For all NAHS subscores and total scores, patients whose symptoms resolved reported significantly higher scores at 24 months compared to those with persistent symptoms (all P < .05). Patients with resolved symptoms also demonstrated significantly greater improvements from baseline for the majority of NAHS scores (all P < .05) (Table 6).
NAHS Scores at 24 Months and Change From Baseline by Symptom Resolution Status a

Data are presented as mean (95% CI). Bold P values indicate statistical significance of P < .05.
Scores at 24 months.
Change from baseline to 24 months.
Discussion
The findings of this study indicate that the majority of patients experience mechanical symptoms before hip arthroscopy, with stiffness being the most common and persistent symptom. Giving out and catching/locking resolved for the majority of patients while stiffness only resolved in about 30% of patients. On multivariable analysis, lower CEA and higher Tönnis angle were significant predictors of symptom persistence. Patients with resolved symptoms had significantly higher NAHS scores at 24 months, indicating meaningful functional improvement. This quantification of symptom prevalence, persistence, and its predictors may help clinicians better understand clinical presentation and outcomes that directly affect patients’ quality of life.
Historically, mechanical symptoms such as catching, locking, and stiffness were among the earliest indications for hip arthroscopy.25,3 Early studies reported improvement in these symptoms, although severity and population prevalence was not routinely quantified. 5 The high prevalence and persistence of stiffness in this population likely reflect the complex healing process of the joint, which involves lingering inflammation and tissue remodeling. Other sources of persistent stiffness may be due to potential scarring of the capsule or capsular contracture from decreased preoperative range of motion due to bony impingement. Studies have also demonstrated that for up to 12 months after hip arthroscopy, as many as 64% of patients can still have some amount of joint effusion, which is a predictor of inferior 2-year outcomes. 19 This ongoing low-grade postoperative inflammation may contribute to joint pain, capsular adhesions, and a sustained sensation of stiffness.2,17 While symptoms such as catching or giving out are more directly linked to structural pathology correctable with surgical repair, stiffness may reflect a more widespread intra-articular and periarticular response. 15 Furthermore, heterotopic ossification is a common potential postoperative complication following hip arthroscopy that has the potential to lead to decreased range of motion; however, it is largely asymptomatic and was not assessed in our study. 21
Furthermore, even within a structured and functionally informed rehabilitation protocol, some patients may experience persistent stiffness due to pain, fear of reinjury, or inconsistent adherence to prescribed exercises. 33 Our postoperative approach specifically aims to increase range of motion, reduce early joint inflammation and protect the soft tissue repair during the critical early healing phase. 24 However, a subset may still adopt overly cautious movement patterns in an effort to protect the repair site, commonly known as kinesiophobia, which can contribute to prolonged stiffness and delayed return of function.10,22 This may also be reflected in the higher rates of new onset stiffness in preoperatively asymptomatic patients when compared with cases of new onset catching/locking or giving out. It is important to recognize that stiffness that persisted in the majority of patients was reported as mild (51.3%), which may be equitable to everyday sensations of low-grade stiffness commonly experienced by the general population. In some cases, reported stiffness may sometimes reflect nonpathological or expected postoperative sensations rather than true, clinically significant symptom persistence. In order to alleviate perceived stiffness, several measures can be undertaken. These may include individualized progression of range-of-motion and strengthening exercises aimed at reducing stiffness on a longitudinal basis, with an emphasis of continuing movement after the postoperative protocol formally concludes. For example, our standard postoperative protocol ends at 6 months, while follow-up in this study extended to 24 months, leaving ample opportunity for stiffness to develop if patients were sedentary. 24 Additionally, patient education and personalized pain management throughout the postoperative period can help reduce fear-avoidant behaviors, in order to support more confident use of the hip and facilitate functional recovery.
The high resolution rates observed for mechanical symptoms such as catching/locking and giving out suggest that hip arthroscopy is particularly effective in treating patients with clear mechanical symptoms attributable to FAI. In patients with FAI morphology, arthroscopic correction through femoral and/or acetabular osteoplasty reduces the osseous conflict responsible for these dynamic symptoms.18,35 This procedure returns the spherical shape of the femoral head and restores the head-neck offset, allowing for improved intra-articular contact and reduced friction, restoring the joint to a more anatomic state. 16 Successful reshaping of joint morphology may therefore be essential to alleviating mechanical symptoms in hip arthroscopy patients.
Higher CEA and lower Tönnis angle were identified as independent predictors of mechanical symptom resolution, specifically the symptom of the hip "giving out." In the broader literature, a lower CEA has been associated with inferior functional outcomes and earlier conversion to total hip arthroplasty, as it reflects insufficient acetabular coverage of the femoral head, contributing to joint instability and abnormal load distribution.8,31 Similarly, patients with persistent postoperative giving out symptoms had, on average, higher Tönnis angles, while those whose symptoms resolved tended to fall within the normal range. The normal Tönnis angle range is approximately 0° to 10°, with angles >10° suggesting acetabular dysplasia or undercoverage, and angles <0° indicating acetabular overcoverage or pincer-type impingement. 36 A steeper acetabulum, as indicated by a higher Tönnis angle, offers less lateral containment of the femoral head and may contribute to functional instability during weightbearing or dynamic movement. 37 Even after appropriate bony reshaping through osteoplasty, if acetabular inclination remains excessive, the joint may continue to lack sufficient structural support, leading to a persistent sense of instability or giving out, and has been identified as a risk factor for reoperation.20,23,38
Finally, resolution of mechanical symptoms was associated with higher NAHS scores at 2 years postoperatively. Symptom resolution was associated with significantly higher final NAHS scores and greater improvement from baseline, particularly in the Sports Activities and Symptoms subscales, providing granular support for the alleviation of mechanical symptoms. 35 Of note, the NAHS Symptoms subscale includes the mechanical symptom questions used to define symptom presence, which may bias scores higher in patients without preoperative symptoms. In contrast, the Pain, Physical Function, and Sports Activities subscales do not include these items and thus offer a less biased assessment of function related to mechanical symptoms. Furthermore, even patients with persistent symptoms reported substantial improvements in NAHS scores from baseline, suggesting that arthroscopy offers broader therapeutic benefits beyond the elimination of mechanical symptoms. The strong relationship between symptom resolution and better functional outcomes underscores the clinical relevance of addressing mechanical pathology through hip arthroscopy, while the improvements seen in patients with persistent symptoms highlight the multifactorial value of surgical intervention.
Limitations
The present study should be interpreted in the context of several limitations. First, the results may have limited generalizability due to the study being conducted at a single institution by a highly experienced surgeon, which may not reflect the broader variability in hip arthroscopy techniques and surgical expertise. Additionally, all patients completed a fully self-guided postoperative protocol without the use of formal physical therapy. While this protocol was specifically directed at increasing range of motion, patients undergoing different protocols may experience different outcomes. Furthermore, as range of motion data were not reported, we were unable to objectively assess stiffness using a standardized protocol. Another limitation of this study is the potential for selection bias, as a proportion of eligible patients were excluded due to incomplete baseline or 2-year follow-up survey data, which may limit the generalizability of the results. A further limitation of this study is the absence of follow-up imaging, such as magnetic resonance imaging or radiographs, at 2 years postoperatively. Without these data, we were unable to objectively assess bony resection, postoperative heterotropic ossification, loose bodies, labral calcification, or cartilage degeneration that may contribute to the persistence of mechanical symptoms. Future studies incorporating various postoperative protocols and routine follow-up imaging could provide valuable insights into the structural mechanisms underlying symptom persistence after hip arthroscopy.
Conclusion
Hip arthroscopy efficiently resolved mechanical symptoms such as catching/locking or giving out while significantly improving functional outcomes. However, persistent stiffness was a common postoperative issue. Patients should be informed preoperatively that residual stiffness may improve with surgery but not be completely alleviated.
Footnotes
Acknowledgements
The authors thank the Conine Family Fund for Joint Preservation for providing funding for this study.
Final revision submitted January 16, 2026; accepted January 22, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Approval for this study was obtained from Massachusetts General Hospital (IRB# 2013P001442 & 2019P002191).