
Abstract
Background:
Gymnasts, due to repetitive upper extremity weightbearing, are prone to capitellar osteochondritis dissecans (OCD) lesions, which often require surgery and result in time away from sport. Ultrasound has shown promise for detecting early, often asymptomatic, capitellar osteochondral lesions in baseball players; however, it has not been applied to young, healthy gymnasts.
Purpose:
To determine the prevalence and characteristics of capitellar osteochondral abnormalities in young, high-level gymnasts.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This institutional review board-approved study recruited healthy gymnasts aged 10 to 19 years from local gymnastics clubs. The exclusion criteria included treatment for an upper extremity injury within the past 6 months or previous elbow surgery. Participants completed questionnaires to capture sports history and upper extremity function through patient-reported outcomes (PROs). Physical examination assessed elbow extension, valgus alignment, and ultrasound assessed humeral retrotorsion angles. Ultrasound evaluation of the medial elbow and radiocapitellar joint was performed. Comparisons were made between gymnasts with and without capitellar osteochondral abnormalities.
Results:
A total of 62 elbows were evaluated in 31 gymnasts (13.7 ± 2.9 years; 80.6% women). They trained at levels 6 to elite (median, 8.57), with 8.9 ± 3.7 years of gymnastics participation. A total of 15 (24.2%) elbows (9 gymnasts) had radiocapitellar joint abnormalities. Also, 66.7% (n = 6) of gymnasts with radiocapitellar joint abnormalities had bilateral abnormalities. Visualized capitellar changes included 7 concavities of the subchondral plate (11.3%), 6 with subchondral flattening (9.7%), and 2 with division of the subchondral plate (3.2%). Capitellar changes were associated with pain with palpation of the radiocapitellar joint (P < .01) and dominant arm Single Assessment Numeric Evaluation Elbow Score (P = .02). Capitellar changes were not associated with other PROs (P > .05), gymnast level (P = .80), years in sport (P = .90), elbow extension (right, P = .45; left, P = .68), or valgus differences (right, P = .39; left, P = .22).
Conclusion:
One in 4 high-level youth gymnasts demonstrated capitellar osteochondral abnormalities, often bilateral and associated with pain to palpation over the radiocapitellar joint but unrelated to function. Prospective studies are needed, but ultrasound screening may allow earlier detection of capitellar OCDs in youth gymnasts.
Gymnastics is a globally popular sport, with an estimated 4.76 million participants in the United States alone, the majority of whom are female youth athletes. 16 Achieving elite status in gymnastics requires early specialization and intensive training from a young age; however, <1% of gymnasts ultimately reach elite levels.6,14,18 The sport's demanding nature, particularly the repetitive weightbearing on the upper extremities, predisposes gymnasts to both common and unique musculoskeletal injuries. 22
Among these injuries, capitellar osteochondritis dissecans (OCD) has emerged as a particularly concerning condition. During tumbling and other high-impact maneuvers, forces transmitted through the radiocapitellar joint can exceed 200% of a gymnast's body weight. 20 This repetitive stress is believed to contribute to the development of OCD lesions affecting the cartilage and subchondral bone of the capitellum.9,11,25 Left untreated, capitellar OCDs can lead to early onset elbow osteoarthritis, chronic pain, and functional decline. 2 Even with treatment, OCD lesions often result in prolonged time away from sport, with 80% of affected gymnasts ultimately requiring surgery and a significant number not returning to their previous level of competition. 25
Early detection of capitellar OCD is critical to improving outcomes and minimizing the need for surgical intervention. In youth baseball players, ultrasound has been validated as an effective, noninvasive, portable, and radiation-free imaging modality capable of identifying early, often asymptomatic, capitellar OCD lesions.8,12 Prevalence studies in baseball report OCD detection rates of 1% to 7% in the dominant elbow, with 70% of cases being asymptomatic at diagnosis.8,11,21 Importantly, ultrasound-guided early detection in baseball populations has facilitated conservative treatment in up to 80% of cases, enabling a quicker return to sport and reduced morbidity.8,10,13,23
In contrast, no ultrasound-based screening studies have been conducted in gymnasts, despite their higher risk profile and a tendency to develop bilateral capitellar OCD lesions, which are associated with increased morbidity and surgical necessity.1,25 The absence of established screening protocols represents a significant gap in the potential of preventive care for this vulnerable athletic population.
Given this information, our study aimed to determine the prevalence of radiocapitellar osteochondral abnormalities in healthy, competitive youth gymnasts using ultrasound screening. We further sought to evaluate associations between ultrasound findings and pain with palpation, patient-reported outcomes (PROs) related to elbow function, gymnastic characteristics, and physical examination measures. By identifying asymptomatic or early-stage abnormalities, this study may inform future screening and management strategies improve long-term athletic and health outcomes in young gymnasts.
Methods
Study Design
This study employed a cross-sectional, descriptive diagnostic epidemiology design to evaluate the prevalence of radiocapitellar osteochondral abnormalities in healthy, competitive youth gymnasts. The study protocol was approved by the local institutional review board.
Participants
Participants were recruited from several local gymnastics clubs through 2 primary strategies: either during community outreach events offering ultrasound scanning at the sports medicine clinic or at on-site events where ultrasound evaluations were conducted at participating gymnastics gyms. Eligible athletes were actively training at Level ≥6 and between the ages of 10 and 19 years. The inclusion criteria included current participation in gymnastics at Level ≥6, ability to provide informed consent or assent (with parental consent for minors), and no known congenital abnormalities of the elbow. Athletes were excluded if they had a history of previous elbow surgery, had been treated for an upper extremity injury within the past 6 months, or were unable to complete the ultrasound examination.
Procedures
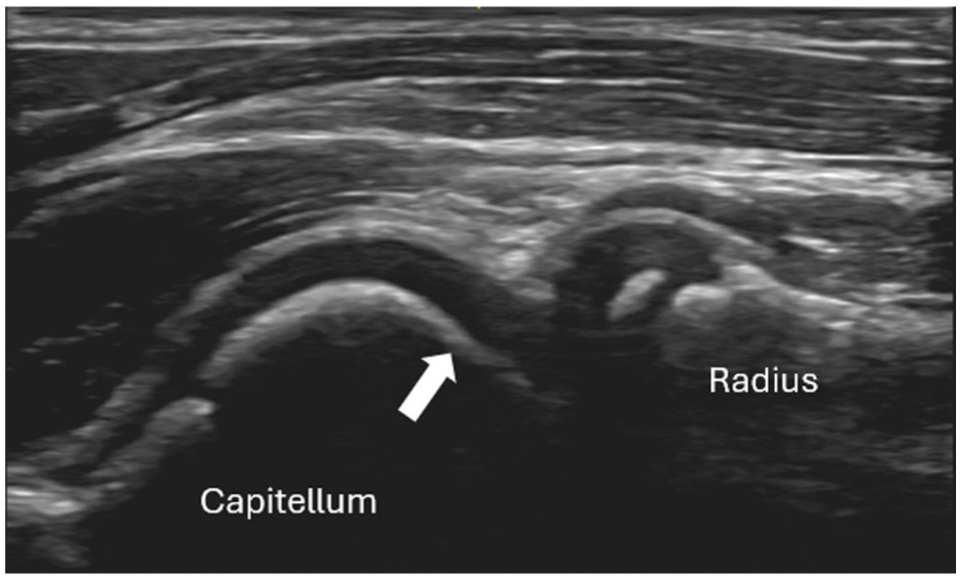
Each participant underwent a standardized ultrasound evaluation of both elbows, performed and interpreted by a sports medicine physician with dual fellowship training in sports medicine and musculoskeletal ultrasound (J.J.). Previous studies have demonstrated a high correlation between ultrasound and intraoperative findings of capitellar abnormalities. 26 Ultrasound examinations were performed using a high-resolution, portable ultrasound machine (GE Venue Go) equipped with a 4 to 20 MHz linear transducer. The examination protocol focused on complete visualization of the radiocapitellar joint to assess for osteochondral abnormalities—including subchondral plate flattening, concavity, or division (Figure 1). This was done by obtaining sagittal views of the anterior and posterior aspects of the joint and scanning medially and laterally to visualize the entirety of this joint. Additional assessment of the medial epicondyle and ulnar collateral ligament was included to screen for other musculoskeletal abnormalities—including tears or avulsions. These were visualized with the transducer in the long-axis (coronal) view, with additional short-axis views (axial) obtained if abnormalities were observed. Ultrasound findings were interpreted by the same ultrasound physician, which involved subjective interpretation.

Anterior sagittal view of a normal appearing radiocapitellar joint. Notice the normal, smooth, rounded appearance of the hyperechoic (white) subchondral plate of the capitellum signaled by the arrow.
In addition to the ultrasound examination, participants completed a series of validated questionnaires to assess sports participation history and upper extremity function. These included the Sports Activity and Functional Evaluation survey to document years of gymnastics participation, frequency, and training history; the Pediatric Functional Activity Brief Scale (Pedi-FABS) (range, 0-30), where higher values equate to high level of physical activity; 4 the Patient-Reported Outcomes Measurement Information System (PROMIS) 7+2 Global Health (range, 16-74), where higher scores indicate a better physical and mental health;3,19 the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH), including the Sports/Performing Arts and Work modules (range, 0-100), with higher levels signifying a greater level of disability; 5 and the Elbow and Shoulder Single Assessment Numeric Evaluation (SANE) for the dominant arm (range, 0-100). 17 The SANE PRO asks to separately rate the dominant elbow and shoulder as a percentage of normal (0%-100%). 17
A brief physical examination of each athlete's elbows was performed by the same clinician to assess bilateral elbow extension and degree of valgus using a goniometer (J.J.). Elbow extension range of motion was measured using a standard goniometer with the fulcrum positioned over the medial epicondyle, the stationary arm aligned with the midline of the humerus, and the moving arm aligned with the ulnar shaft. Valgus alignment was assessed with the elbow in neutral extension (180°) by placing the goniometer over the anterior aspect of the arm, aligning the stationary arm with the humeral shaft and the moving arm along the ulnar and radial shafts. Additionally, the physician assessed for pain with focal palpation over the anterior radiocapitellar joint. The athlete reported the presence or absence of pain in this area on bilateral elbows, and their responses were recorded for comparison.
Humeral retrotorsion angles were measured using the indirect ultrasound humeral inclination angle technique described by Myers et al. 15 Participants were positioned supine with the shoulder abducted to 90° and the elbow flexed to 90°. A linear transducer was placed on the anterior shoulder, level with the table and perpendicular to the long axis of the humerus in the frontal plane. The humerus was rotated until the intertubercular line between the greater and lesser tubercles appeared parallel to the horizontal plane on the ultrasound image. The corresponding inclinometer was placed over the distal ulna to measure the humeral inclination angle.
Data Management and Analysis
All data—including ultrasound findings, physical examination results, and questionnaire responses—were securely stored in a password-protected database accessible only to the research team. Descriptive statistics were calculated to summarize participant characteristics, ultrasound findings, and PROs. Any one of the findings of subchondral plate flattening, concavity, or division was defined as a radiocapitellar osteochondral abnormality in the comparisons. The prevalence of radiocapitellar osteochondral abnormalities was reported as the proportion of affected elbows divided by the entire cohort. Independent samples t tests and Mann-Whitney U tests were conducted to examine associations between ultrasound radiocapitellar abnormalities and ultrasound measurements and PROs. Mann-Whitney U tests were applied to continuous data after rejecting the hypothesis of data normality. Statistical significance was defined as P < .05.
Results
A total of 62 elbows from 31 gymnasts (80.6% women) were enrolled in the study, with a mean age of 13.7 ± 2.9 years. Participants had a mean of 8.9 ± 3.7 years of gymnastics participation and trained at levels ranging from 6 to elite, with a median gymnastics level of 8.57. Further participant characteristics and elbow measurements are presented in Table 1.
Participant Characteristics and Elbow Measurements

Radiocapitellar osteochondral abnormalities were identified in 15 elbows (24.2%) in 9 gymnasts. Among gymnasts with osteochondral changes, 66.7% (6 of 9) exhibited bilateral radiocapitellar abnormalities. Specific ultrasound findings included 6 elbows (9.7%) with subchondral flattening (Figure 2), 7 elbows (11.3%) demonstrating concavity of the subchondral plate (Figure 3), and 2 elbows (3.2%) with division of the subchondral plate (Figure 4). Additionally, healed medial epicondyle avulsion was observed in 2 elbows (3.2%), and a sublime tubercle avulsion was identified in 1 elbow (1.6%).
Anterior sagittal view of a capitellum with subchondral flattening. Notice the loss of normal contour and subtle flattening of the subchondral plate (arrow).

Anterior sagittal view of a capitellum with subchondral concavity. Notice the concavity appearance of the subchondral plate at the capitellum articulation with the radial head (arrow).

Anterior sagittal view of a capitellum with subchondral division. Notice the division within the subchondral plate of the capitellum at its articulation with the radial head (arrow).
The number of years in sport did not differ between participants with and without capitellar osteochondral abnormalities (mean, 9.75 ± 4.40 vs 8.62 ± 3.44 years, respectively; P = .47). Additionally, the presence of capitellar osteochondral abnormalities did not differ by level of gymnastics competition (present 9.25 ± 1.67 vs absent 8.57 ± 1.29; P = .25).
Pain with palpation over the radiocapitellar joint was reported in 66.7% (n = 10/15) of elbows with osteochondral abnormalities compared with 17% (n = 8/47) of elbows without abnormalities, a statistically significant difference (P < .01). No statistically significant associations were found between the presence of radiocapitellar osteochondral abnormalities and PROs (Table 2) or physical examination measures (Table 3). Specifically, radiocapitellar changes were not associated with Pedi-FABS scores or SANE Elbow Function scores. Additionally, there were no significant differences in elbow extension, valgus, or humeral retrotorsion angles between participants with osteochondral abnormalities and those without, for either the right or left elbows (all P > .05) (Table 3).
Sport History and PROM Comparisons Between Those With and Without Capitellar Abnormalities a
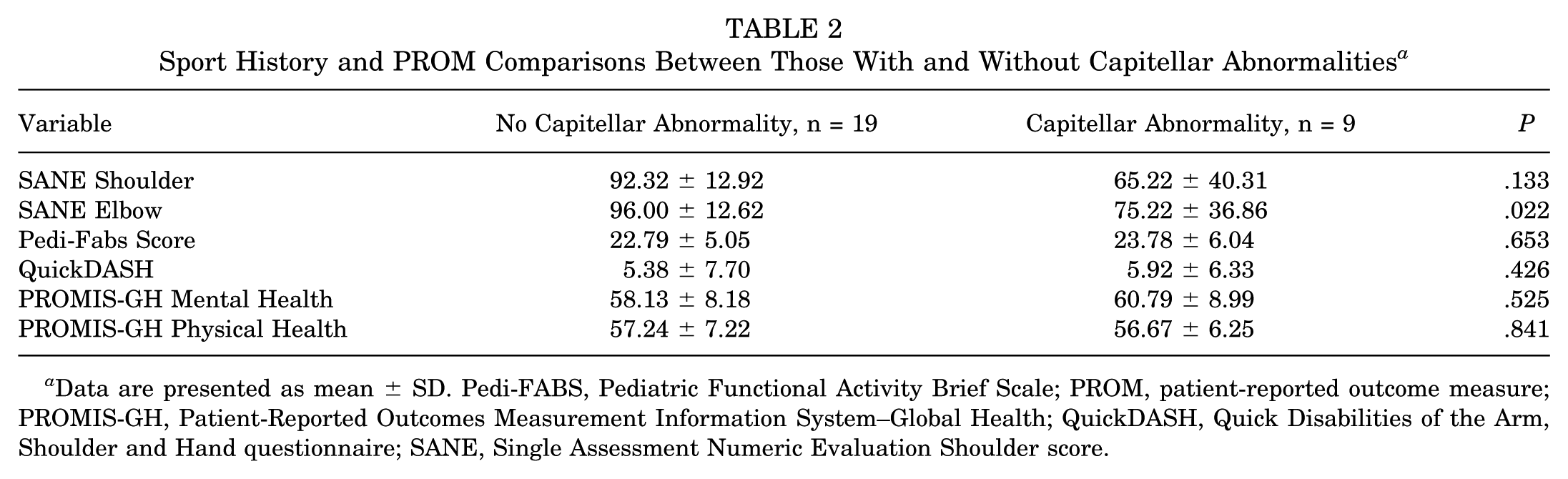
Data are presented as mean ± SD. Pedi-FABS, Pediatric Functional Activity Brief Scale; PROM, patient-reported outcome measure; PROMIS-GH, Patient-Reported Outcomes Measurement Information System–Global Health; QuickDASH, Quick Disabilities of the Arm, Shoulder and Hand questionnaire; SANE, Single Assessment Numeric Evaluation Shoulder score.
Elbow Measurement Comparisons Between Those With and Without Capitellar Abnormalities a

Data are presented as (n) mean ± SD.
Discussion
This study aimed to determine the prevalence of radiocapitellar osteochondral abnormalities in healthy, competitive youth gymnasts using ultrasound screening, and to examine the relationship between these abnormalities and pain to palpation over the radiocapitellar joint, PROs related to elbow function, gymnastic characteristics, and physical examination measures.
In this study, nearly one-fourth (24.2%) of elbows in healthy, competitive youth gymnasts demonstrated radiocapitellar osteochondral abnormalities on ultrasound, despite the absence of significant differences in reported competition level, years in sports, reported function, the amount of extension, and elbow valgus. However, pain with palpation over the radiocapitellar joint was present in two-thirds of gymnasts with imaging abnormalities and occurred significantly more frequently than in those without osteochondral abnormalities (P < .01). These findings align with a previous study by Dexel et al 4 who reported radiocapitellar abnormalities on elbow magnetic-resonance imaging (MRIs) on 30 high-level youth gymnasts. One-third demonstrated radiocapitellar abnormalities, of which 70% were capitellar OCDs. Similarly, 60% with radiocapitellar abnormalities endorsed symptoms, while the remaining 40% were asymptomatic.
Notably, two-thirds of gymnasts in our cohort with abnormalities exhibited bilateral lesions. This pattern contrasts with the predominantly unilateral findings reported in other overhead athletes, such as baseball players.8,12 These findings suggest that gymnasts, due to their sport-specific bilateral upper extremity loading, may be uniquely predisposed to bilateral capitellar involvement. This aligns with previously published literature. 1 The prevalence observed in this cohort is substantially higher than reported rates in asymptomatic youth baseball players, where ultrasound screening studies have identified capitellar osteochondral abnormalities in 1% to 7% of dominant arms.8,21 This disparity may reflect the greater mechanical demands placed on the elbow in gymnastics, the bilateral loading inherent to many gymnastics skills, and the fact that our cohort focused exclusively on higher-level gymnasts who possess skills involving regular upper extremity weightbearing. The frequent occurrence of subchondral concavities, flattening, and divisions observed in our cohort may represent a spectrum of early-stage osteochondral injury.
Given the relatively high prevalence of abnormalities detected on imaging, we identified that two-thirds of those with endorsed pain on palpation had abnormalities. This was significantly higher compared with those without any capitellar abnormalities (P < .01). This association suggests that a portion of these abnormalities may reflect underlying local injury. On the contrary, we did not identify significant associations with PROs, physical examination findings, or humeral retrotorsion angles. Previous ultrasound screening literature in youth baseball players demonstrated that the majority of ultrasound-detected OCD lesions were asymptomatic.8,11 Although the clinical implications of these abnormalities in our study remain incompletely understood, the ability to detect abnormalities raises questions about the natural progression of these abnormalities. Furthermore, whether and how such findings progress to OCDs may help inform optimal treatment timing; however, our study lacks these data. Prospective studies are needed to inform whether early identification influences OCD development and ultimately improves clinical outcomes.
The high prevalence of bilateral abnormalities further raises questions about the cumulative impact of repetitive bilateral upper extremity loading in gymnastics. Unlike unilateral sports, gymnastics demands symmetrical weightbearing and impact forces across both elbows during skills such as tumbling, vaulting, and parallel bar maneuvers. 20 The presence of bilateral abnormalities in two-thirds of affected gymnasts in this study suggests that bilateral screening may be critical in gymnastics populations, rather than focusing solely on a dominant extremity as done in other overhead athletes. 8
Whereas ultrasound lacks fluid-sensitive sequencing, as in MRI, it offers superior resolution for superficial structures. 7 This allows for detailed visualization of the capitellum, not limited by the slice thickness of other advanced imaging modalities. 7 Additionally, ultrasound has demonstrated a high correlation with intraoperative findings, superior to MRI, for capitellar OCDs’ articular contours. 26 This suggests ultrasound can accurately assess early changes in the articular cartilage and subchondral bone of the capitellum while lacking the fluid-sensitive sensing present on MRIs.
Future research should explore longitudinal follow-up of gymnasts with abnormalities to assess lesion evolution and evaluate whether early detection and intervention can improve clinical outcomes. Additionally, expanding screening efforts to larger, more diverse gymnastics populations may better define prevalence and risk factors for radiocapitellar abnormalities in this unique sport.
Several limitations should be noted. First, the cross-sectional design precludes assessment of lesion progression, improvement over time, or direct correlation with symptom development; progression to surgical threshold was not followed. Longitudinal studies are necessary to determine which ultrasound-detected abnormalities may evolve into more clinically significant OCD lesions. Second, the relatively small sample size focusing on a higher-level gymnast cohort limits the ability to detect subtle associations between imaging findings and clinical or training variables. Consequently, any analysis of other variables would have been underpowered and was therefore not performed. Third, we obtained SANE scores only from the dominant elbow and shoulder, which limits the ability to assess side-to-side functional differences with the nondominant elbow. Finally, although the ultrasound protocol was standardized and performed by a single experienced musculoskeletal sonography provider (J.J.), this could introduce observer bias. The inclusion of additional raters would strengthen reliability.
Conclusion
Ultrasound screening identified radiocapitellar osteochondral abnormalities in approximately one-fourth of elbows in healthy, competitive youth gymnasts, with a predominance of bilateral abnormalities. These abnormalities are associated with pain to palpation over the radiocapitellar joint but are unrelated to reported function. Prospective studies are needed; however, ultrasound screening may allow earlier detection of capitellar OCDs in youth gymnasts.
Footnotes
Final revision submitted January 5, 2026; accepted January 12, 2026.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Institutional Review Board of the University of Texas Southwestern (STU082010-134).