
Abstract
Background:
Patients with hip and lumbosacral spinal pathologies may experience exacerbated symptoms as a result of these concomitant conditions. There is a paucity of midterm follow-up on patients who undergo primary hip arthroscopy before spinal surgery.
Purpose:
To assess patient-reported outcome measures (PROMs) among patients with hip arthroscopy and concomitant symptomatic lumbosacral pathology at 5-year follow-up and to compare revision rates and conversion to total hip arthroplasty between patients in a hip-spine (HS) cohort and patients in a matched control (MC) cohort without lumbosacral pathology.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective review analyzed prospective data of patients who underwent primary hip arthroscopy for treatment of symptomatic labral tears. The study included patients aged ≥18 years with PROMs at baseline and minimum 60-month follow-up. Patients with HS syndrome were propensity matched to a MC group without any lumbosacral pathologies. Patients in the HS cohort indicated (1) lower back pain/symptoms on preoperative surveys, (2) a pathologic lumbosacral spine diagnosis confirmed by a radiologist, and (3) clinical documentation. PROMs, clinically meaningful outcomes, improvement over time, revision rates, and conversion to total hip arthroplasty were compared.
Results:
A total of 76 patients were included, with 38 patients each in the HS and MC cohorts. The HS cohort had significantly worse functional outcomes at baseline and 12-, 24-, and 60-month follow-up. However, the HS cohort demonstrated no significant difference in achieving the minimal clinically important difference, Patient Acceptable Symptom State, and substantial clinical benefit but showed a mix of no significant difference or significantly greater mean magnitudes of improvement across various PROMs over time. There were no significant differences in rates of revision or conversion to total hip arthroplasty.
Conclusion:
Although hip arthroscopy patients with concomitant lumbosacral spinal pathology report lower functional outcomes at 5 years than MCs, they can expect similar, if not higher, magnitudes of improvement, as well as similar rates of achieving clinically meaningful outcomes and no increased risk of secondary surgery. These findings substantiate that HS pathology is not an absolute contraindication for hip arthroscopy.
For patients with symptomatic labral tears and femoroacetabular impingement (FAI), hip arthroscopy has been shown to improve patient outcomes with low rates of complications and revisions. 24 However, hip arthroscopy patients with concomitant spinal pathology may experience increased stresses through the hip joint or use compensatory behaviors, exacerbating FAI symptoms.14,19 This phenomenon was first defined by Offierski and MacNab as “hip-spine syndrome” in patients with concurrent hip osteoarthritis and lumbar spine degenerative disease. 28 As low back pain was estimated to affect 619 million people globally in 2020, there is a growing need to understand how concomitant spinal problems affect hip arthroscopy outcomes. 11
There are 3 classifications of hip-spine (HS) syndrome as originally defined: simple, in which the hip or spine is identified as the primary source of pain; complex, in which the pain source is unclear; and secondary, where pain is attributable to hip and spine pathologies. 28 Since HS syndrome was first described, more attention has been brought to secondary HS syndrome, where coexisting pathology in either the hip or spine exacerbates symptoms in the other, for any patient population, regardless of the presence of osteoarthritis.28,36 A unifying feature across these conditions is abnormal spinal mobility, which alters spinopelvic mechanics and limits the body's ability to accommodate motion demands.
In these patients, variations in sagittal and coronal spinal alignment can lead to compensatory changes in pelvic tilt and reduced overall range of motion. 6 Consequently, lumbar spine pathology may exacerbate FAI symptoms or induce symptoms when FAI may have otherwise been asymptomatic. These compensations modify functional acetabular orientation during movement, altering hip joint mechanics and increasing abnormal contact stresses. 10 This can include contributing to anterior instability, hyperextension, and hip impingement. Rather than a single mechanism, HS syndrome encompasses a spectrum of spinal pathologies that restrict mobility and force compensatory motion through the hip joint, potentially contributing to pain and accelerated wear patterns. 16
Even in the absence of FAI, lumbar spine dysfunction can cause muscular imbalances, leading to further instability and weakness in the hip. 8 Excessive lordosis can lead to anterior pelvic tilt while limited lordosis can lead to posterior pelvic tilt. 18 Scoliosis can also cause a limited range of motion. 21 Reciprocally, the limited range of motion caused by the pathologic hip joint has been historically associated with low back pain.23,26 Hip pathologies have been found to distribute pain in a similar manner to lumbar spine pathologies, with referrals to the buttocks, posterior thigh, and pain below the knee.15,17 Therefore, in patients who have hip and lumbar spine issues, it can be difficult to determine the primary source of the pain.
Outcomes for patients undergoing hip arthroscopy in the setting of secondary HS syndrome have been well studied at 2-year follow-up. 10 Patients with HS syndrome often report worse measures at baseline and inferior outcome measures in comparison with a matched control (MC) but still achieve significant improvement in comparison with baseline scores.1,35 However, a paucity of data exists examining longer-term outcomes for patients undergoing hip arthroscopy in the setting of HS syndrome. Therefore, the purpose of this study was to assess patient-reported outcome measures (PROMs) for hip arthroscopy patients with concomitant symptomatic lumbosacral pathology at 5-year follow-up and to compare revision rates and conversion to total hip arthroplasty (THA) between patients in a HS cohort and patients in a MC cohort without lumbosacral pathology.
Methods
Study Design
This was a retrospective review of prospectively collected data of patients undergoing hip arthroscopy by a single fellowship-trained surgeon (S.D.M.) from May 2014 to May 2019. This study was approved by the institutional review board (2013P001442 and 2019P002192). Inclusion criteria were as follows: patients aged ≥18 years who were undergoing primary hip arthroscopy and had completed baseline and 5-year follow-up PROM surveys. Patients were excluded if they had previous spinal surgery or intervention (eg, decompression laminectomy/discectomy, kyphoplasty, fusion), any previous surgical procedure involving the ipsilateral hip or leg, radiographic evidence of hip dysplasia (lateral center-edge angle <20°), advanced hip osteoarthritis (Tönnis grade >1), and/or previous hip conditions (fracture, inflammatory arthropathies, Legg-Calve-Perthes disease, slipped capital femoral epiphysis, avascular necrosis).
All patients underwent a standardized assessment when evaluated in an outpatient clinic for hip pain with provocation testing of the labrum. This included physical examinations in which patients were assessed for impingement-related symptoms (eg, pain and/or limited range of motion with flexion, adduction, and internal rotation or flexion, abduction, and external rotation). 13 Patients received hip/spine radiographs (ie, anteroposterior pelvic and Dunn lateral views). Patients with positive clinical and radiographic findings underwent magnetic resonance arthrography of the hip to evaluate for labral pathologies. Patients received a corticosteroid injection at the time of magnetic resonance arthrography with a minimum 3 months of physical therapy. Patients with persistent or recurrent symptoms were offered hip arthroscopy for definitive management, and the decision to proceed was made after a shared conversation between the patient and the surgeon (S.D.M.). All patients who consented for surgery with the senior author (S.D.M.) were approached for enrollment in this study.
Prospective survey data and a review of electronic medical records were used to identify patients with a history of lumbosacral pathology before indication for hip arthroscopy. Patients in this study were then stratified into either the HS cohort or the MC cohort. To be placed in the HS cohort, patients required (1) confirmation of lower back pain/symptoms on preoperative survey questionnaires, (2) a pathologic lumbosacral spine diagnosis confirmed by the radiologist with preoperative imaging (plain lumbar spine radiographs, lumbar spine magnetic resonance imaging, or both), and (3) clinical documentation of lumbosacral pathology by the physician who either ordered imaging or initially evaluated the patient for lower back symptoms. Lower back pain was not captured through hip-specific PROMs but was instead assessed at enrollment by a Self-administered Comorbidity Questionnaire that included a yes/no item asking patients whether they had lower back pain. The presence of back pain alone on the questionnaire was not used to define HS syndrome without corresponding imaging and clinical documentation. Patients who were placed in the MC cohort reported (1) absence of lower back pain/symptoms on preoperative surveys and (2) no clinical diagnosis verifying the presence of lumbosacral pathology.
Patients in the HS and MC cohorts were matched via propensity score matching (PSM). PSM was used to efficiently match covariates with a single score, thus retaining more participants than if exact matching were to be employed by producing matches on a continuous scale. 4 Patients were matched by the following factors: age, sex, body mass index, Tönnis grade, and alpha angle. Matching was performed on demographics similar to a previously published 2-year cohort, with the addition of Tönnis grade and alpha angle to further account for baseline differences. 35 Additional variables were not included, as this would have substantially reduced the MC size.
Data Collection
Descriptive data were collected, including age, sex, laterality, and body mass index. Intraoperative findings were recorded, such as cartilage degeneration as graded by the Outerbridge classification, 29 labral treatment, and FAI treatment. Radiographic findings were also included, such as osseous pathology (cam and/or pincer lesions), cartilage thinning, Tönnis grade and angle, lateral center-edge angle, and labral tear type (intact, frayed, linear, complex, or degenerative). Patients were sent the following PROM surveys preoperatively and postoperatively at 3, 6, 12, 24, and 60 months: the modified Harris Hip Score, Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports-Specific Subscale (HOS-SSS), and the International Hip Outcome Tool–33 (iHOT-33). PROMs were assessed for the percentage of patients who achieved previously established thresholds for the minimal clinically important difference (MCID), Patient Acceptable Symptom State (PASS), and substantial clinical benefit (SCB) for those undergoing hip arthroscopy.27,33 Rates of revision hip arthroscopy, secondary hip surgery, any instances of spinal surgery, and conversion to THA were collected via postoperative surveys and confirmed by the electronic medical records.
Abbreviated Surgical Technique
All patients in this study underwent hip arthroscopy via the puncture capsulotomy technique.9,12,30 General anesthesia was administered and the patient was placed supine on a hip traction table. The nonoperative leg was abducted with a silicone-padded perineal post, and the operative leg was slightly adducted against the post. To decrease risk of nerve injury, the anterolateral portal was created by intra-articular distention under fluoroscopic guidance. 2 Next, the midanterior and anterior portals were created, followed by the Dienst portal. In certain cases, an additional portal was made to enhance visualization of anteromedial or lateral cam lesions distal or proximal to the anterolateral portal for enhanced visualization. The hip was assessed for chondrolabral junction breakdown and damage to the labrum.
Labral repair was performed if adequate tissue remained for suture fixation. The peripheral compartment of the hip was assessed for labral condition, degree of tearing, and/or degeneration. For labrums that were hypoplastic (width <5 mm), had complex tearing, were <10 mm, or had frank degeneration of native tissue, a labral reconstruction with capsular augmentation was performed. 34 For cases of labral reconstruction, only a capsular autograft was used, with no patients undergoing remote autografts or allografts. During the study period, the senior surgeon began using a standardized method of bone marrow aspirate concentrate for chondrolabral junction breakdown, full-thickness chondral flaps, or Outerbridge grade ≥2 lesions, 20 switching away from the previous use of microfracture. Procedures were determined by reviewing operative notes. Cam deformities were resected via femoroplasty, and acetabuloplasty was performed for pincer deformities. Pincer lesions were defined as a lateral center-edge angle >39°, and cam lesions were defined as an alpha angle >55°.
Postoperative Rehabilitation
All patients underwent a standardized 5-step, 6-month postoperative rehabilitation protocol.12,25 Patients could immediately bear weight as tolerated using a flat-foot gait with crutches. Patients were not required to undergo any formal therapy or wear a brace in the postoperative period. They were also instructed to avoid pivoting, hip flexion >90°, and pelvic tilting. At 6 weeks, patients could begin cycling on a stationary bike with minimal resistance. At 10 weeks, patients could begin swimming or using the elliptical machine to simulate light resistance. At 4 months, light-weight high-repetition strengthening exercises, including short-arc leg presses and hamstring curls, could be resumed. Finally, patients were instructed to resume full-impact loading activities as tolerated beginning at 6 months.
Post Hoc Power Analysis and Statistical Analysis
A post hoc power analysis was performed by using this study's 5-year iHOT-33, which had a standard deviation of 21.6, and the previously established MCID threshold for iHOT-33 at 5 years, 15.1. 27 To be powered at 80% with these thresholds, 34 patients were needed for the HS cohort and the MC cohort.
Once PSM was performed, continuous variables were compared by 2-tailed independent t tests. Improvement over time was assessed by a linear mixed effects model, with time defined as a continuous variable at 60-month follow-up to account for weighted mean differences in improvement at discrete time points. The model estimates the weighted mean difference in improvement from baseline between cohorts to 60 months. Positive and negative values indicate greater and lesser improvement, respectively, in the HS cohort as compared with the MC cohort. Categorical variables were analyzed with a chi-square or Fisher exact test. For continuous variables, parameters were presented with 95% confidence intervals. P < .05 was considered statistically significant. All analyses were performed in RStudio (Version 2024.12.1 +563).
Results
Patient Characteristics
Of the 195 patients initially enrolled, 28 were excluded owing to Tönnis grade >1 (n = 27) or prior spinal surgery (n = 1), leaving 167 eligible patients. Of these, 86 patients (52%) completed 5-year postoperative PROMs. Among patients with available PROMs, 38 patients in the HS group underwent PSM to 48 patients in the non-HS group, resulting in 38 matched pairs in the final analysis (Figure 1). The mean length of follow-up was 61.0 months (range, 60-78) for all patients. No significant differences were found in baseline descriptive, radiographic, or intraoperative variables between the HS and MC cohorts (Tables 1 and 2). For the HS cohort, radiologist impressions of lumbosacral imaging as well as clinical documentation allowed for classification of lumbosacral pathologies, with lumbar degenerative disc disease as the most common comorbidity (42.2%). Distributions of types of procedures, chondral injury treatment, and labral management were also similar between cohorts (Table 2).
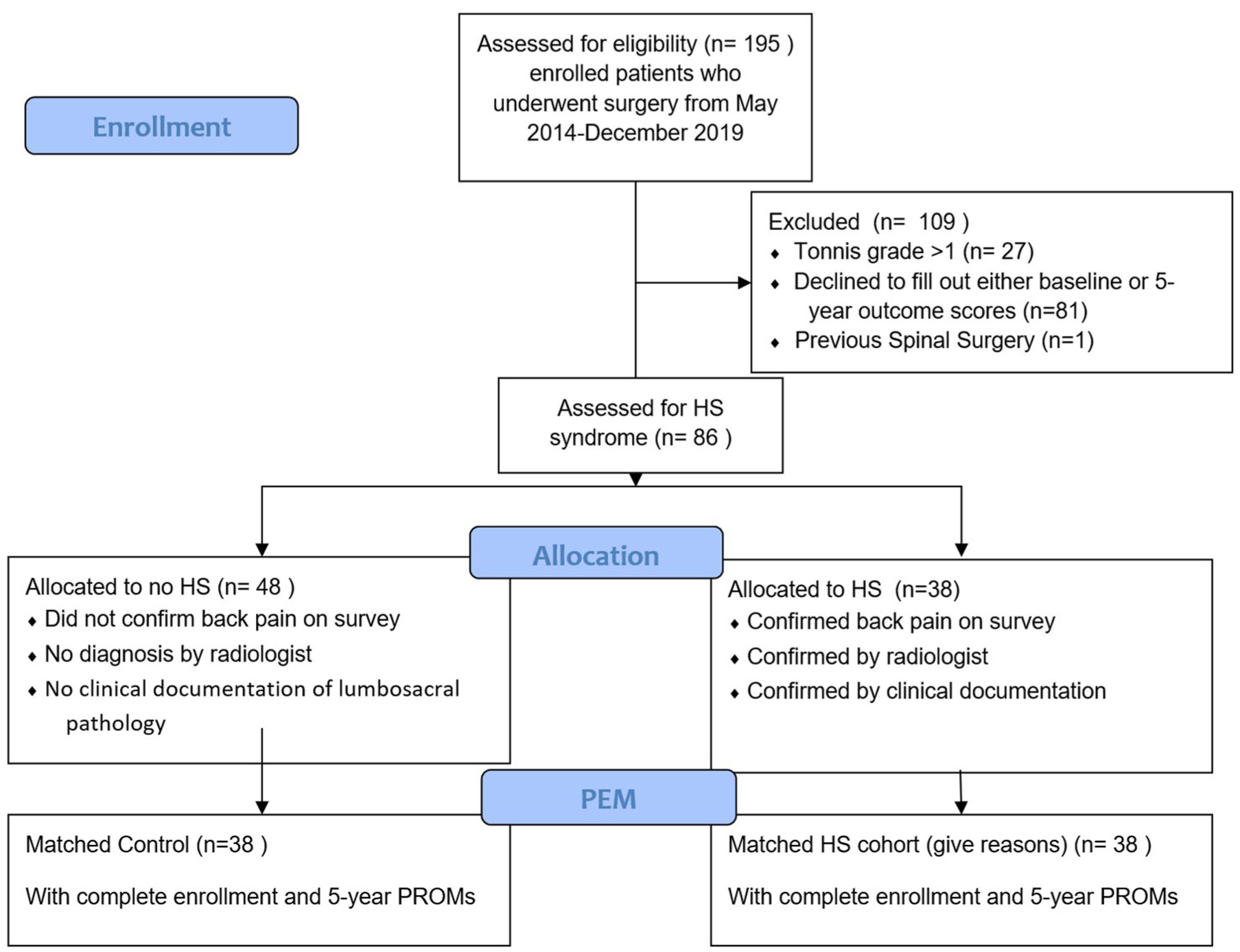
Flowchart detailing selection criteria. HS, hip-spine; PROM, patient-reported outcome measure.
Patient Characteristics by Cohort a
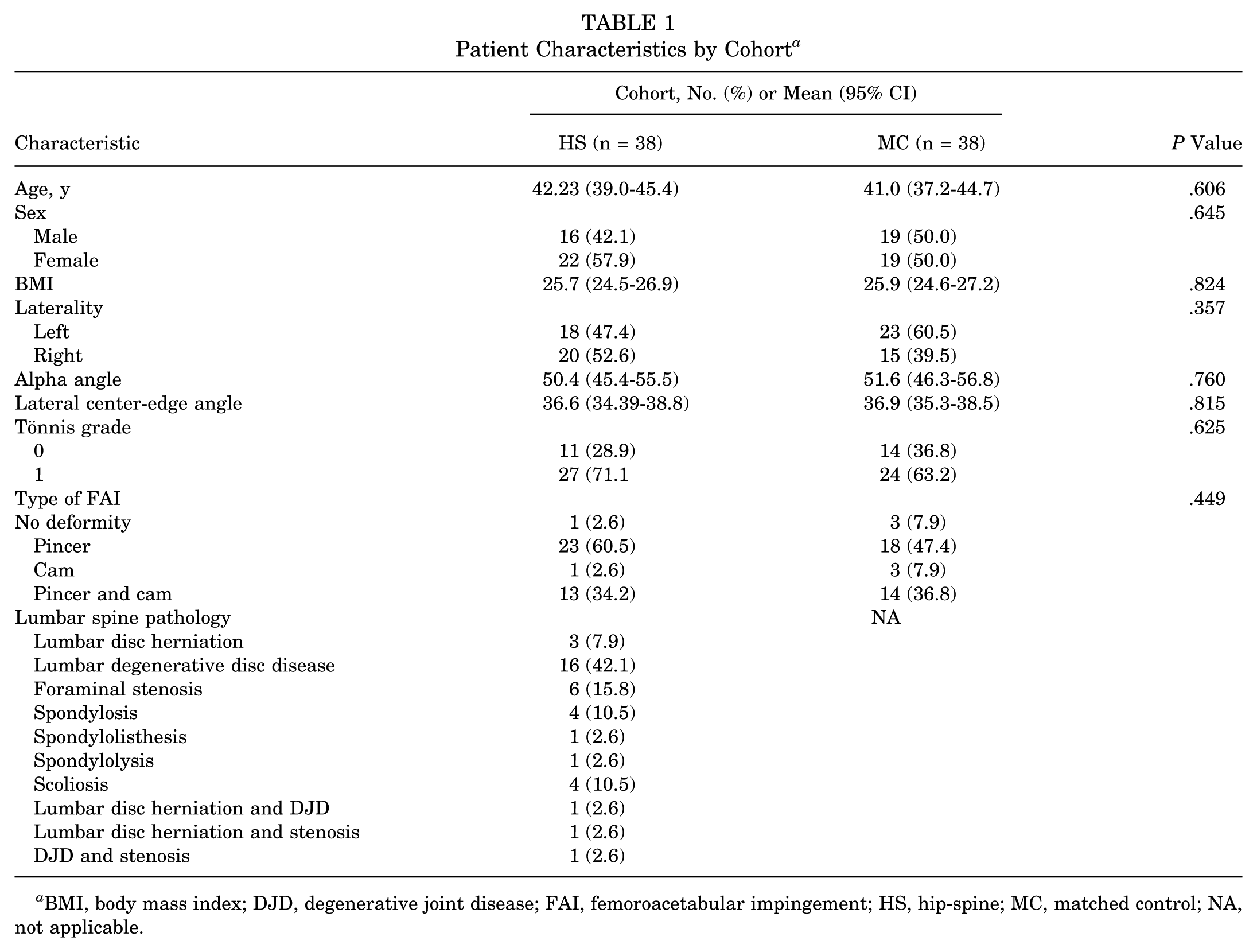
BMI, body mass index; DJD, degenerative joint disease; FAI, femoroacetabular impingement; HS, hip-spine; MC, matched control; NA, not applicable.
Intraoperative Findings and Procedures a

BMAC, bone marrow aspirate concentrate; HS, hip-spine; MC, matched control.
Patient-Reported Outcome Measures
Patients in the HS cohort reported significantly worse functional outcomes for the majority of PROMs at baseline and through the 1-, 2-, and 5-year follow-up time points (Table 3). Exceptions include HOS-SSS at baseline; HOS-ADL, iHOT-33, and HOS-SSS at 3 months postoperatively; HOS-ADL at 6 months; and HOS-SSS at 60 months.
Patient-Reported Outcome Measures a
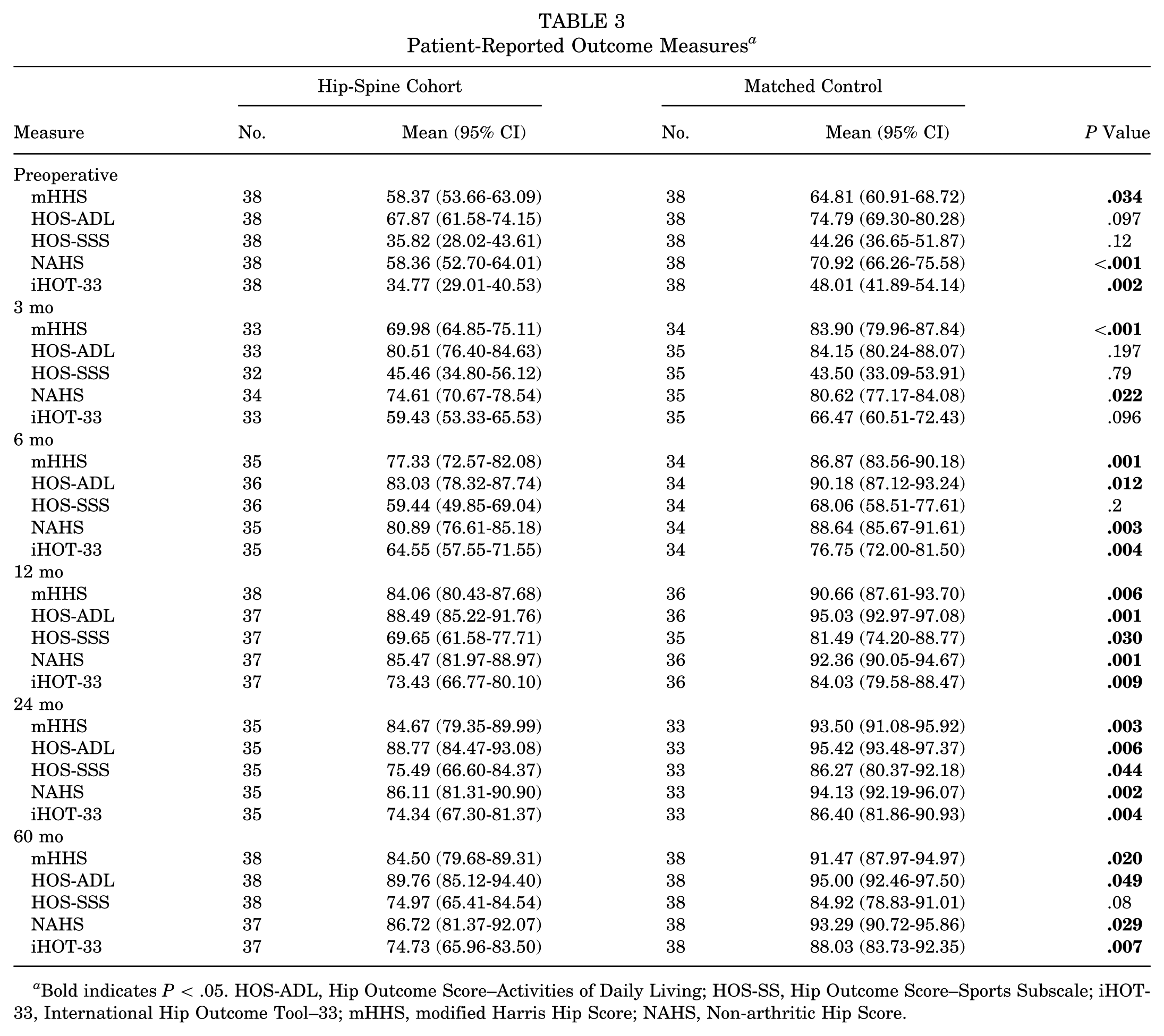
Bold indicates P < .05. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; iHOT-33, International Hip Outcome Tool–33; mHHS, modified Harris Hip Score; NAHS, Non-arthritic Hip Score.
Magnitude of Improvement and Clinically Meaningful Outcome Achievement
When time was incorporated into a linear mixed effects model as a continuous variable, the mean magnitude of improvement was either similar or significantly greater at 5 years for all PROMs for the HS cohort as compared with the MC cohort (Table 4). There were no significant differences in achieving the MCID, PASS, and SCB for any PROM at 5-year follow-up, except that the MC cohort had significantly higher rates of PASS than the HS cohort for the modified Harris Hip Score and iHOT-33 at 5 years.
Improvement in Patient-Reported Outcome Measures a

Bold indicates P < .05. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; HS, hip-spine; iHOT-33, International Hip Outcome Tool–33; MC, matched control; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-arthritic Hip Score; PASS, Patient Acceptable Symptom State; SCB, substantial clinical benefit.
Values represent the weighted mean difference in improvement from baseline between the HS and MC cohorts, derived from a linear mixed effects model. Positive values indicate greater improvement in the HS cohort; negative values indicate less improvement.
Revision Surgery and Conversion to THA
There was no difference in rates of revision surgery between cohorts (P≥ .99) as the HS and MC cohorts reported no revisions (0%). Additionally, no significant difference was found in the rates of conversion to THA (P≥ .99), as 1 patient had THA on the ipsilateral side in the MC cohort and 2 patients had THA in the HS cohort within 5 years after hip arthroscopy. For the MC cohort, THA was performed 51 months after hip arthroscopy, while the times to THA in the HS cohort were 47 and 48 months. Five patients in the HS cohort had spine surgery at a mean time of 36.6 months (95% CI, 12.95-60.25) after hip arthroscopy, 2 with lumbar laminectomy and 3 with lumbar decompression and fusion. No patients in the MC cohort reported spinal surgery within the study period.
Discussion
At 5-year follow-up, patients in the HS cohort had lower PROM scores than a MC cohort but statistically similar and sometimes higher magnitudes of improvement. Additionally, the cohorts had similar rates of achieving clinically meaningful outcomes as well as similar rates of secondary surgery. This study adds longer-term follow-up data to a growing body of literature demonstrating that HS cases tend to have lower functional outcomes overall yet similar rates of improvement and no increased need for secondary surgery.3,35 Thus, hip arthroscopy has the potential to significantly improve hip-related symptoms for patients with overlapping hip and spine pathology. The results of this study can help inform the preoperative decision-making process for patients with labral tears and concomitant lumbosacral pathology.
The first key finding of this study was that patients in the HS cohort had lower PROM scores than the MC cohort at 12-, 24-, and 60-month follow-up. This result is not unexpected, as it is consistent with literature that patients with lumbosacral pathology start with lower preoperative functional outcome measures. 31 Moreover, it has historically been found that HS cases have worse functional outcomes with prospective follow-up.5,35 The current study illustrates that patients with hip arthroscopy and concomitant lumbosacral pathology maintain lower outcomes than MCs at 5-year follow-up.
However, in regard to the MCID, PASS, and SCB, patients in the HS cohort achieved clinically meaningful outcomes at similar rates for nearly all PROMs in comparison with the MC cohort at 5 years. This is especially promising as at 2-year follow-up, there are mixed reports in the literature on whether HS cases achieve similar or lower rates of achieving the MCID or PASS than an MC group.1,5,35 The MCID, PASS, and SCB are respectively used to determine the lower boundary of perceived benefit to the patient, the score on a PROM that a patient considers acceptable, and substantial improvement. 27 Although patients in the HS cohort had slightly lower rates of achieving the PASS and SCB on average, these differences were not statistically significant and may reflect lower baseline PROM scores, as these outcomes are based on threshold values. Through these measures, this study offers insight into the appropriate degree of improvement that an HS population can expect after hip arthroscopy. Although it is uncertain if an HS cohort will achieve a similar degree of improvement by 2 years, the group is likely to achieve a similar degree of improvement from baseline at 5 years as compared with an MC group. One potential explanation for the discrepancy between 2- and 5-year outcomes is a difference in recovery trajectory related to baseline symptom severity. Patients with HS syndrome had lower preoperative PROM scores in several measures, which may require a longer duration of improvement to reach absolute threshold-based outcomes such as the PASS and SCB. Unlike the MCID, which reflects a change from baseline, the PASS and SCB represent fixed thresholds of acceptable or substantial improvement. As a result, patients starting with lower baseline scores may appear less likely to achieve these benchmarks at earlier time points, despite experiencing meaningful improvement. Additionally, early postoperative outcomes in the HS population may be influenced by concomitant causes of pain that delay functional adaptation, whereas longer-term follow-up may better capture durable improvement attributable to treatment of the hip pathology.
Furthermore, the weighted difference in mean improvement from baseline to 60-month follow-up refers to the average difference in improvement between groups over time. Notably, the weighted mean improvement scores were statistically similar and in some cases higher for the HS cohort over the 5 years. This finding underscores the potential for such patients to achieve similar levels of progress from baseline as their MC counterparts. While this improvement may not always be apparent in direct functional outcomes, the results of this study highlight the importance of extended prospective follow-up in MC designs and consideration for clinically meaningful outcomes.
Another key finding was that both cohorts reported no revision arthroscopies and similar rates of conversion to THA. A systematic review on hip arthroscopy reported that 58 months was the mean interval to arthroplasty conversion, 32 which underscores the importance of conducting a 5-year follow-up to capture meaningful longer-term outcomes and supports that lumbar spine pathology is not an independent predictor of conversion to THA. Previous studies have additionally shown that patients who receive lumbar spine surgery before hip arthroscopy yield similar rates of improvement to an MC cohort at 5 years. 31 However, these patients also had lower functional outcomes and PASS rates than the MC. Lumbar spine surgery may contribute to decreased spinal mobility, placing higher demands on the hip. 7 As patients in the current study, which excluded previous spinal surgery, reported similar rates of PASS to an MC group, it may be beneficial for future studies to quantify if hip arthroscopy first and lumbar spine surgery second portend better outcomes than lumbar spine surgery first. Yet, in this study, given the small sample size of patients who reported spinal surgery after hip arthroscopy (n = 5), no separate analyses were done to determine if spinal surgery after hip arthroscopy improved outcomes for the HS cohort.
Limitations
The present study should be interpreted in the context of certain limitations. First, patients in the HS cohort did not all present with the same manner of pathology, which may introduce confounding variables. However, stratifying patients by lumbosacral pathology would lead to restrictively small sample sizes, rendering this not feasible at the present time, given the longer-term, prospective follow-up and strict application of eligibility criteria in this study. Second, these findings may not be widely generalizable given the homogeneity of the study's single-institution and highly trained single-surgeon design, particularly in regard to variation in hip arthroscopy techniques and expertise.12,22 This study is limited by the exclusion of patients without a minimum 5-year follow-up, which may introduce attrition bias. Yet, despite the loss to follow-up, the final cohorts remained relatively balanced in size, reducing the likelihood of substantial bias in between-group comparisons. Long-term follow-up was required to assess durable outcomes, and this limitation is common to retrospective studies requiring extended follow-up. This study also included very few patients with isolated cam-type FAI morphology (n = 4), with the majority having pincer or mixed lesions. This limits our ability to draw conclusions about treatment outcomes specific to cam-type morphology and may affect the generalizability of our findings. An additional limitation is the lack of uniform data regarding nonoperative treatment of lumbar spine pathology, including physical therapy and injections, given the heterogeneity in diagnosis and management. While some patients may have received nonoperative lumbar treatments before or during the study period, the long-term follow-up of approximately 5 years reduces the likelihood that short-term symptomatic relief from such interventions substantially influenced the outcomes. Nonetheless, this variability limits more granular assessment of the interaction between lumbar treatment and hip-related outcomes. Finally, though outside the scope of this study, future studies could address whether HS-specific symptoms such as back pain improve over time, using validated measures to further quantify the potential of hip arthroscopy for these patients.
Conclusion
Although patients with hip arthroscopy and concomitant lumbosacral spinal pathology report lower functional outcomes at 5 years than an MC cohort, they can expect similar, if not higher, magnitudes of improvement, as well as similar rates of achieving clinically meaningful outcomes and no increased risk of secondary surgery. These findings substantiate that HS pathology is not an absolute contraindication for hip arthroscopy.
Footnotes
Final revision submitted January 13, 2026; accepted January 18, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mass General Brigham (2013P001442 and 2019P002192).