
Abstract
Background:
Anterior cruciate ligament (ACL) primary repair (ACLPR) has been proposed as a treatment option for select patients with proximal ACL tears. However, long-term data are imperative to validate the utility of this technique.
Purpose:
To determine the long-term incidence of posttraumatic osteoarthritis (PTOA) and clinical outcomes after arthroscopic ACLPR.
Study Design:
Case series; Level of evidence, 4.
Methods:
Prospective data were collected on consecutive patients with modified Sherman type 1 ACL tears who underwent ACLPR between 2008 and 2013. Inclusion required minimum 10-year follow-up. Standardized radiographs of both knees were obtained preoperatively and at 10-year follow-up to assess PTOA as determined by Kellgren-Lawrence (KL) grade and minimal joint space width. Clinical outcomes included repair failure (anterior tibial translation side-to-side difference (ATT SSD) ≥3 mm, grade ≥2 Lachman, grade ≥2 pivot-shift test and/or subjective instability) and reoperation rates, ATT SSD, International Knee Documentation Committee (IKDC) Subjective Knee Form, Lysholm, Forgotten Joint Score–12 (FJS-12), ACL Return to Sport after Injury Survey (ACL-RSI), Tegner activity scale (Tegner), and Patient Acceptable Symptom State (PASS).
Results:
Outcomes were available for 16 of 18 eligible patients (median age at surgery, 40 years; 79% male) with a median follow-up of 11 years (IQR, 10-12 years). PTOA assessment revealed 42% (5/12) KL grade 0, 50% (6/12) grade 1, and 8% (1/12) grade ≥2. There were no significant differences in KL grading compared with preoperative ipsilateral values (P = .69) and contralateral values at 10 years (P = .72). Joint space width in all compartments showed no significant change (all P > .05). Repair failure and reoperation occurred in 12.5% (2/16) of patients each. ATT SSD was 0.9 ± 1.4 mm. Median patient-reported outcome measures were as follows: IKDC, 95 (93-99); Lysholm, 96 (90-100); FJS-12, 96 (90-100); ACL-RSI, 90 (68-100); equal preinjury to postoperative Tegner (P = .25); and PASS was achieved in 92% to 100%.
Conclusion:
At minimum 10-year follow-up, a low incidence of clinically relevant radiographic osteoarthritis was observed in patients who underwent ACLPR. These patients can expect to experience a high rate of clinically significant outcome achievement, preserved knee stability, and an acceptable repair failure rate of 12.5% at long-term follow-up. While the present study provides meaningful insights, validation in larger cohorts remains essential.
The current gold standard for addressing knee instability after anterior cruciate ligament (ACL) rupture is ACL reconstruction (ACLR) using autograft. 68 However, although ACLR reproducibly eliminates translational and rotatory instability while improving functional outcomes, the incidence of posttraumatic osteoarthritis (PTOA) after ACLR remains considerable. 12 Indeed, when defined as Kellgren-Lawrence (KL) grade ≥2, 32 the incidence of PTOA remains an important and unaddressed concern as it has been estimated to affect 11% of patients at 5 years, 21% at 10 years, and 52% at 20 years after ACLR, 11 with a significantly higher rate of PTOA compared with the contralateral healthy knee. 18
The multifactorial etiology of PTOA includes meniscal and chondral injuries at the time of injury,50,66 while the traumatic nature of ACLR may also contribute to PTOA.12,50 Indeed, previous studies have postulated that ACLR introduces a secondary trauma, triggering a second “inflammatory hit” with an acute increase in cartilage degenerative markers.19,31 ACL primary repair (ACLPR) has been proposed as an alternative treatment option for select patients with proximal ACL tears and preserved tissue quality and consists of a surgical technique that is less traumatic to the intra-articular environment.25,39,43,68 ACLPR has been associated with expedited recovery and return to sport (74%), which may be a function of a diminished inflammatory response.2,24,25,61 In a porcine study of Bridge-Enhanced ACL Restoration (BEAR) and ACLR, a reduction in the incidence of PTOA in favor of the BEAR cohort was observed, supporting this hypothesis. 44 However, as modern arthroscopic ACLPR remains a relatively novel treatment option, further long-term data are imperative to validate the utility of this technique for the treatment of proximal ACL tears in select patients.
Therefore, this study aimed to determine the long-term incidence of PTOA and clinical outcomes after arthroscopic ACLPR. The authors hypothesized that ACLPR would confer a low incidence of clinically significant PTOA and favorable clinical outcome measures given the less invasive nature of ACLPR that does not require autograft harvest or reaming of femoral and tibial tunnels for graft docking.
Methods
Patient Selection and Study Setting
The current study received institutional review board approval prior to commencement and was performed according to the ethical standards in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Prospective data were previously recorded and stored in a secure clinical registry, which consisted of consecutive patients presenting with ACL injuries who underwent acute (injury to surgery, ≤21 days), subacute (22-90 days), or chronic (>90 days), isolated (without medial or lateral extra-articular procedure), arthroscopic ACLPR for proximal (modified Sherman type 1), complete ACL tears between January 2008 and December 2013. Inclusion required minimum 10-year follow-up. Indications for surgical intervention were based on the presence of subjective instability, clinical examination, anterior tibial translation side-to-side difference (ATT SSD) >3 mm measured using the Lachmeter (digital Rolimeter; Aircast Europa), and magnetic resonance imaging confirmation of an ACL tear.13,56 As an individualized surgical approach, the final decision for ACLPR was based on careful intraoperative evaluation of the ACL tear location and tissue quality. Patients who underwent ACLPR demonstrated sufficient tissue quality to hold sutures required for repair, while patients with nonrepairable tears including modified Sherman types 2 to 5 were treated with ACLR or augmented ACLPR with all–soft tissue quadriceps tendon autograft.14,57,59 Patients were excluded from the study if they did not undergo ACLPR, were skeletally immature, or underwent additional, simultaneous surgical procedures because of concomitant ipsilateral and/or contralateral ligamentous injuries (Figure 1).

Study flowchart. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; ACLPR, ACL primary repair; CL, contralateral; FU, follow-up; IL, ipsilateral.
Surgical Technique and Rehabilitation Protocol
All surgeries were performed by the senior author (G.S.D.), a fellowship-trained sports medicine surgeon. Intraoperative procedures began with the treatment of meniscal injuries. The ACL was then assessed through direct visualization and probing (Figure 2). Using a grasper, the remnant was carefully evaluated to determine whether it provided sufficient tissue length for reapproximation to its native anatomic origin. Patients with excellent tissue quality, defined by the presence of a broad stump with >50% preservation of the synovial sheath, underwent anatomic double suture anchor repair as described previously (Figure 3).21,22 The anteromedial and posterolateral bundles of the ACL remnant were sutured individually in an alternating Bunnell-type stitch pattern using No. 2 FiberWire and No. 2 TigerWire (Arthrex). A small femoral notchplasty was performed anterior to the ACL anatomic footprint before placement of 2 suture anchors (4.75-mm SwiveLock; Arthrex) for anatomic reattachment of both ACL bundles.

Arthroscopic images (anterolateral portal) demonstrating 4 cases of proximal, complete anterior cruciate ligament (ACL) injury. (A) Patient 1, left knee; (B) patient 1, left knee, demonstration of full detachment using probe; (C) patient 5, right knee; (D) patient 5, right knee; complete separation of the ACL remnant from its femoral footprint; (E) patient 10, left knee; (F) patient 10, left knee, complete, proximal tear; (G) patient 11, right knee; (H) patient 11, right knee; demonstration of full detachment using probe. LFC, lateral femoral condyle; ←, intact synovial sheath with multiple visible capillaries; ↔, marking the tear location with full detachment of the ACL.

Arthroscopic image (anterolateral portal) showing patient 15 undergoing double suture anchor anterior cruciate ligament (ACL) primary repair (left knee). Placement of the anteromedial (black triangles) and posterolateral (black arrows) bundle repair sutures from distally to proximally in an Bunnell-type pattern. Final sutures exit the remnant proximally to optimally reduce the ACL to the femoral wall, with anteromedial sutures (black triangles) exiting medially and laterally and posterolateral sutures (black arrows) exiting on the lateral side. LFC, lateral femoral condyle.
Postoperative rehabilitation allowed for immediate full weightbearing with unlimited passive range of motion (ROM) as tolerated. If meniscal repair was performed concomitantly, weightbearing was limited to toe-touch with ROM from 0° to 90° for up to 4 weeks. During the first 2 to 4 weeks, the use of a brace locked in extension to prevent knee buckling was recommended. Once patients demonstrated the ability to perform 20 consecutive straight leg raises without lag, the brace was unlocked and gradually weaned until unrestricted walking was achieved. Intra-articular knee aspirations were performed in patients presenting with significant effusion that caused restricted ROM and/or arthrogenic muscle inhibition.
Data Collection
As standard of care, patients were routinely followed at 1 week, 1 month, 2 months, 3 months, 6 months, and 1 year, 2 years, and 5 years postoperatively. For the purpose of this study, follow-up was extended to include examinations at 10 years postoperatively. Baseline and follow-up visits adhered to a standardized data collection protocol to ensure consistent long-term data acquisition. At the 10-year follow-up, fully weightbearing anteroposterior (AP), 30° flexion posteroanterior (PA), lateral, and skyline Merchant view radiographs of both knees were obtained as part of the clinical evaluation.
Radiographic Analysis
The primary outcome measure was the incidence of radiographically significant PTOA, defined as grade ≥2 on the KL grading system (0, none; 1, doubtful; 2, minimal; 3, moderate; 4, severe). 32 PTOA was assessed and classified by a musculoskeletal radiologist with >25 years of experience (D.N.M.) and an orthopaedic surgery resident (M.M.M.) in a blinded fashion. If the grading of both observers did not match, the higher grade was used. The definition of KL grade ≥2 as clinically relevant osteoarthritis (OA) has been used in previous studies.3,11,63 The KL grading system has demonstrated good interobserver (0.51-0.89) and intraobserver reliability (0.72-0.87).23,26,32,34,53,67 Additionally, minimal joint space width measurements of the medial and lateral tibiofemoral joint (TFJ) and the medial and lateral patellofemoral joint (PFJ) compartments were conducted on AP, 30° flexion PA, and skyline Merchant view radiographs by a single observer (M.M.M.) (Figure 4). 6 Symptomatic OA was defined as patients with radiographic PTOA presenting with symptoms such as pain, stiffness, tenderness, loss of full ROM, grating sensation, bone spurs, or swelling of the affected knee joint.

Preoperative anteroposterior and skyline Merchant view radiographs (A and D, right knee), postoperative bilateral anteroposterior and skyline Merchant view radiographs (B and E, right knee; C and F, left knee) at 10-year follow-up after double suture anchor anterior cruciate ligament primary repair (right knee). Minimal joint space width (JSW) is marked. (A) The degree of posttraumatic osteoarthritis preoperatively and at 10-year follow-up ([B] ipsilateral and [C] contralateral) was graded as Kellgren-Lawrence grade 1. Presurgery: (A) ipsilateral tibiofemoral joint (TFJ) JSW medial, 5.4 mm; TFJ JSW lateral, 6.3 mm; (D) patellofemoral joint (PFJ) JSW medial, 9.1 mm; PFJ JSW lateral, 7.3 mm. At 10-year follow-up: (B) ipsilateral TFJ JSW medial, 4.9 mm; TFJ JSW lateral, 5.5 mm. (E) PFJ JSW medial, 8.6 mm; PFJ JSW lateral, 7.2 mm. At 10-year follow-up: (C) contralateral TFJ JSW medial, 4.9 mm; TFJ JSW lateral, 6.4 mm; (F) PFJ JSW medial, 8.8 mm; PFJ JSW lateral, 7.0 mm.
Secondary Outcome Measures
Secondary outcome measures included the incidence of repair failure and reoperation, objective ATT SSD knee laxity measurements, Lachman test, pivot-shift test, manual ROM measurements, patient-reported outcome measures (PROMs), and complications at final follow-up. Clinical failure was defined as objective laxity (ATT SSD ≥3 mm, grade ≥2 Lachman, and/or grade ≥2 pivot-shift test) or symptomatic subjective feelings of instability. All clinical assessments were performed by the senior author and included objective ATT SSD measurements. A comprehensive review of medical notes and a standardized interview were conducted to evaluate recurrent symptoms and potential failures, reoperations, surgery-related complications, or subjective recurrent instability. Reoperation was defined as any subsequent surgical intervention other than ipsilateral ACL revision surgery. PROMs were collected including the subjective International Knee Documentation Committee (IKDC), 29 Lysholm score (Lysholm), 36 Forgotten Joint Score–12 (FJS-12), 4 ACL–Return to Sport after Injury (ACL-RSI) score, 64 and Tegner activity scale (Tegner, including preinjury level). 55
Patient satisfaction was assessed based on the dichotomous Patient Acceptable Symptom State (PASS) anchor question: “Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?” Answers of “yes” to this question indicated subjective patient satisfaction, whereas answers of “no” indicated dissatisfaction. For the clinically meaningful outcome analysis, previously established PASS thresholds were utilized, given the small sample size of this study, which statistically precluded the deriving of novel PASS thresholds. Therefore, thresholds derived from a previous study reporting PASS thresholds in a larger population (referenced thresholds: IKDC, 77; Lysholm, 79; FJS-12, 57.3; ACL-RSI, 47.5) were applied. 13 PROMs were not collected for patients who experienced repair failure because these patients were subsequently treated nonoperatively and, therefore, clinical outcome assessment at the 10-year follow-up point would not represent that outcome of ACLPR but rather ACL deficiency.
Statistical Analysis
The normality of distribution was assessed using the Shapiro-Wilk test. Normally distributed data were expressed as mean ± SD. If normality of data could not be confirmed, data were expressed as median with interquartile range, and nonparametric testing was performed using the Friedman test (P < .05). For data with confirmed normality, variances were compared using Levene test (P < .05). If no significant differences in variance were observed, a single-factorial analysis of variance was performed. Categorical variables were compared using the chi-square test (P < .05). Effect size for the observed proportion of events (primary outcome, 8.3%; KL ≥2) compared with an expected rate of 21 % 11 was calculated using Cohen h. To determine the interobserver reliability for KL grading, weighted Cohen kappa (Fleiss-Cohen) was calculated. All statistical analyses were performed using BlueSkyStatistics (Version 10.3.4).
Results
Baseline Demographic and Clinical Characteristics
Outcomes were available for 16 of 18 patients (median age at surgery, 40 (24-44) years; 81.3% male), with a median follow-up of 11 years (IQR, 10-12 years). A detailed overview of baseline demographics and clinical characteristics is provided in Table 1. Median time between injury and surgery was 39 days (23-80 days). Meniscal tears were present in 25.0% of patients (n = 4), with 3 involving the medial meniscus and 1 the lateral meniscus. Partial meniscectomy was performed in 3 cases (1 degenerative bucket-handle medial meniscal tear, 1 posterior horn medial meniscal tear, and 1 posterior horn lateral meniscal tear) and repair in 1 case (medial bucket-handle tear). Concomitant medial collateral ligament injuries were observed in 3 cases (18.8%), all of which were treated nonoperatively. No lateral collateral ligament injuries were identified. A limited mechanical chondroplasty was required in 5 cases of grade 46 2 to 3 chondromalacia (31.3).
Baseline Demographic and Clinical Characteristics a
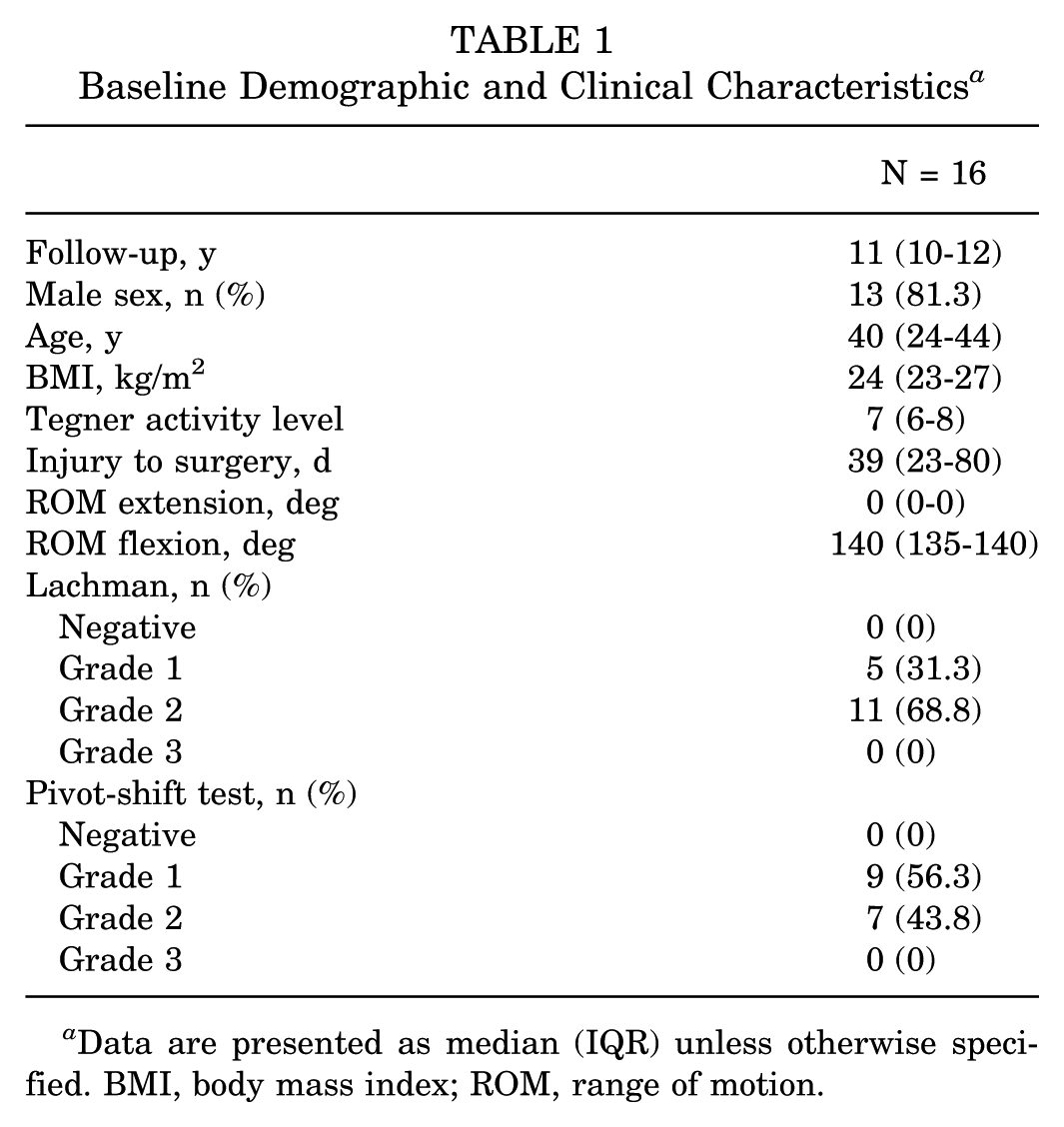
Data are presented as median (IQR) unless otherwise specified. BMI, body mass index; ROM, range of motion.
Incidence of PTOA
Both preoperative and postoperative radiographs of the injured knee joint were available at final follow-up for 12 out of 14 cases. Two patients declined postoperative radiographic evaluation because of the absence of PTOA symptoms (patients 11 and 16). Bilateral radiographs were obtained in 10 cases. At the 10-year follow-up, no patient had clinical symptoms consistent with symptomatic OA. A KL grade of 0 was observed in 41.7% (5/12) of patients, while KL grade 1 was present in 50.0% (6/12) of patients. One case (8.3%; 1/12) of KL grade 3 was observed (initial injury included ACL rupture with concomitant medial and lateral meniscal injury, as well as posterolateral tibial plateau impression fracture [preoperative KL grade 2]) (Table 2). The observed effect size was moderate (Cohen h = 0.36), indicating a notable difference between the observed and expected event rates. Cohen kappa for KL grading reached 0.84 (0.60-0.99) demonstrating high interobserver reliability.
Radiographic Evaluation of Osteoarthritic Features Using KL Grade and JSW a
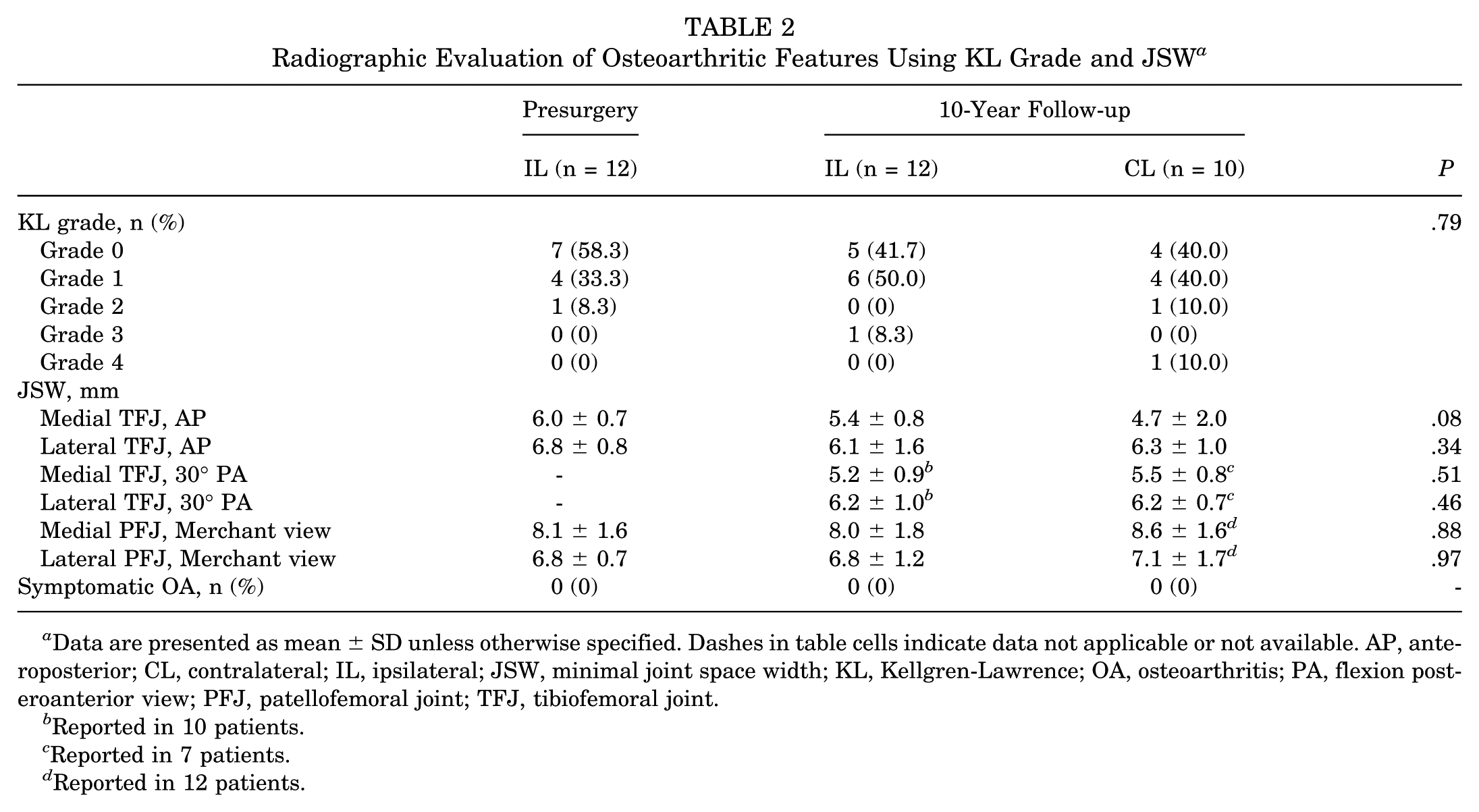
Data are presented as mean ± SD unless otherwise specified. Dashes in table cells indicate data not applicable or not available. AP, anteroposterior; CL, contralateral; IL, ipsilateral; JSW, minimal joint space width; KL, Kellgren-Lawrence; OA, osteoarthritis; PA, flexion posteroanterior view; PFJ, patellofemoral joint; TFJ, tibiofemoral joint.
Reported in 10 patients.
Reported in 7 patients.
Reported in 12 patients.
Contralateral (uninjured) knee radiographs at 10 years showed 40.0% (4/10) KL grade 0 (1 patient with contralateral ACL injury), 40.0% (4/10) KL grade 1, 10.0% (1/10) KL grade 2, and 10.0% (1/10) grade 4 (1 patient with preexisting contralateral multiligament knee injury and surgical reconstruction decades prior). Preoperatively, 58.3% (7/12) of patients had KL grade 0, 33.3% (4/12) KL grade 1, and 8.3% (1/12) with grade 2. An increased PTOA grade (2 patients KL grade 0 to KL grade 1, 1 patient KL grade 2 to KL grade 3) in the ipsilateral knee was noted in 3 of 10 patients at the 10-year follow-up compared with preoperative evaluation. Comparison of radiographic OA as evaluated through KL grading demonstrated no significant 10-year change in the presence of OA features in the ipsilateral knee (P = .69). Likewise, comparison of ACLPR knees at 10-year follow-up compared with the contralateral knee did not demonstrate statistically significant differences in the presence of OA features (P = .72). Furthermore, minimal joint space width of the medial and lateral TFJ, as well as medial and lateral PFJ compartment did not differ significantly between the ipsilateral knee presurgery, ipsilateral knee at 10-year follow-up, and contralateral knee at 10-year follow-up. The 4 patients with concomitant medial or lateral meniscal injury did not exhibit a higher KL grade in the respective compartment compared with the opposite compartment at final follow-up (Table 3).
Individual Values of Recorded Primary and Secondary Outcome Measures a

Primary and secondary outcome measures of the 14 patients included for analysis. Dashes in table cells indicate data not applicable or not available. Not included in this analysis: patients 2 and 12, lost to follow-up; and patients 9 and 14, repair failure. Osteoarthritis grading preoperatively and at 10-year follow-up according to Kellgren-Lawrence 32 : 0, none; 1, doubtful; 2, minimal; 3, moderate; and 4, severe. If the grading of both observers did not match, the higher grade was noted. ACL, anterior cruciate ligament; ACL-RSI, ACL–Return to Sport after Injury; ATT, anterior tibial translation; CL, contralateral; ext, extension; flex, flexion; FJS-12, Forgotten Joint Score–12; FU, follow-up; IKDC, International Knee Documentation Committee; IL, ipsilateral; KL, Kellgren-Lawrence; ROM, range of motion; SSD, side-to-side difference.
Patient with concomitant medial and lateral meniscal injury, as well as posterolateral tibial plateau impaction fracture. Additionally, patient sustained contralateral multiligament knee injury decades prior.
Patient sustained traumatic, sport-related injury on the contralateral ACL.
Patients with concomitant medial or lateral meniscal tear.
Patient sustained fresh medial meniscal injury.
Secondary Outcomes
Two patients (12.5%) experienced sport-related, traumatic ACL reinjury (time to failure, 7 and 10 months). Both patients were treated nonoperatively after consultation with the senior surgeon (G.S.D.). One patient sustained a traumatic, sport-related injury on the contralateral ACL 10 years postoperative, which was managed successfully with ACLPR. Another patient required subsequent ipsilateral meniscal repair due to a fresh medial meniscal injury. The remaining patients experienced no procedure-related complications and did not require additional surgical procedures.
Patients demonstrated a mean ATT SSD of 0.9 ± 1.4 mm with full ROM at 10-year follow-up, while no patients reported subjective recurrent knee instability (Table 4). All patients (100%) reported being very satisfied with the procedure aligning with high PROMs for IKDC, Lysholm, FJS-12, and ACL-RSI scores. Pre- and postsurgery Tegner scores showed no significant (P = .25) differences (Table 5). Nine of 18 patients (50%) reported a presurgery Tegner score of ≥7 (median, 8; IQR, 7-8), and among them, 7/9 (78%) returned to their preinjury activity level, as reflected by comparable Tegner scores at 2-year follow-up and high ACL-RSI values at 10 years (median, 92; IQR, 64-98). The majority of patients achieved the PASS for the subjective IKDC (92%), Lysholm (92%), FJS-12 (92%), and ACL-RSI (100%) score at 10-year follow-up, which did not differ significantly (P > .99) compared with the 2- and 5-year follow-up periods.
Evaluations of ROM and Stability at 2-, 5- and 10-Year Follow-up a

Data are presented as mean ± SD or median (IQR) unless otherwise specified. Bold value denotes statistical significance at P < .05. Dashes in table cells indicate data not applicable or not available. ATT, anterior tibial translation; FU, follow-up; ROM, range of motion; SSD, side-to-side difference.
Significant difference between 2-year FU and 10-year FU and between 5-year FU and 10-year FU.
Reported in 8 patients.
Reported in 11 patients. Outcomes were not assessed for patients who experienced reinjury.
Temporal Changes in Patient-Reported Outcome Measurements a

Data are presented as median (IQR) unless otherwise specified. Dashes in table cells indicate data not applicable or not available. Outcomes were not assessed for patients who experienced reinjury. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; FJS-12, Forgotten Joint Score–12; FU, follow-up; IKDC, International Knee Documentation Committee; PASS, Patient Acceptable Symptom State.
Patient satisfaction according to PASS anchor question.
Discussion
The main findings of the current study were as follows: (1) among patients undergoing selective, arthroscopic ACLPR for proximal, complete ACL tear patterns, a low incidence of clinically significant PTOA as evaluated through radiographic KL grading was detected at a minimum 10-year follow-up; (2) functional and clinical improvements were maintained at long-term follow-up, with all patients demonstrating intact stability (ATT SSD); and (3) a repair failure rate of 12.5% was observed.
At long-term follow-up, only 1 patient (8.3%) in the current study demonstrated radiographic OA, while >40% of patients demonstrated no OA features (KL grade, 0). Furthermore, only 3 patients showed progression compared with the preoperative state. This finding is clinically meaningful, as PTOA may lead to morbidity and accelerate the need for additional treatment interventions such as palliative injections and arthroplasty. Additional surgical and nonsurgical interventions in patients who have previously undergone ACL surgery present a source of additional physiological demand and psychological distress, incur additional costs to health care systems, and are therefore not without consequences.37,45 Current evidence suggests that despite significant technical advancements in ACLR techniques, the PTOA incidence 10 years after ACLR may be as high as 21%, with a 3-fold increased incidence compared with the contralateral (uninjured) knee.3,11 Indeed, Bjornsson et al 5 reported significantly more frequent signs of PTOA after ACLR using hamstring tendon and patellar tendon autograft compared with the uninjured side 16 years postoperatively, suggesting that ACLR or the initial ACL injury perpetuates PTOA. As such, the inflammatory response triggered by the initial injury, compounded by a “second inflammatory hit” from ACLR and elevated cartilage degenerative markers may contribute to increased PTOA risk.19,31 In this context, ACLPR, being less invasive by eliminating the need for large tunnel drilling, may mitigate that second inflammatory hit and partially explain the low rates of PTOA observed in this study.
This concept has been tested in a porcine model, where performing ACL repair with the use of a BEAR implant reduced the inflammatory response compared with ACLR.33,35,44 At 12 months postoperatively, structural properties and objective laxity demonstrated no significant differences between ACL repair with BEAR and ACLR with or without BEAR. 44 However, the mean macroscopic chondral lesion area was notably lower in the BEAR group compared with the ACLR group with BEAR as well as ACLR without BEAR. 44 Further high-level and empirical evidence is necessary to further delineate the mechanisms through which ACLPR may reduce the incidence of PTOA in comparison with ACLR, as the current literature remains anecdotal and inconclusive.9,17,28
Despite previous reports citing a risk of increased residual laxity after ACLPR as compared with ACLR, results from the current study demonstrate sustained restoration of knee stability with a mean SSD of 0.9 ± 1.4mm at 10-year follow-up. 48 This finding is in accordance with biomechanical data demonstrating that ACLPR confers time-zero stability with a mean SSD of 0.2 ± 1.1 mm. 48 As the gold standard, ACLR reproducibly demonstrates improvements in knee stability, 1 yet is associated with high rates of 10-year PTOA as described. Therefore, it does not appear that restoration of stability alone is the primary contributor to the development of PTOA; rather, other factors must explain the variability observed between the rates of PTOA in this study and those observed in ACLR populations.
Sustained improvements in PROMs were observed in this cohort at 10-year follow-up, with 100% reporting satisfaction and over 92% achieving the PASS for all outcome metrics. Furthermore, most highly active patients (78%) returned to their preinjury activity level, aligning with the findings of Annibaldi et al, 2 who reported a 74% return to soccer (94% return to preinjury level) in a cohort of 50 amateur soccer players. Several studies have reported similar or favorable results in the Single Assessment Numeric Evaluation, Marx, FJS-12, Lysholm, IKDC, Knee injury and Osteoarthritis Outcome Score (KOOS), Tegner activity scale, and PASS for ACLPR at short- and midterm follow-up.10,13,24,25 The Multicenter Orthopaedic Outcomes Network (MOON) Study group and other studies reported PROMs of IKDC (81-85), KOOS (75-95), and Lysholm (89-91) 10 years after ACLR.8,41 This cohort surpassed those PROMs suggesting that ACLPR has the potential to restore knee function in the long term. This may be attributed to the less invasive nature of the procedure, which preserves the native ACL and proprioception, thereby promoting more natural knee kinematics and gait patterns compared with ACLR.7,10,54
Historically, studies on ACLPR and ACLR have focused on surgical failure rates as the primary outcome measure, often defined as recurrent objective or subjective instability after surgery. 20 In a previous case series of 113 patients that included a subset of the same cohort as this study, we reported a failure rate of 3.5% in patients >21 years of age and an overall failure rate of 11.5% at short-term follow-up. 62 The Scientific Anterior Cruciate Ligament Network International Study Group confirmed these findings, demonstrating a nonsignificant difference in failure rate between patients >21 years undergoing ACLPR and ACLR. 24 Rilk et al 49 further highlighted this in a meta-analysis, which found no significant differences in failure rates among adults (>21 years). In another systematic review and meta-analysis, Vermeijden et al 60 found a cumulative failure rate of 8% (95% CI, 3.9%-14.4%) after ACLPR, while, as of the current article's publishing, long-term outcomes are still missing. For comparison, at the same follow-up period after ACLR (10 years), Crawford et al 16 reported a cumulative failure rate of 11.9% (graft rupture rate 6.2%, clinical failure rate 10.3%). The MOON Group observed a subsequent surgical revision rate of 7.5% due to failure of ACLR at 6-year follow-up. 42 For patients >40 years of age, studies report failure rates after ACLR ranging between 1.9% and 18.2% (mean follow-up, 2-16 years).15,38 The observed failure rate of 12.5% in this study, although quantified in a small population, aligns with these reported ranges, highlighting ACLPR as a potential viable treatment option for carefully selected patients. It is important to note that patients aged <21 years exhibit a significantly higher failure risk after ACL surgery, a pattern observed for both ACLPR and ACLR.24,47,51,52,65 Rilk et al demonstrated in a meta-analysis a markedly increased revision risk for ACLPR compared with ACLR in this age group (risk ratio, 6.33; P = .03). Vermeijden et al similarly reported a significant failure rate (37%) in patients ≤21 years at 2-year follow-up. Interestingly, a subsequent analysis of the same cohort showed no further increase between 2 and 5 years (37.0% vs 38.5%; P = .92), with non–age stratified failure rates likewise remaining stable (11.5% vs 15.9%; P = .34). 13 Therefore, based on current evidence, although young patient age should not be viewed as an absolute contraindication, it remains a substantial risk factor that must be carefully incorporated into the indication process and patient counseling before proceeding with ACLPR. In this context, combining ACLPR with lateral extra-articular stabilization has been proposed for high-risk patients,25,27,30,40 although definitive evidence supporting this approach is still lacking.
Limitations
Several limitations of this study must be acknowledged. First, the small sample size and the missing control group introduce fragility to the data, limiting the ability to draw definitive conclusions about the long-term value of ACLPR. Second, patients undergoing ACLPR are generally older than ACLR patients,58,59 which confounds direct comparisons of outcomes in a retrospective manner. Third, KL grade was used as a proxy for PTOA, and more specific and quantitative methods, such as T2 cartilage mapping or second-look arthroscopy may be better indicators of PTOA. Fourth, clinical assessments were performed by the senior author, which may introduce observer-related bias. Fifth, PASS thresholds could not be calculated because of the small sample size; therefore, referenced 5-year thresholds 13 were used though they theoretically may not apply. Sixth, there is the potential for selection bias, as patients who ultimately underwent ACLPR were selected intraoperatively by the operating surgeon based on subjective assessment of tear type and tissue quality.
Conclusion
At minimum 10-year follow-up, a low incidence of clinically relevant radiographic OA was observed in patients who underwent ACLPR. These patients can expect to experience a high rate of clinically significant outcome achievement, preserved knee stability, and an acceptable repair failure rate of 12.5% at long-term follow-up. While the present study provides meaningful insights, validation in larger cohorts remains essential.
Footnotes
Final revision submitted December 29, 2025; accepted January 7, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.S.D. receives royalties, owns stock, and is a paid consultant for Zimmer Biomet; receives royalties from Arthrex; received stock options, provides consulting services, and participates in funded research with Miach Orthopaedics; and receives stock options and provides consulting services for OSSIO Inc. K.N.K. received stock options and is a paid consultant for AllaiHealth Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study was approved by the institutional review board of Hospital for Special Surgery (No. 2017-0404).