
Abstract
Background:
Frequent pivoting, rotation, and deep hip flexion place football players at high risk for femoroacetabular impingement (FAI), a leading cause of hip pain in this population. Previous studies have primarily focused on professional National Football League athletes undergoing mixed surgical techniques, including labral debridement. Limited data exist on outcomes in younger, amateur players treated with labral repair.
Purpose:
To report return to sport (RTS) rates and functional outcomes at a minimum 5-year follow-up in primarily active high school and college football players undergoing primary hip arthroscopy with labral repair for FAI.
Study Design:
Case series, Level of evidence, 4.
Methods:
All football players who underwent primary hip arthroscopy with labral repair for FAI between 2010 and 2019 were identified from an institutional database. Collected data included descriptive data, radiographic parameters, surgical details, and reoperations. At a minimum 5-year follow-up, RTS outcomes and patient-reported outcome measures (PROMs), such as the Modified Harris Hip Score (mHHS) and Hip Outcome Score (HOS), were evaluated.
Results:
A total of 36 hips in 27 male athletes (mean age, 18 years; body mass index, 28.1 kg/m2) were included. The majority of athletes competed at the high school (70%) or collegiate level (26%). Mean preoperative radiographic measurements were as follows: lateral center-edge angle, 31.6°; Tönnis angle, 4.1°; and alpha angle, 61.4°. Femoroplasty and acetabuloplasty were performed in 100% and 86% of cases, respectively. Also, 84% of players returned to football, all at the same or higher level than before surgery. At a mean follow-up of 9.8 years, all PROMs improved significantly from baseline (P < .002). Outcome scores at follow-up were as follows: mHHS 90.5; HOS-Activities of Daily Living, 94.5; HOS-Sports-Specific Subscale, 91.1; and visual analog scale (VAS) pain with use, 2.3/10; VAS pain at rest, 1.3/10; and surgical satisfaction, 8.5/10. No patients required revision surgery. However, 2 patients (7%) underwent reoperations—including 1 for heterotopic ossification excision and 1 for periacetabular osteotomy.
Conclusion:
American football players who underwent primary hip arthroscopy with labral repair for FAI achieved excellent long-term outcomes, with high RTS rates at the same or higher levels, and improvements in PROMs and patient satisfaction. Despite favorable outcomes, nonmedical factors, such as graduation, may influence RTS in competitive athletes, particularly at the high school and collegiate levels.
Femoroacetabular impingement (FAI), initially described as an abnormality of the morphology of the proximal femur or acetabulum, is a common cause of hip pain that can impact quality of life.2,10,16 More recently, a consensus statement described FAI as “a motion-related clinical diagnosis of the hip that represents symptomatic contact between the proximal femur and acetabulum.” 11 The syndrome can be further characterized as abnormal contact between the femoral head-neck junction (cam-type), acetabulum (pincer-type), or mixed (cam and pincer-type). 34 It has been previously theorized that FAI results from increased stresses around the extension of the physeal scar near the femoral head epiphysis during skeletal growth.28,31 Thus, skeletally immature athletes may be at an increased risk of developing FAI. The prevalence of cam-type deformities in athletes has been reported to be twice that of the general population, 8 with one series of 200 patients with FAI reporting that 70% of patients <30 years old were involved in athletics. 3
While athletes have reported high rates of FAI, football players in particular may be at an increased risk. Nepple et al 22 assessed radiographs of 107 National Football League (NFL) players with reported groin pain and found radiographic markers of cam and/or pincer type FAI in 94.3% of hips. Furthermore, in a radiographic study of 134 hips of collegiate football players, 95% had at least 1 sign of cam or pincer impingement, with 65% having pincer deformities, 78% having cam deformities, and 50% having mixed type. 14 In part, this is theorized to be due to the high amount of mechanical stress exerted on the femoral head-neck junction and acetabulum during training and competition.
Arthroscopic treatment of FAI has become increasingly common, with proponents of this technique citing a lower rate of complications and morbidity compared with traditional open approaches like surgical hip dislocations. 17 A meta-analysis of 1981 hips demonstrated a 1.7% risk of clinical complications, with 87.7% of patients returning to sports (RTS). 20 Further studies assessing RTS after arthroscopic treatment for FAI have demonstrated favorable RTS rates reported between 26 71.4% and 9 93.7%. Two of the largest studies analyzing RTS in NFL players after hip arthroscopy for FAI demonstrated excellent outcomes, with Menge et al 18 reporting a RTS rate of 87% in 51 players, and Sochacki et al 29 reporting a RTS rate of 84% in 55 players
However, despite the common belief that FAI is related to repeated mechanical stress in skeletally immature patients, there is a paucity of literature evaluating RTS and patient-reported outcomes in young, competitive athletes. One such study of 104 adolescent athletes (mean age, 16 years) reported an 86% RTS rate after hip arthroscopy for FAI. However, this cohort included only 17 football players who had undergone labral debridement. 4 Two additional studies examined multisport, nonprofessional athlete cohorts that included only small subgroups of contact athletes (football, wrestling, rugby).32,33 One study of 39 National Collegiate Athletic Association (NCAA) Division I athletes (mean age, 20 years) reported a 93% RTS rate at 2-year follow-up. 33 The second, involving both amateur recreational and nonprofessional athletes (mean age, 27 years), found smaller improvements in Hip Outcome Score–Activities of Daily Living (HOS-ADL) scores for contact athletes and reported a 92% RTS rate for the overall multisport cohort. 32 While these studies provide useful context, their multisport design and limited representation of football players underscore the continued lack of data isolating RTS and functional outcomes in young American football athletes.
There are over 1 million estimated high school football participants. Yet only 7.5% of these players transition to playing at any level of NCAA division I, II, or III football, highlighting the large subset of high school athletes who choose not to pursue competitive athletics at the next level. 21 Previous work has suggested that adolescents may stop playing sports for several reasons—including changing priorities (eg, a shift in focus to academics) and life events (eg, graduation).24,27,35 Despite the disparity in the number of high school athletes playing in college, as college sports enter the Name, Image, and Likeness era, the potential financial incentives for both high school athletes pursuing college football as well as college football players to RTS successfully will likely continue to influence management of FAI, underscoring the importance of understanding management of this condition. 12
Therefore, this study aimed to report RTS rates and patient-reported outcomes (PROMs) in a cohort of competitive, nonprofessional American football players with arthroscopically treated FAI and labral repair at a minimum 5-year follow-up. We hypothesized that these athletes would RTS at a high rate with good PROMs; however, given the age of the cohort, other factors could lead to a lower RTS rate than in studies reporting on professional athletes.
Methods
Study Design
A prospectively maintained institutional hip arthroscopy database containing 1788 primary labral repairs (1624 patients) performed between 2010 and 2019 (performed by authors A.J.K and B.A.L.) was retrospectively reviewed following institutional review board approval (IRB) (IRB No.: 08-002259). The inclusion criteria consisted of preoperative participation in American Football (within 1 year before surgery) at any nonprofessional level of competition (high school, collegiate, or semi-professional), clinical and radiographic diagnosis of FAI with a labral tear, undergoing primary hip arthroscopy and labral repair for FAI, and a minimum of 5-year follow-up with clinical outcomes. Patients were excluded if they had a history of hip dysplasia, previous hip surgery, Legg–Calvé–Perthes disease, slipped capital femoral epiphysis, underwent labral debridement without repair, required concomitant or staged periacetabular osteotomy, or had discontinued football participation preoperatively for nonhip-related reasons. Patients were not limited to age, sex, body mass index (BMI), or participation in multiple sports. Although no formal age restriction was applied, the cohort was self-selected toward athletes aged < 25 years due to the nature of American football participation. Preoperative anteroposterior and lateral pelvic radiographs were evaluated for alpha angles, lateral center-edge angles (LCEA), and Tonnis angles and grading. Intraoperative characteristics recorded included type of capsulotomy (interportal versus T-capsulotomy), femoroplasty, acetabuloplasty, and capsular repair.
Data Collection
After applying the inclusion and exclusion criteria (Figure 1), eligible patients were contacted at a minimum of 5 years postoperatively by telephone or email to complete validated clinical outcome questionnaires, including return to football and football characteristics, using REDCap electronic capture tools (Vanderbilt University). RTS was defined as participation in at least 1 competitive football game postoperatively. RTS status and reasons for non-return were obtained for all 27 patients (100%). Validated PROMS—including the Modified Harris Hip Score (mHHS), HOS, HOS-ADL, HOS Sports-Specific Subscale (HOS-Sport), Tegner Activity Scores, visual analogue scale (VAS) for pain with rest and use, VAS 5-point scales, and patient surgical satisfaction—were collected for 19 patients (70%). The mHHS and HOS scores were graded on a 0 to 100 scale, while the Tegner Activity Score, VAS for pain, and surgical satisfaction were graded on a 0 to 10 scale. RTS was defined as returning to football at any time postoperatively. Electronic medical records were assessed for demographic information—including age at the time of surgery, sex, BMI, and hip laterality—and operative notes were assessed for intraoperative characteristics.

CONSORT flow diagram. CONSORT, Consolidated Standards of Reporting Trials.
All patients were analyzed for RTS outcomes according to an intention-to-treat approach, with missing PROM data excluded on a per-variable basis. To minimize recall bias, standardized survey questions and validated outcome instruments were used, supplemented by chart review for descriptive and operative data.
Surgical Technique
All procedures were performed with patients positioned on a modified traction table to allow distraction of the operative hip. Standard anterolateral and mid-anterior arthroscopic portals were routinely established. In certain cases, supplementary distal anterolateral or posterolateral portals were utilized at the discretion of the surgeon based on intraoperative evaluation. Capsulotomy was performed via either a T-type or interportal approach according to the surgeon's preference. Bony pathology was addressed through femoroplasty and/or acetabuloplasty. Labral tears were treated in all patients with arthroscopic suture anchor-based repair. Capsular closure was performed in most cases (94%), whereas a subset (6%) did not undergo repair at the surgeon's discretion. Intraoperative fluoroscopy and postoperative radiographs were used to confirm appropriate FAI correction.
Postoperative Rehabilitation
All patients underwent a standard hip arthroscopy rehabilitation protocol. For the first 2 weeks, patients were partial weightbearing with a predominantly passive range of motion (ROM) of the hip. At 2 weeks, patients began progressive loading with weightbearing as tolerated and were instructed to wean off any assistive support. ROM to tolerance in all planes was permitted. Goals for the 6- to 12-week period were to ambulate independently with natural gait, achieve full pain-free ROM, and progress resistance as tolerated. Starting at the 12-week mark, patients were allowed to resume jogging and other plyometric activities with physician approval. Regarding RTS, a goal to achieve a limb symmetry index of 75% in objective strength and functional tests, such as Y-Balance, by week 12 was set. After 16 weeks, patients progressed to American football-specific tasks and repeat strength testing, aiming to achieve 90% limb symmetry index for clearance to full RTS. These RTS criteria were incorporated into the postoperative hip arthroscopy rehabilitation protocol based on previous literature that has established quantitative thresholds to improve the likelihood of a successful RTS.7,13
Statistical Analyses
Descriptive and RTS data are reported using descriptive statistics such as sample sizes and percentages, and mean ± standard deviations (Microsoft Corporation, Redmond, WA, USA; Microsoft Excel Version 2411). Due to the limited sample size, univariate logistic regression analyses were used to investigate predictors of RTS, reporting odds ratios with 95% CIs, and P values. No formal power analysis was performed due to the retrospective nature and fixed sample size of this cohort. This regression analysis may therefore be underpowered, and results should be interpreted with this potential for type 2 error in mind. Preoperative and postoperative clinical outcomes were compared using Student t tests or Wilcoxon rank-sum tests (Mann-Whitney U), after testing for normality (Shapiro-Wilk test). They were reported as mean ± standard deviations, 95% CIs, and P values. Previously established minimum clinically important difference (MCID) thresholds for patients with FAI at a minimum 5-year follow-up were applied: 14.4 for mHHS, 10.6 for HOS-ADL, and 15.4 for HOS-Sport.1,23 Postoperative clinical outcomes were further evaluated to compare outcomes between patients who returned to football and those who did not. P < .05 was considered statistically significant. Statistical analyses were conducted in RStudio (RStudio Team; RStudio Version 4.4.1).
Results
Descriptive Data
A total of 27 male, nonprofessional American football players (36 hips) were included in this study, with a mean age of 18 ± 2.7 years and a mean BMI of 28.1 ± 7 kg/m2 (Table 1). There was a statistically significant difference in the number of high school athletes (70%) compared with college (26%) or semiprofessional (4%). A total of 48% right hips were involved, compared with 19% left and 33% bilateral. There were 13 linemen compared with 12 nonlinemen. As evaluated radiographically, the mean LCEA angle was 31.6º± 6.3°, the mean Tönnis angle was 4.1º± 3.8°, and the mean alpha angle was 61.4º± 12.5°. An interportal capsulotomy was performed in 61% of hips, while a T-Capsulotomy was performed in 39% of hips. The labrum was repaired in all cases. Femoroplasty was performed in all hips and acetabuloplasty in 86% of hips. In 94% of hips, the capsule was primarily repaired. All T portions of the capsulotomies were repaired in cases of T-capsulotomy.
Descriptive Data of Football Players a

Data are presented as mean ± SD or n (%). The bold P value indicates statistical significance. LCEA, lateral center-edge angle.
Return to Football
Of the 27 American football players in this study, 19 (70%) attempted to RTS after surgery. Sixteen athletes (84%) successfully returned to football at the same or higher level than before surgery (Table 2), with a higher level defined as advancing to a more competitive tier of play (eg, high school to collegiate). In this cohort, 2 high school athletes returned to college-level competition postoperatively. Of the 3 athletes who attempted RTS, one did not return due to hip limitations, and the other two were unable to return due to other injuries. Eight athletes did not attempt to return to football for nonmedical reasons (such as graduating, changing priorities, etc, Figure 2). When these athletes were included, the overall RTS rate was 59% (16 of 27). The clinical RTS rate, representing athletes limited by hip function or injury, was therefore 84%.
RTS Outcomes in Football Players After Hip Arthroscopy a
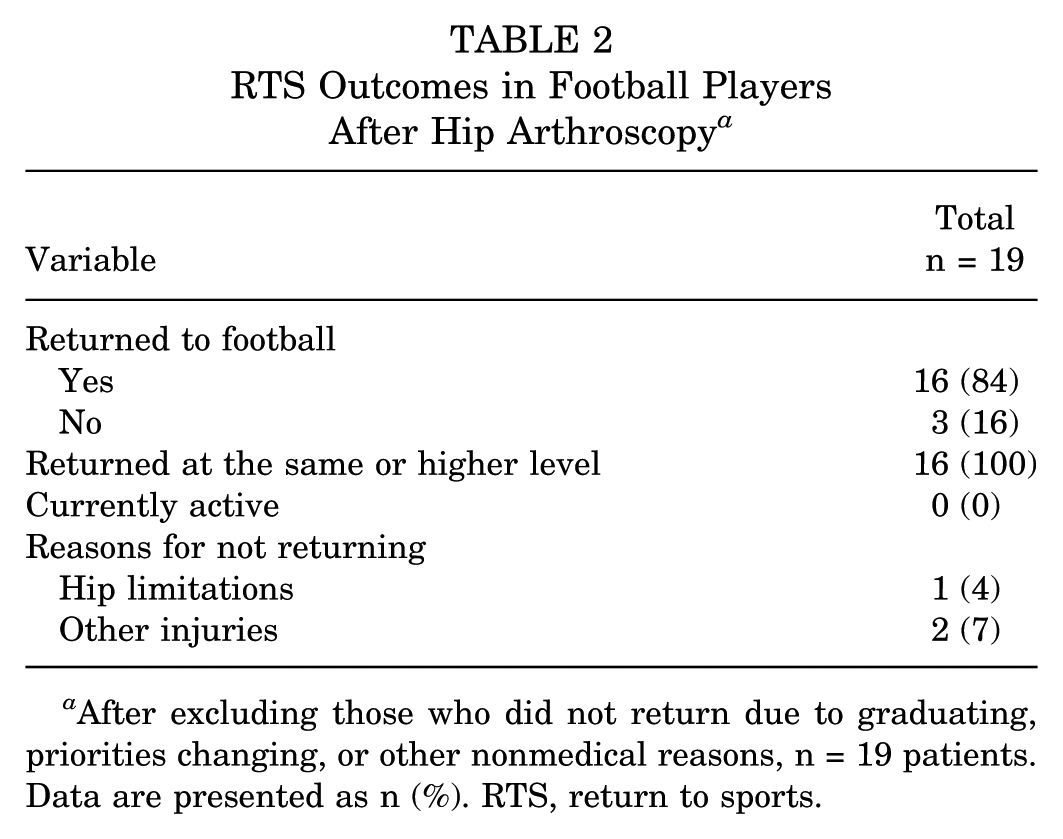
After excluding those who did not return due to graduating, priorities changing, or other nonmedical reasons, n = 19 patients. Data are presented as n (%). RTS, return to sports.

The primary reason for not returning to American football after hip arthroscopy.
Factors Influencing Return
A logistic regression model was used to investigate possible predictors of RTS (Table 3). None of the variables included (eg, BMI, age, level of play, alpha angle, or football position) was found to affect RTS significantly.
Logistic Regression Results for Predictors of Return to Football After Hip Arthroscopy a

Group sample sizes are as follows: BMI <25 kg/m2: n = 9; BMI ≥25 kg/m2: n = 18. Age <20 years: n = 21; ≥20 years: n = 5. Level of play—high school: n = 19; college: n = 7. Alpha angle >60°: n = 17; ≤60°: n = 10. Position—Lineman: n = 13; non-lineman: n = 12. BMI, body mass index; OR, odds ratio.
Patient-Reported Outcomes
At a mean follow-up of 9.8 ± 2.7 years, the mean mHHS was 90.5 ± 11.5 (95% CI, 85–96.1), and the mean HOS-ADL and HOS-Sport were 94.5 ± 7.1 (95% CI, 91.1–97.9) and 91.1 ± 12.1 (95% CI, 85.3–96.9), respectively (Table 4). The mean Tegner activity level was 6.7 ± 2.3 (95% CI, 5.7–7.8). The mean satisfaction with surgery was 8.5 ± 2. Significant improvements were reported in mHHS (68.5 vs 90.5: P < .002), HOS-ADL (73.9 vs 94.5; P < .001), and HOS-Sport (49.7 vs 91.1; P < .001) (Figure 3). All changes exceeded the minimum 5-year follow-up MCID thresholds (14.4 for mHHS, 10.6 for HOS-ADL, and 15.4 for HOS-Sport), indicating clinically meaningful improvement. No significant differences in postoperative PROMs were observed between those athletes who returned to sports and those who did not (Table 5).
Final Follow-up Postoperative PROMs in All Football Players a

Values are presented as mean ± SD or n (%). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-Sport, Hip Outcome Score–Sport Specific Subscale; mHHS, Modified Harris Hip Score; PROM, patient-reported outcome measure; VAS, visual analog scale.

Preoperative versus postoperative outcome scores in football players undergoing primary hip arthroscopy. Data are presented as mean ± 95% CI. The asterisk (*) indicates a statistically significant difference between pre- and postoperative scores (P < .01). HOS-ADL, Hip Outcome Score–Activities of Daily Living; mHHS, Modified Harris Hip Score.
Comparison of Postoperative PROMs Between RTS and Non-RTS Football Players a

Values are presented as mean ± SD or n (%). HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-Sport, Hip Outcome Score–Sport Specific Subscale; mHHS, Modified Harris Hip Score; PROM, patient-reported outcome measure; RTS, return to sports; VAS, visual analog scale.
Complications and Reoperations
No patients required revision arthroscopic FAI correction or labral repair. Two hips (8%) underwent reoperation at 0.7 and 11.1 years postoperatively for the following reasons: one patient underwent heterotopic ossification excision due to symptomatic limitation of hip motion, and another patient underwent unplanned periacetabular osteotomy at 9 months postoperatively for persistent hip pain. There were no complications, and all reoperations were performed with patients experiencing improvement in their symptoms after the procedures.
Discussion
This study aimed to evaluate RTS and PROMs in nonprofessional American football players. A total of 27 male athletes (36 hips) were included, with a mean follow-up of 9.8 ± 2.7 years. In this cohort, 84% of football players who attempted to RTS after hip arthroscopic labral repair were successful, demonstrating improvements in mHHS, HOS-ADL, and HOS-Sport scores and a low reoperation rate at long-term follow-up. Of the 3 athletes who attempted to RTS but could not, only 1 cited hip-related limitations, whereas the other 2 cited other injuries.
Most of the literature on RTS in American football players after primary hip arthroscopy for FAI has focused on NFL players. The largest study reporting on RTS after FAI in NFL players reported a RTS rate of 84.1% in 55 players (63 hips). 29 This is similar to our study, and although their cohort was older (mean age, 27.5 years), the greatest proportion of athletes undergoing arthroscopy were also linemen. 29 Menge et al 18 reported a RTS rate of 87% in their study of 51 NFL players with a mean age of 27 years. Studies 9 of other high-level athletes reported RTS rates of 71.4% (mean age, 27 years) 26 and 93.7% (mean age, 29.1 years). Byrd et al 4 published a RTS rate of 86% in a large cohort of 104 high school athletes with a mean age of 16. This is consistent with the findings of the present study, despite their cohort including 49% female athletes and representing multiple sports, compared with our cohort of 100% male football players. A greater likelihood of positive outcomes after hip arthroscopy for FAI has been reported, with this association correlating with young age and male sex. Although we did not find age to be a predictor of RTS, our overall cohort was young, with a mean age of 18 years.
We observed improved PROMs at a mean 9.8-year follow-up, with increases in mHHS (90.5), HOS-ADL (94.5), and HOS-Sport (91.1) scores compared with preoperative scores. Menge et al 19 also reported significantly improved PROMs, with a mean mHHS of 88, mean HOS-ADL of 92, and mean HOS-Sport (86) at a minimum 10-year follow-up in a large cohort (70 hips) of similarly aged patients (mean age, 16 years) undergoing hip arthroscopy for FAI. However, in their study, a higher proportion of athletes participated in sports such as soccer and dance than in football, and their mean BMI was 21.4 kg/m2, compared with 28.1 kg/m2 in our study. In addition, the majority of our cohort who underwent surgery (12 out of 19) reported feeling much better than before surgery based on the VAS pain 5-point scale. This is similar to other studies, which have shown improvements in VAS after hip arthroscopy for FAI.5,6 Interestingly, there was no difference in PROMs between those who were able to RTS and those who did not, and overall surgery satisfaction was also not statistically different between the groups, highlighting the improved outcomes regardless of ultimate ability to return to competitive American football.
While it has previously been reported that younger age, male sex, and lower BMI were associated with better postoperative outcomes, 30 our analyses did not identify differences in RTS based on BMI, age, level of play, alpha angle, or football position. However, the study may have been underpowered to detect small effect sizes. In addition, labral repair has previously been shown to have better outcomes than debridement alone.15,25 Our cohort comprised entirely of young male players with relatively low BMIs, all undergoing labral repair, which could have certainly played a role in the outcomes achieved.
Finally, 84% of athletes (16/19) who attempted to return to American football succeeded. While the overall RTS rate in our study was 59% (16/27), it is important to note that this includes those who did not return for other reasons unrelated to their FAI. However, of those who did not return, 5 athletes graduated or shifted focus to another sport, 3 reported changing priorities or limited time availability, and 2 reported other injuries that prevented their return. There are just over 1 million high school football players, of whom just over 7% go on to play college football, highlighting the relatively low rate of players who end up playing college football. 21 Several recent psychosocial studies have suggested that changing priorities during the transition from high school to university, such as focusing on academics, lack of time, or preference to play a different sport, are reasons why athletes decide to either not RTS or play at the next level.24,27,35 As there was no significant difference in PROMs between the RTS and non-RTS cohorts, this suggests that PROM improvement does not always equate to RTS and instead highlights contextual factors, such as those stated above. Compared with the cohorts of NFL players, who are elite-level athletes who prioritize a single sport and are all financially compensated by playing, our cohort was comprised of a majority of high school (70%) or college (26%) players. This highlights additional patient-specific priorities to consider when treating this unique population, as factors beyond the desire to continue competing in athletics may influence presurgical counseling for younger patients.
This study is not without limitations. First, this was not a single-surgeon series, which may introduce variability in surgical technique, decision-making, and postoperative rehabilitation protocols. Second, procedures were performed over 9 years, during which significant advancements in hip arthroscopy—including improved capsular management, greater precision in femoral osteoplasty, and rehabilitation protocols—may have influenced outcomes. Third, although follow-up was long-term, the relatively small cohort size and limited variability in patient characteristics may reduce the statistical power to detect differences between subgroups, increasing the possibility of type 2 error. Additionally, attrition due to loss to follow-up (11 of 36 hips; 31%) may limit generalizability and introduce selection bias. Loss to follow-up for PROMs was primarily due to noncompletion of REDCap surveys or inability to contact patients. PROMs were analyzed only for patients with available data, while all patients were included in the RTS analysis using an intention-to-treat approach. Missing data could influence the results if patients lost to follow-up systematically differed in outcomes, potentially leading to over- or underestimation of functional improvements. As such, the findings—particularly those based on subgroup comparisons—should be interpreted with caution.
Conclusion
Hip arthroscopy with labral repair for FAI in non-professional American football players resulted in excellent long-term outcomes, with significant functional improvements, high satisfaction, and a low reoperation rate. Among those who attempted, 84% returned to football at the same or higher level. Nonmedical factors played a key role in RTS decisions, underscoring the need for individualized counseling in younger athletes.
Footnotes
Final revision submitted November 23, 2025; accepted December 20, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.A.L. is a consultant for Arthrex, Inc. B.A.L. is part of the editorial or governing board for the Journal of Knee Surgery, Knee Surgery, Sports Traumatology, Arthroscopy, and Orthopedics Today. M.H. is a consultant for DJO–Enovis, Stryker, Vericel, and Moximed. M.H. receives publishing royalties, financial or material support from Elsevier. M.H. is part of the editorial or governing board for the Journal of Cartilage and Joint Preservation. A.J.K. is a consultant for Arthrex, Inc. A.J.K. is part of the editorial or governing board for the American Journal of Sports Medicine, Association of North America, International Cartilage Repair Society, and Springer. A.J.K. receives research support from Aesculap/B. Braun. K.R.O. is a consultant for Arthrex, Inc and Smith & Nephew.
Ethical approval for this study was obtained from Mayo Clinic IRB (No. 08-002259-17).