
Abstract
Background:
Paralabral cysts are one of the signs of labral injury; however, it remains unclear whether they affect the mid-term clinical outcomes after hip arthroscopy.
Purpose:
To compare the midterm patient-reported outcomes (PROs) of hip arthroscopy for labral tear with or without paralabral cysts, with a minimum follow-up of 5 years.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective matched cohort study was conducted on patients who underwent unilateral hip arthroscopy for labral tear between November 2015 and September 2019. Exclusion criteria comprised nonlabral tear indications, prior hip surgery, incomplete data, or loss to follow-up. Patients with paralabral cysts confirmed by magnetic resonance imaging (MRI) were designated as the cyst group (n = 35), whereas a control group without cysts (n = 35) was selected using 1:1 propensity score matching (PSM) based on sex, age, and body mass index (BMI). Demographic data, radiographic parameters (alpha angle, lateral center edge angle), and PROs, including visual analog scale (VAS), modified Harris Hip Score (mHHS), minimal clinically important difference (MCID), and Patient Acceptable Symptom State (PASS), were analyzed.
Results:
Among 841 eligible cases, paralabral cysts were present in 41 (4.9%) on MRI scan. After 6 cases were excluding because of incomplete data or bilateral surgery, 35 patients (hips) were included in the cyst group. Using 1:1 PSM for age, sex, and BMI, the authors selected an equivalent control group (noncyst group; n = 35), yielding a final cohort of 70 patients (70 hips). No significant differences were found in age (39.2 ± 11.34 vs 39.9 ± 11.92 years; P = .790), sex (70% vs 62.9% female; P = .806), BMI (23.87 ± 3.1 vs 23.60 ± 3.14 kg/m2; P = .711), or symptom duration (22.51 ± 30.37 vs 25.6 ± 25.81 months; P = .635) between the noncyst and cyst groups. Follow-up was significantly longer in the noncyst group (97.03 ± 3.71 vs 78.54 ± 15.84 months; P < .001). Preoperatively, the cyst group had significantly better scores than the noncyst group (VAS, 4.83 ± 1.84 vs 5.94 ± 1.99, P = .018; mHHS, 66.24 ± 15.14 vs 56.51 ± 3.49, P = .046). Postoperatively, both groups improved significantly (all P < .001), with no statistically significant difference in final outcomes between groups (VAS, 1.88 ± 1.82 vs 2.29 ± 2.07, P = .387; mHHS, 89.91 ± 10.42 vs 86.15 ± 16.87, P = .272). Preoperatively, the mean VAS score was 5.39 ± 2.0 (range, 2-10), and the mean mHHS was 61.38 ± 18.62 (range, 12-86). Postoperatively, both groups demonstrated significant improvements in VAS (2.09 ± 1.95; range, 0-7) and mHHS (88.0 ± 14.04; range, 30-100; P < .001). One patient in each group required revision surgery or total hip arthroplasty during follow-up. Overall, 80.0% (56/70) of patients achieved the MCID, and 82.9% (58/70) attained the PASS. Both groups demonstrated comparable success rates for MCID (80.0% vs 80.0%) and PASS (85.7% vs 80.0%; P = .537).
Conclusion:
Paralabral cysts did not adversely affect midterm arthroscopic outcomes, with 80% to 83% of patients achieving clinically significant improvement regardless of cyst status.
The acetabular labrum serves as a critical anatomic structure that maintains hip joint stability and preserves the intra-articular fluid seal. Labral pathology frequently manifests as groin pain and functional impairment. Since Ganz and colleagues’ 3 seminal description of femoroacetabular impingement (FAI) in 2003, substantial clinical research has advanced our understanding of this condition. The aberrant bony morphology characteristic of FAI creates abnormal biomechanical forces during hip motion, subjecting the labrum to either shear stress or direct compression, ultimately leading to tissue injury.
Magnetic resonance imaging (MRI) has emerged as the gold standard noninvasive modality for diagnosing acetabular labral pathology. Beyond direct visualization of labral structural abnormalities, the detection of paralabral cysts serves as a valuable secondary marker of labral injury, analogous to meniscal cysts in the knee or glenoidal labral cysts in the shoulder. 14 Current evidence strongly associates these cysts with underlying labral tears. 11 Emerging research further suggests that hip paralabral cysts may represent early indicators of osteoarthritis (OA), as their presence reflects compromised joint sealing mechanisms and predisposes to abnormal contact forces that accelerate cartilage degeneration.1,2,4 Additionally, these cysts may potentially compress adjacent neurovascular structures, contributing to clinical symptoms. 13
The pathogenesis of paralabral cysts remains incompletely understood, but current evidence implicates repetitive microtrauma as the primary etiological factor for anterosuperior cyst development. 17 The proposed mechanistic cascade involves (1) abnormal hip morphology causing labral tearing, (2) subsequent elevation of intra-articular pressure gradients, and (3) resultant synovial fluid extravasation through labral defects, ultimately accumulating as discrete cystic formations.
Arthroscopic management of paralabral cysts serves dual therapeutic purposes: decompression of neurovascular structures and labral restoration. A 2-year comparative outcomes study demonstrated equivalent clinical efficacy between cyst resection and isolated labral tear repair. 6 Notably, intraoperative findings revealed significantly greater prevalence of acetabular rim chondral delamination in the cyst cohort (P < .05), suggesting that these lesions may represent more advanced joint pathology despite similar short-term outcomes. 2
Although existing literature has established paralabral cysts as potential markers of hip joint degeneration, their impact on medium-term clinical outcomes remains poorly characterized. This study addresses 2 critical knowledge gaps: (1) whether paralabral cysts accelerate OA progression and (2) their prognostic significance after arthroscopic intervention, with particular focus on patient-reported outcomes at minimum 5-year follow-up. We hypothesized that the presence of a paralabral cyst would not affect midterm patient-reported outcomes after hip arthroscopy.
Methods
Inclusion and Exclusion Criteria for Patients
After obtaining institutional review board approval (LM2021193), we performed a retrospective cohort study of consecutive patients who underwent hip arthroscopy between November 2015 and September 2019. Inclusion criteria were (1) patients with positive clinical findings (ie, hip pain or limited range of motion), (2) MRI-confirmed labral pathology, (3) primary unilateral arthroscopy for labral tear, and (4) minimum 60-month follow-up. Exclusion criteria were (1) nonlabral tear indications (including synovial chondromatosis, gluteal muscle contracture, inflammatory synovitis, intra-articular loose bodies, osteoid osteoma, or isolated extra-articular pathology), (2) loss to follow-up, (3) incomplete datasets, (4) bilateral simultaneous procedures, or (5) revision surgeries.
The cyst group comprised patients with MRI-verified paralabral cysts. Through propensity score matching (PSM; 1:1 ratio; caliper = 0.005), we selected matched controls without cysts, balanced for sex, age, and body mass index (BMI). Figure 1 illustrates the cohort selection process. Both groups completed ≥60 months of follow-up.

Flow chart of patient inclusion/exclusion criteria. FAI, femoroacetabular impingement; MRI, magnetic resonance imaging.
Demographic, Radiographic, and Follow-up Data
All patients underwent standardized preoperative 3.0-T MRI examinations of the affected hip to evaluate for intra-articular pathology, with paralabral cysts identified as shown in Figure 2. Two senior radiologists independently reviewed all MRI studies, with consensus required for cyst diagnosis, and excellent interrater reliability was found (intraclass correlation coefficient [ICC] > 0.85). Radiographic evaluation included anteroposterior (AP) pelvis and 45° Dunn view radiographs obtained both preoperatively and postoperatively for bony evaluation. These images were used to measure (1) the lateral center edge angle (LCEA), defined as the angle between a vertical reference line and a line connecting the femoral head center to the lateral acetabular edge on AP views, 16 and (2) the alpha angle, measured between the femoral neck axis and a line from the femoral head center to the point of maximal head-neck asphericity on Dunn views. 15 All radiographic measurements were performed by 2 junior surgeons under the supervision of senior surgeons, with excellent interrater reliability (ICC > 0.80).

Preoperative coronal (left) and sagittal (right) magnetic resonance images representing paralabral cysts in the anterosuperior region.
Clinical outcomes were assessed using validated patient-reported outcome measures (PROMs), including the visual analog scale (VAS) for pain and modified Harris Hip Score (mHHS). We defined clinically meaningful improvement as a minimal clinically important difference (MCID) of ≥½ standard deviation in mHHS (8.2 points), whereas patient satisfaction was determined by achieving a Patient Acceptable Symptom State (PASS) threshold of mHHS ≥74. 5 Preoperative PROMs were extracted from electronic medical records, whereas postoperative assessments were conducted via structured telephone interviews at standardized follow-up intervals by research staff blinded to treatment groups. Additional outcome measures included the incidence of revision arthroscopy or total hip arthroplasty during the follow-up period.
Surgical Procedures
Four senior surgeons performed all procedures using a uniform technique: supine positioning on a traction table with 8- to 10-mm joint distraction. Under fluoroscopy, we established 3 portals (anterolateral, midanterior, proximal midanterior) for 70° arthroscope insertion. After interportal capsulotomy, we sequentially addressed central compartment pathology (labral tears, pincer lesions) and peripheral lesions (cam deformities). Labral treatment (debridement/repair/reconstruction) was tailored intraoperatively. Our surgical philosophy emphasizes cyst decompression and labral preservation as primary objectives. Associated conditions (gluteal injuries, subspine impingement) were treated concurrently. Cartilage status was graded using Outerbridge criteria. 10
Statistical Analysis
Data analysis used SPSS 26.0. After PSM (1:1 ratio; caliper = 0.005), continuous variables were analyzed with t tests and reported as mean ± standard deviation (range). Categorical variables were compared using chi-square and Fisher exact tests and shown as n (%). All tests were 2-tailed with α = .05.
Results
Demographic Data
During the 47-month study period (from November 2015 to September 2019), 922 consecutive hip arthroscopies were performed. After exclusion of 73 nonlabral tear procedures and 8 revision cases, 841 primary labral tear surgeries remained for analysis. Preoperative MRI identified paralabral cysts in 41 cases (4.9%). After exclusion of 5 patients with incomplete data and 1 bilateral case, 35 cyst-positive patients comprised the study group. PSM (1:1 for age, sex, and BMI) yielded 35 matched controls, creating a final cohort of 70 patients. The cohort demonstrated the following mean values: age, 39.6 ± 11.6 years (range, 15-62 years); BMI, 23.7 ± 3.1 kg/m2 (range, 16.9-30.1 kg/m2); symptom duration, 24.1 ± 28.0 months (range, 3-180 months); and follow-up duration, 87.8 ± 14.7 months (range, 60-112 months). Demographic comparison revealed no significant intergroup differences except for longer follow-up in controls (97.0 ± 3.7 vs 78.5 ± 15.8 months; P < .001) (Table 1).
Demographic Characteristics of the Study Population a
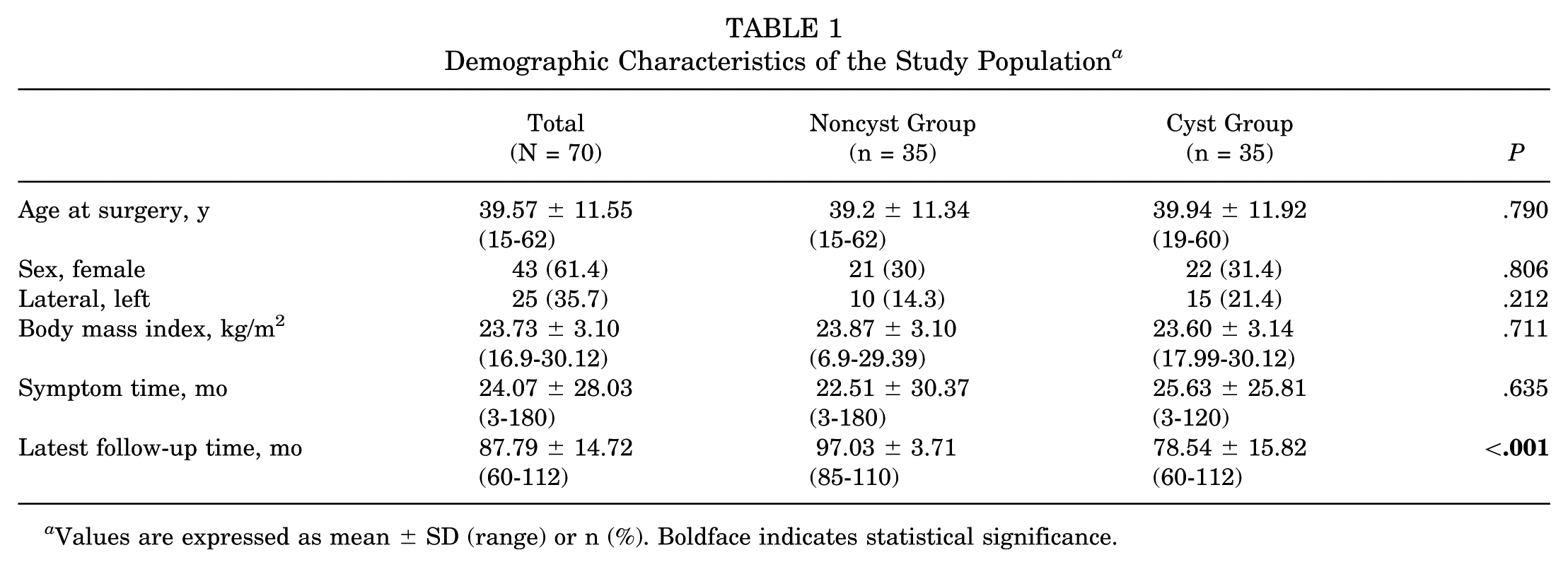
Values are expressed as mean ± SD (range) or n (%). Boldface indicates statistical significance.
Radiographic Characteristics
Radiographic assessment demonstrated significant improvements in both alpha angle (preoperative, 44.6°± 8.2°, range 28.4°-70.0°; postoperative, 37.6°± 5.4°, range 29.4°-59.6°; P < .001) and LCEA (preoperative, 35.2°± 7.6°, range 16.3°-57.9°; postoperative, 33.1°± 6.6°, range 15.2°-50.8°; P < .001). Intergroup comparisons revealed no statistically significant differences in either parameter pre- or postoperatively (all P > .05), indicating comparable bony morphology correction between cyst and noncyst groups (Table 2).
Descriptive Analysis of Radiographic Characteristics a

Values are expressed as mean ± SD (range).
Surgery
The treatment algorithm was stratified by labral integrity: debridement (17.1%) for focal lesions with preserved stability, repair (81.4%) for reconstructible tears, and reconstruction (1.4%) for irreparable damage. Concomitant procedures included femoroacetabular osteoplasty (88.6%), acetabular rim trimming (48.6%), and subspine decompression (2.8%), reflecting our comprehensive approach to addressing both intra- and extra-articular pathology. Intraoperative cartilage assessment revealed distinct injury patterns between compartments. Femoral head cartilage demonstrated predominantly mild involvement (Outerbridge grade 0, 82.9%; grade 1-2, 12.9%; grade 3-4, 4.3%). In contrast, acetabular cartilage showed greater degeneration (grade 0, 52.9%; grade 2, 24.3%; grade 3-4, 22.8%). Comparative analysis demonstrated significantly more severe acetabular cartilage lesions in the noncyst group (P = .033), suggesting a potential protective effect of paralabral cysts against chondral degeneration (Table 3).
Surgical Procedures and Intraoperative Findings a

Values are expressed as n (%). Boldface indicates statistical significance.
Patient-Reported Outcomes
Preoperative assessment revealed baseline VAS pain scores of 5.39 ± 2.0 (range, 2-10) and mHHS of 61.38 ± 18.62 (range, 12-86). Postoperatively, significant improvements were observed in both VAS (2.09 ± 1.95, range, 0-7; P < .001) and mHHS (88.03 ± 14.04, range, 30-100; P < .001). Although the cyst group demonstrated superior preoperative VAS (4.83 ± 1.84 vs 5.94 ± 1.99; P = .018) and mHHS (66.24 ± 15.14 vs 56.51 ± 3.49; P = .046), final follow-up scores showed no intergroup differences (P > .05). One patient in each group required revision surgery or total hip arthroplasty during follow-up. Clinically meaningful improvement (MCID) was achieved by 80.0% of patients overall, with 82.9% reaching PASS thresholds. Both groups demonstrated comparable success rates for MCID (80.0% vs 80.0%) and PASS (85.7% vs 80.0%; P = .537) (Table 4).
Comparison of Patient-Reported Outcomes Before and After Surgery a

Values are expressed as mean ± SD (range) or n (%). Boldface indicates statistical significance.
Discussion
This study establishes a 4.9% prevalence of paralabral cysts among labral tear patients undergoing arthroscopic intervention. Importantly, both cyst and noncyst cohorts demonstrated excellent functional outcomes at minimum 5-year follow-up, with 80% achieving clinically meaningful improvement (MCID) and 83% reaching satisfactory symptom states (PASS). Comparable hip survival rates (97.1%) between groups suggest that paralabral cysts do not adversely affect medium-term surgical prognosis.
Paralabral cysts represent important radiographic indicators of labral pathology, as evidenced by our finding of a 4.9% (41/841) incidence among surgical FAI patients. This prevalence aligns with previous reports, including Lee and colleagues’ 9 identification of cysts in 10.9% (55/506) of FAI cases, with 80% demonstrating associated labral tears, and Magerkurth and colleagues, 12 MRI-based detection rate of 5.7% (40/704). However, similar to labral tears themselves, these cysts may occur in asymptomatic individuals, as demonstrated by Schmitz and colleagues’ 14 observation of paralabral cysts in 26.2% (11/42) of asymptomatic hips. These findings underscore the importance of correlating imaging findings with clinical symptoms when determining treatment strategies for labral cysts.
The relationship between bony morphology and paralabral cyst formation remains controversial. Although Dean et al 2 reported an association between cysts, male sex, and severe cam-type impingement, suggesting a potential link to mechanical overload and joint degeneration, a larger series by Lee et al 9 found no correlation with specific FAI subtypes. Our findings align with the latter, demonstrating no significant differences in alpha angles (44.9°± 7.6° vs 44.2°± 8.8°; P = .70) or LCEA (35.0°± 7.4° vs 35.5°± 8.0°; P = .78) between cyst and noncyst groups. This discrepancy may reflect differing patient selection criteria or cyst pathogenesis mechanisms beyond simple mechanical impingement.
The acetabular labrum plays a critical biomechanical role in maintaining joint stability and fluid seal integrity. Current surgical principles emphasize labral preservation and restoration of its sealing function, with arthroscopic techniques demonstrating consistent efficacy.7,8 Although previous studies have primarily reported short-term outcomes after arthroscopic management of labral cysts, our study provides valuable medium-term follow-up data (mean, 87.8 months). Contrary to traditional views that consider labral cysts as markers of joint degeneration and predictors of poor outcomes, our findings challenge this paradigm. Although Hanke et al 4 initially identified cysts as potential risk factors for surgical failure, subsequent adjusted analyses revealed no significant association. This aligns with Heerey and colleagues’ 6 work showing no correlation between cysts and clinical symptoms in athletes and Dean and colleagues’ 2 demonstration of comparable 2-year outcomes despite more severe intraoperative findings in patients with cysts.
Our medium-term results further support this counterintuitive observation. Both groups achieved similar patient-reported outcomes, with the noncyst group paradoxically demonstrating more severe baseline acetabular cartilage damage (Outerbridge grade 3-4, 25.7% vs 20.0%) and poorer preoperative function (mHHS, 56.5 vs 66.2; P = .046). The comparable revision rates (2.9% overall) and excellent clinical outcomes (80% MCID; 83% PASS attainment) across groups suggest that (1) labral cysts may represent an adaptive response rather than purely degenerative change, (2) the formation of cysts may be a manifestation before potential cartilage degeneration, and (3) timely surgical intervention for symptomatic cysts yields durable outcomes.
These findings support considering arthroscopic treatment when clinical symptoms correlate with imaging findings, as delayed intervention may permit progression to irreversible chondral damage. The protective adaptation hypothesis warrants further investigation through long-term studies and basic science research into cyst pathogenesis.
Limitations
This study has several limitations that warrant consideration. First, despite our use of PSM to enhance comparability, the relatively small sample size (n = 35 per group) may limit the statistical power to detect subtle between-group differences. Larger multicenter studies would strengthen these findings. Second, although our medium-term follow-up (mean 7.3 years) provides valuable data, the extended study period (2015-2019) inherently incorporates evolving surgical techniques and rehabilitation protocols that may influence outcomes. Third, the comprehensive nature of the procedures—addressing concomitant pathologies like abductor tears (27.1%) and advanced cartilage lesions (Outerbridge 3-4, 22.8%)—introduces potential confounding variables that could affect outcome interpretation.
Conclusion
Paralabral cysts occurred in 4.9% of surgical labral tear cases. Importantly, arthroscopic management yielded excellent medium-term outcomes regardless of cyst status, with 80% of patients achieving MCID and 83% reaching PASS. The comparable 5-year survival rates (97.1%) between groups suggested that paralabral cysts did not adversely affect surgical prognosis when appropriately addressed.
Footnotes
Final revision submitted November 10, 2025; accepted December 5, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Natural Science Foundation of China under Grants 82372496, 82272571, and 82372418.
Ethical approval for this study was obtained from Peking University Third Hospital (LM2021193).