
Abstract
Background:
Despite surgical reconstruction, some patients develop persistent residual rotatory laxity following anterior cruciate ligament (ACL) reconstruction (ACLR). Lateral extra-articular tenodesis (LET) has been shown to be a successful adjunctive procedure to address anterolateral instability in high-risk patients with ACL tears. It is often performed during ACLR; however, there is growing interest in understanding possible indications for the LET as an isolated procedure.
Purpose:
To consolidate the current evidence on isolated LET (iLET) following ACLR, explore its indications, and evaluate outcomes such as laxity, patient-reported outcome (PRO) measures (PROMs), and complication rates.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
This systematic review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A comprehensive literature search was performed across Ovid MEDLINE, Embase, EBM Reviews, and Emcare from inception to April 2025. Studies were eligible if they reported outcomes in patients undergoing iLET for residual laxity following ACLR with evidence of an intact ACL graft. Biomechanical, cadaveric, and non-English studies were excluded. Two reviewers independently screened studies, extracted data, and assessed methodological quality. A narrative synthesis was conducted, with descriptive statistics (frequencies, percentages, or weighted means with measures of variability) reported where appropriate.
Results:
Four studies (N = 69 patients, 70 knees) were included, with a mean ± SD patient age of 25.3 ± 2.9) and follow-up period of 26.3 ± 3.6 months. Patients demonstrated significant reductions in rotatory laxity following iLET, with only 6 patients reporting positive postoperative pivot shift (grade ≥1). Reported PROMs improved across all studies. Complication rates ranged from 15.8% to 36.8% while failure rates ranged from 0% to 10.5%.
Conclusion:
This review demonstrated that iLET may provide favorable PROs, reduction in laxity, and low failure rates in patients with residual laxity following ACLR. These findings suggest that the use of iLET may be a viable option for residual laxity following ACLR with evidence of an intact ACL graft; however, a limited number of reporting studies and small sample size require these results to be interpreted with caution.
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACLR) is widely recognized as the gold standard for restoring knee stability after ACL injury. 24 Despite advances in surgical technique and graft placement, a significant subset of patients continue to experience residual rotatory instability, often manifesting as a persistent or high-grade pivot shift.9,12 This residual instability is not only a marker of biomechanical insufficiency, but is also strongly associated with reduced patient satisfaction, functional limitations, and increased risk of graft failure or reinjury. 9
In cases where the graft appears technically intact, yet instability persists, attention has increasingly shifted toward the role of secondary stabilizers such as the anterolateral complex of the knee. 26 Among adjunctive procedures, lateral extra-articular tenodesis (LET), which typically utilizes a strip of the iliotibial band anchored near the lateral femoral epicondyle, has gained renewed interest as an adjunct to ACLR. 4 Biomechanically, LET is designed to resist internal tibial rotation and anterior translation, thereby reducing strain on the intra-articular graft and mitigating residual laxity.17,19
LET has traditionally been considered in primary ACLR for patients at high risk of failure such as those with generalized ligamentous laxity, young age, high-level athletic participation, and high-grade pivot shift. 6 Its application in revision scenarios has garnered attention recently, especially for patients with persistent subjective or objective instability despite an intact ACL graft. 3 In this context, LET serves not merely as a salvage technique, but as a targeted intervention addressing the often-overlooked rotational component of instability.
Despite its theoretical and biomechanical appeal, there remains minimal focused literature evaluating the outcomes of isolated LET (iLET) procedures performed specifically after an ACL graft. While some studies have included LET within broader revision ACLR protocols, few have focused on its outcomes as an isolated intervention in patients with clinical instability but no evident graft failure. 23 This distinction is crucial, as a targeted lateral procedure may restore functional stability in cases where full intra-articular revision is unnecessary or overly invasive.
Given this knowledge gap, a systematic review of the literature is warranted to synthesize current evidence on outcomes of iLET following ACLR when patients present with rotatory instability despite an intact or partially intact ACL graft. The goal of this review is to clarify the clinical rationale for iLET in this specific population by consolidating reported indications, residual laxity outcomes, patient-reported outcome (PRO) measures (PROMs), and complication rates and to determine whether current evidence supports its use as a reliable adjunct or standalone intervention for persistent pivot shift following ACLR. We hypothesized that iLET would be associated with meaningful reductions in residual laxity, improvements in PROs, and low complication rates in patients with persistent instability following ACLR.
Methods
Study Design and Reporting Standards
This systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to ensure transparent and reproducible reporting. 15 The review protocol was developed a priori to guide study design, eligibility criteria, and outcome selection. This review did not require ethics approval, as it involved analysis of previously published literature.
Literature Search Strategy
A comprehensive literature search was conducted across Ovid MEDLINE, Embase, EBM Reviews, and Emcare from database inception to April 14, 2025. The search strategy was developed by the study team using a combination of controlled vocabulary and relevant free-text terms. Keywords included "Lateral Extra-Articular Tenodesis," "LET," "ACL Reconstruction," "Pivot shift," and "Residual Laxity," combined using Boolean operators to maximize sensitivity. The final strategy targeted studies addressing (1) isolated lateral extra-articular procedures, (2) following anterior cruciate ligament reconstruction, for (3) Residual laxity. For example, the Ovid MEDLINE search included the terms "Lateral Extra-Articular Tenodesis" OR "LET" OR "Anterolateral Ligament" OR "Modified Lemaire" AND "Anterior Cruciate Ligament Reconstruction" OR "ACL Reconstruction" OR "ACLR" AND "Pivot Shift" OR "Rotatory Instability" OR "Residual Laxity." Full search strategies for all databases are detailed in Appendix Table S1. Additionally, reference lists of all included studies and relevant systematic reviews were manually screened to identify additional eligible articles not captured in the initial search.
Study Selection
All search results were imported into Covidence systematic review software (Veritas Health Innovation) for deduplication and blinded screening. Two reviewers (O.H., A.D.) independently screened titles and abstracts, followed by full-text reviews to determine final eligibility. Disagreements at either stage were resolved through discussion or adjudication by a third reviewer and senior author (M.D.B.). Reasons for full-text exclusion were documented. Interrater reliability was assessed using the kappa statistic and interpreted as follows: slight agreement (0.00-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and almost perfect agreement (0.81-1.00). 14
Eligibility Criteria
Studies were eligible for inclusion if they met the following criteria: (1) included patients undergoing iLET for excess residual laxity following primary ACLR with an intact or partially intact ACL graft, (2) reported clinical outcomes, and (3) were original research studies including randomized controlled trials, cohort studies, or case series with ≥10 patients. For this review, iLET was defined as LET without concomitant revision ACLR. For the sake of this study, residual laxity was defined using both objective instability and subjective feelings of instability. Studies were excluded if they examined LET combined with revision ACLR, focused exclusively on biomechanical, cadaveric, or radiologic assessments, or were not published in English. Abstract-only publications, conference proceedings, and editorials were excluded unless full-text data could be retrieved.
Data Extraction
Data extraction was independently performed by 2 reviewers (O.H. and M.P.) using a standardized form developed in Microsoft Excel Version 16.90 (Microsoft Corp). Extracted variables included study characteristics (first author, publication year, study design, and level of evidence), patient demographics (age, sex, laterality), surgical details, and duration of follow-up. Reported outcomes included PROMs, residual laxity, reoperation or graft failure rates, and documented complications. Any discrepancies in data extraction were resolved through discussion and consensus with a senior author (D.S.-E.).
Quality Assessment
The review consisted only of nonrandomized studies, which were assessed using the methodological index for non-randomized studies (MINORS) instrument. Two reviewers (A.D. and M.P.) independently scored each study across relevant domains, with maximum scores of 16 for noncomparative studies and 24 for comparative studies. Based on total scores, noncomparative studies were categorized as poor (≤8), moderate (9-14), or high quality (15-16), while comparative studies were graded as poor (≤14), moderate (15-22), or high quality (23-24). 25 Disagreements in scoring were resolved through consensus in consultation with a senior author (P.V.).
Data Synthesis and Analysis
Given the heterogeneity in surgical techniques, outcome measures, and limited sample sizes, a quantitative meta-analysis was not performed. Instead, a narrative synthesis was conducted. Descriptive statistics such as weighted means, ranges, frequencies, and measures of variability were reported where applicable. Tables and figures were used to present synthesized findings across included studies, and all analyses were conducted using Microsoft Excel (Version 16.90).
Results
Search Results and Screening Process
A total of 1031 studies were identified through database searches, including 50 from EBM Reviews, 496 from Embase, 277 from Ovid MEDLINE, and 208 from Emcare (Figure 1; Appendix Table S1). After the removal of 483 duplicates by Covidence, 548 unique articles were screened by 2 independent reviewers (O.H. and A.D.). Agreement at the title and abstract screening stage was fair (κ = 0.28). Of these, 535 articles were excluded by consensus based on irrelevance to the review topic. The remaining 13 full-text articles were assessed for eligibility, with moderate agreement between reviewers (κ = 0.41). Nine studies were excluded at the full-text stage for the following reasons: wrong intervention (n = 5), inappropriate study design (n = 3), and unavailable or non-English full text (n = 1). Wrong intervention referred to studies that evaluated LET procedures with concomitant ACL repair. Inappropriate study design referred to studies that were case series with <10 patients, surveys, or reviews. Manual reference screening yielded no additional studies. A total of 4 studies were included for final analysis (Figure 1).

Study selection flowchart following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for inclusion of studies.
Study Characteristics and Patient Demographics
Four studies comprising 69 patients (70 knees) were included for final analysis (Table 1).2,7,8,20 The mean ± SD age at the time of surgery was 25.3 ± 2.9 years, and 60.0% of patients were male. The mean follow-up was 26.3 ± 3.6 months. The mean time between initial ACLR and the iLET was 23.6 ± 8.0 months. Study designs varied and included 2 prospective case series,2,20 1 retrospective case series, 7 and 1 retrospective cohort study. 8 All studies were published between 2022 and 2025. All 4 studies employed the modified Lemaire technique for iLET.
Study Characteristics and Patient Demographics of Included Studies Reporting Outcomes Following iLET After ACLR a
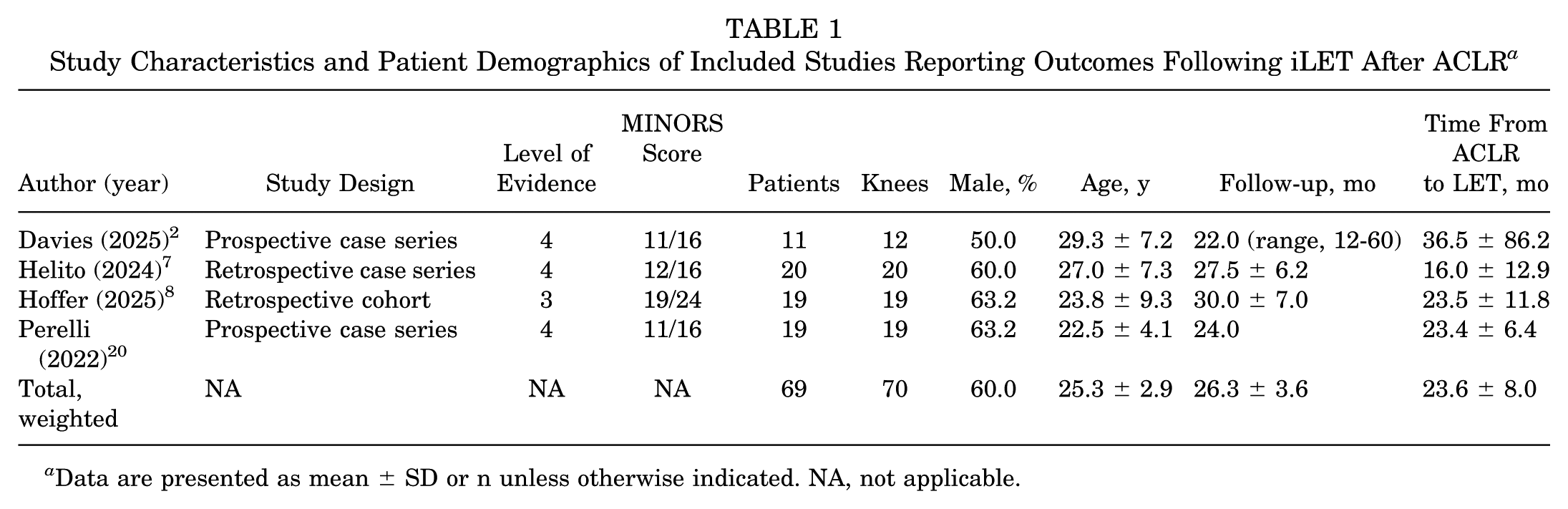
Data are presented as mean ± SD or n unless otherwise indicated. NA, not applicable.
Patient inclusion criteria varied slightly between studies. Davies et al 2 defined knee instability based on a subjective feeling of laxity and excluded patients with a Lachman test or pivot-shift score >3. Helito et al 7 defined instability subjectively and excluded patients with >5 mm of anterior tibial translation or a pivot shift >2. In Hoffer et al, 8 residual laxity was defined as a pivot shift >2, and all patients had sustained concomitant meniscal tears. Finally, Perelli et al 20 included all patients with subjective residual laxity with no limitations on objective clinical findings.
Study Quality
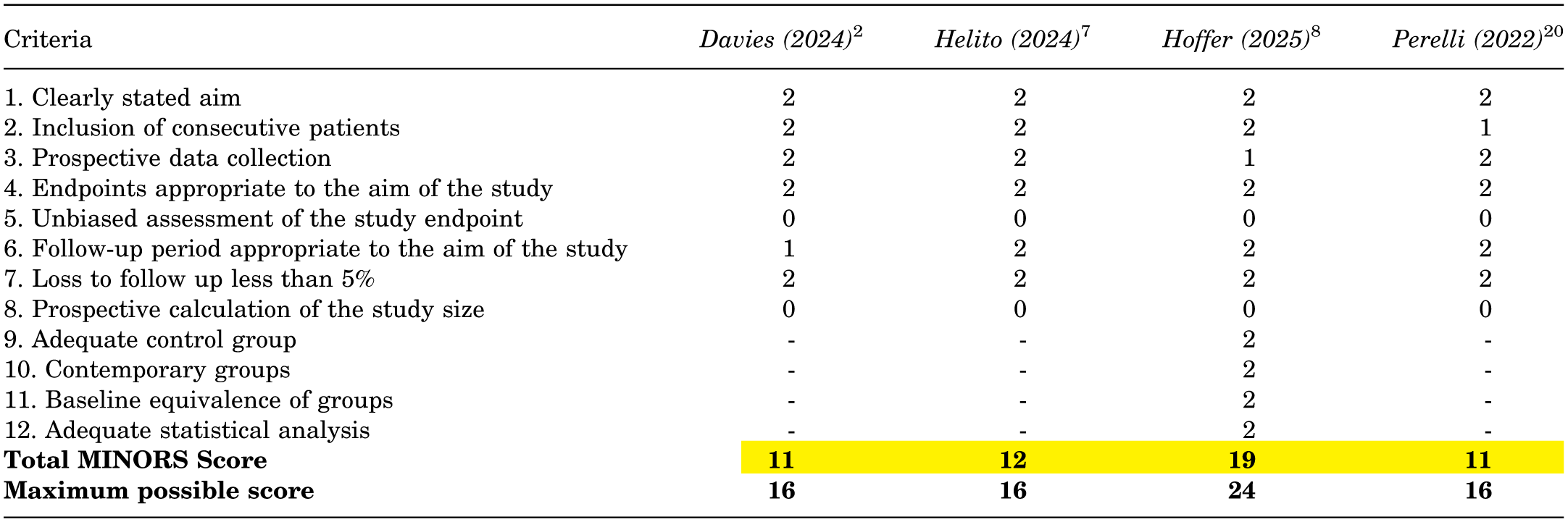
Three studies in this review were noncomparative with MINORS scores of 11, 2 11, 20 and 12, 7 indicating moderate methodological quality (Appendix Table S2). The 1 comparative study had a MINORS score of 19 indicating moderate methodological quality. 8 No studies met the criteria for poor or high quality. Common limitations included absence of prospective calculation of study size and absence of unbiased assessment of study endpoint. Despite these limitations, all studies had clearly stated aims, end points appropriate to the aim of the study, and <5% loss to follow-up.
Residual Laxity
Pivot shift is a clinical finding of residual rotatory laxity that is scored from grade 0 to 3 (0 is normal, 1 is glide, 2 is clunk, and 3 is locked subluxation) with any score >0 being considered high grade. 28 Three studies2,7,8 reported pivot shift as a clinical score while 1 study used a quantitative measure of pivot shift (Table 2). 20 In Davies et al, 2 9 out of 12 knees had a positive pivot shift (≥ grade 1) prior to iLET and no patients had residual pivot shift following the operation. While all other patients included in this review had objective clinical rotatory laxity, 3 patients in Davies et al did not because the inclusion criteria for this study were subjective residual laxity instead of objective instability. In Helito et al, 7 all 20 knees had a positive preoperative pivot shift and 6 knees (30%) had positive postoperative pivot shift. In Hoffer et al, 8 all knees were pivot-shift positive preoperatively and only 2 (10.5%) remained pivot-shift positive postoperatively. In this study, the improvement in pivot shift following iLET was significantly better than in the revision ACLR comparator group (P = .03). 8 All 3 studies that reported qualitative pivot shift found a significant (P < .05) reduction in the number of patients with positive pivot shift postoperatively.2,7,8 Parelli et al 20 reported a quantitative pivot-shift (QPS) value that was measured using a KiRA accelerometer in m/s2. The mean preoperative QPS was 4.7 ± 3.2, which decreased to 2.3 ± 2.5 postoperatively (p = 0.007).
Measures of Rotatory and Anteroposterior Laxity Following iLET After ACLR a

Data are presented as mean ± SD or n (%). ACLR, anterior cruciate ligament reconstruction; AP, anteroposterior; iLET, isolated lateral extra-articular tenodesis; NR, not reported; Postop, postoperative; Preop, preoperative; QPS, quantitative pivot shift (m/s2).
Statistically significant decrease vs isolated revision ACLR comparison group (P = .03).
Two studies7,20 reported objective anteroposterior (AP) tibial laxity using the KT-1000 arthrometer (Table 2). Helito et al 7 had mean AP laxity of 3.0 ± 0.7 mm and 2.0 ± 0.4 mm pre- and postoperatively, respectively. In Perelli et al, 20 these values were 8.3 ± 2.4 and 7.3 ± 1.6. Both studies found the reduction in AP laxity to be significant (P < .05). Davies et al 2 and Hoffer et al 8 did not report postoperative AP laxity.
PRO Measures
PROMs showed overall favorable outcomes across all 4 studies (Table 3). International Knee Documentation Committee subjective knee scores (IKDC-SKS) were reported and showed improvement in all studies. Postoperative scores were >90 in all studies except 1 where the postoperative IKDC-SKS score was 87.6. 7 Three studies reported the P value indicating that this improvement was significant.2,7,20 One study 8 did not report the P value, but the score improved from 52.0 to 91.7. The sole comparative study 8 found that postoperative IKDC-SKS in patients receiving an iLET were significantly better than in patients receiving an isolated revision ACLR (P = .004).
Patient-Reported Outcome Measures Following iLET After ACLR a
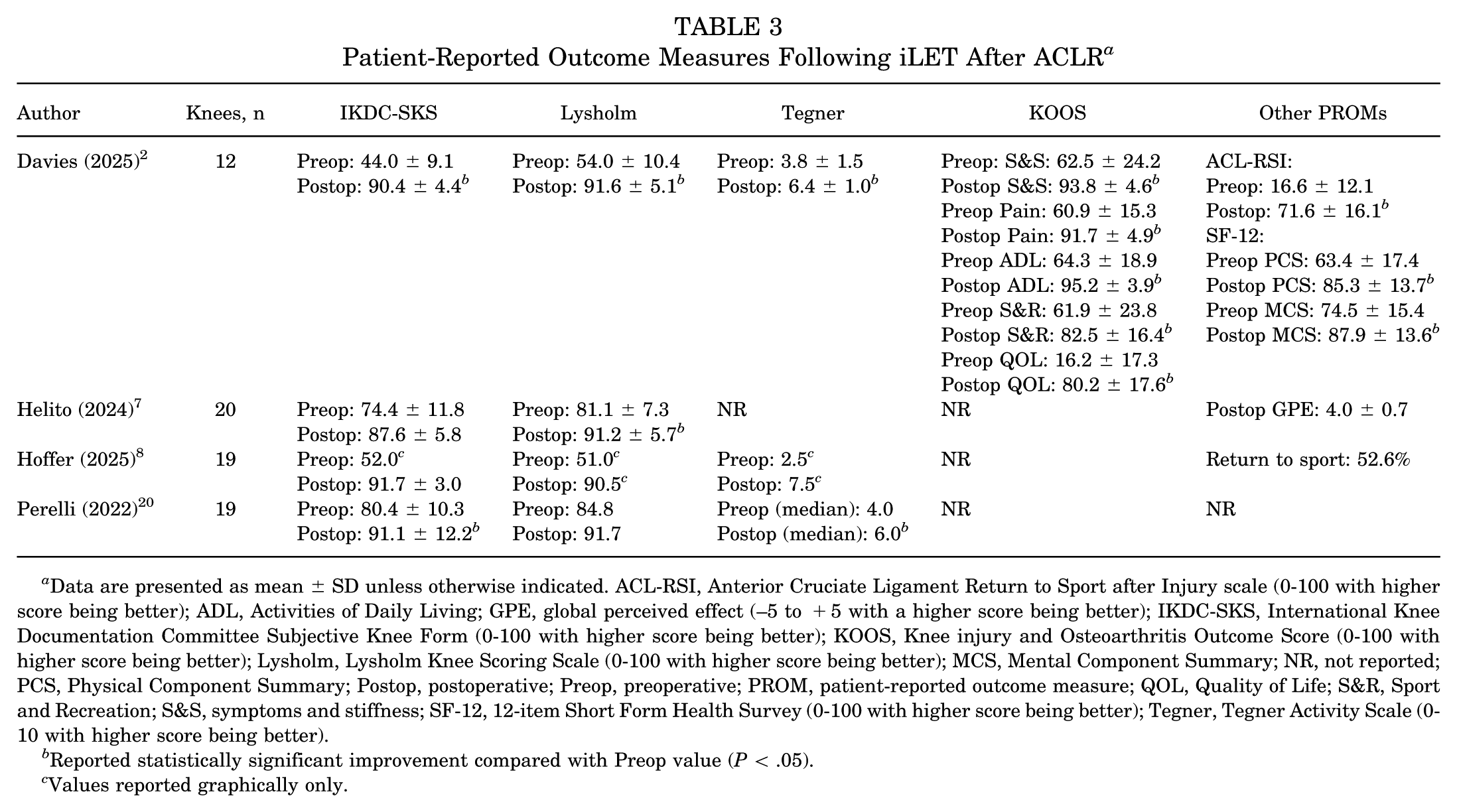
Data are presented as mean ± SD unless otherwise indicated. ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury scale (0-100 with higher score being better); ADL, Activities of Daily Living; GPE, global perceived effect (–5 to +5 with a higher score being better); IKDC-SKS, International Knee Documentation Committee Subjective Knee Form (0-100 with higher score being better); KOOS, Knee injury and Osteoarthritis Outcome Score (0-100 with higher score being better); Lysholm, Lysholm Knee Scoring Scale (0-100 with higher score being better); MCS, Mental Component Summary; NR, not reported; PCS, Physical Component Summary; Postop, postoperative; Preop, preoperative; PROM, patient-reported outcome measure; QOL, Quality of Life; S&R, Sport and Recreation; S&S, symptoms and stiffness; SF-12, 12-item Short Form Health Survey (0-100 with higher score being better); Tegner, Tegner Activity Scale (0-10 with higher score being better).
Reported statistically significant improvement compared with Preop value (P < .05).
Values reported graphically only.
Lysholm scores, similarly, showed improvement across all 4 studies. The mean postoperative Lysholm score was >90 in all studies. This finding was significant in 2 studies,2,7 while 1 study did not report the significance, 8 and the improvement in Lysholm score was not found to be significant in Perelli et al 20 (P = .05). Hoffer et al 8 found no significant difference in Lysholm scores between patients receiving an iLET and isolated revision ACLR.
Tegner activity was reported, and showed improvement, in 3 studies.2,8,20 The mean preoperative Tegner score ranged from 2.5 8 to 4.0, 20 while the mean postoperative scores ranged from 6.0 20 to 7.5 8 . Two studies2,20 reported this improvement as significant while Hoffer et al 8 did not comment on significance. In the sole comparative study, 8 there was no significant difference in postoperative Tegner scores between iLET and isolated revision ACLR.
Additional PROMs were reported in select studies such as the ACL–Return to Sport after Injury scale (ACL-RSI), 12-item Short Form Health Survey (SF-12), and Knee injury and Osteoarthrosis Outcome Score (KOOS), which were reported in Davies et al. 2 All 3 of these PROMs showed significant improvement compared with their preoperative scores. Helito et al 7 reported the global perceived effect scale, which is a single-item score rating the improvement of the patient's symptoms after surgery. The mean postoperative value was 4.0 on a scale from −5 to +5. Hoffer et al 8 reported return-to-sport rates and found that 10 patients (52.6%) returned to sport at 2 years postoperation, and 9 of those 10 patients returned to the same level of sport as before the operation.
Failure and Complication Rates
Table 4 summarizes the complication and failure rates reported in all 4 studies. Total complication rate varied from 15.8% 20 to 36.8% 8 . The most common nonfailure complication was postoperative hematoma, occurring in 4 patients across 2 different studies.7,8 Failure, defined as rerupture of the ACL, occurred in 4 patients across 3 studies.2,8,20 Other complications that were reported include arthrofibrosis (n = 2), painful hardware (n = 2), suture dehiscence (n = 1), superficial infection (n = 1), and subjective continuing instability (n = 1).
Reported Complications Following iLET After ACLR a

Data are presented as n or n (%). ACL, anterior cruciate ligament; ACLR, ACL reconstruction; iLET, isolated lateral extra-articular tenodesis.
In Davies et al, 2 the patient who experienced ACL rerupture was recommended to undergo revision ACLR with the LET procedure because of complete medial meniscal deficiency, but insisted on iLET despite the senior surgeon's recommendation. In Perelli et al, 20 both patients who had ACLR rerupture incurred the injury while participating in sport activities. The 1 incident of suture dehiscence occurred at a posteromedial access point used for a concurrent medial meniscal repair and was unrelated to the anterolateral compartment procedure. 7 The 1 patient who continued to experience subjective instability following the iLET experienced it during sport activity, despite improvements in heavy work activity. 20
Discussion
This systematic review aimed to synthesize the evidence regarding iLET performed for persistent rotatory instability following ACLR with an intact or partially intact primary graft. This current analysis, encompassing 4 studies and 69 patients (70 knees), offers important insights into the efficacy and safety of the iLET following ACLR. The primary findings of this review indicate that iLET has generally favorable outcomes in terms of addressing residual laxity and improving PROMs, with an acceptable failure and complication rate. However, short follow-up durations, limited number of patients, and a limited number of comparative studies necessitate cautious interpretation of these findings.
The primary indication for iLET was residual rotatory laxity, the definition of which varied between studies. Three studies used subjective feelings of clinical laxity2,7,20 while 1 study defined laxity objectively using a pivot shift >2. 8 Interestingly, 2 of the studies that used a subjective feeling of instability as an indication for iLET had limitations on objective clinical findings.2,7 Davies et al 2 excluded patients with a pivot-shift > grade 3, while Hoffer et al 8 excluded patients with a pivot shift >2. These studies thus limited included patients to only those with mild objective clinical instability and excluded patients with significant objective instability. This heterogeneity in inclusion criteria must be considered when evaluating which patients would be good candidates for iLET.
When measuring pivot shift, 3 studies2,7,8 used a clinical maneuver while 1 study 20 used a QPS test.21,28 The preoperative percentage of patients with a positive pivot shift ranged from 75% 2 to 100%7,8 while the postoperative percentage of patients with positive pivot shift ranged from 0% 2 to 30%. 7 One study used a quantitative measurement of pivot shift and found a reduction from a mean pivot shift of 4.7 m/s2 to 2.3 m/s2, indicating an objective improvement in rotatory laxity. 20 In the sole comparative cohort, 8 iLET was significantly more effective than isolated revision ACLR at reducing the number of patients with a positive pivot shift. These findings indicate that iLET can effectively reduce residual rotatory laxity following a primary ACLR, which is important because a positive pivot shift after ACLR is a clinical indicator of failure, because of its association with poorer PROMs, increased progression to osteoarthritis, and graft rerupture.1,10,11
Objective measurement of AP laxity using the KT-1000 arthrometer, reported in 2 studies,7,20 further supports the stabilizing effects of iLET. Both studies demonstrated significant improvement in AP laxity with mean reductions of 1.0 mm. Excessive AP laxity is associated with increased graft failure and decreased PROM scores following ACLR. 16 These findings indicate that iLET may provide AP stability in addition to rotatory stability; however, these findings should be interpreted with caution because of the limited number of reporting studies.
Across all 4 studies, PROMs demonstrated robust gains following iLET. IKDC-SKS improved by 10.7 to 46.4 points surpassing the established minimal clinically important difference (MCID) of 13.8 in 2 of the 4 studies.2,8,18 While 2 studies failed to achieve MCID, the postoperative IKDC-SKS was still quite high with mean values of 87.6 7 and 91.1 20 Thus, the failure to meet the MCID may be due to high preoperative values rather than failure of the iLET. The sole comparative study 8 demonstrated a significantly higher IKDC-SKS in iLET when compared with isolated revision ACLR.
Lysholm scores also showed large improvements across all 4 studies with the mean postoperative score surpassing 90 in all studies. One study failed to reach an established MCID of 9.9, but this was likely due to a very high preoperative score of 84.8.18,20 Tegner scores were reported in all but 1 study 7 and showed mean improvements ranging from 2.0 20 to 5.0. 8 All studies surpassed the established MCID of 0.9, indicating significant functional improvement. 22 This result is particularly promising because of the established importance of Tegner activity scores in younger patients.13,27 Tegner scores are a strong indicator of activity levels and return to sport, important outcomes in younger patients. 13 The sole comparative study 8 found a significant improvement of Lysholm scores in iLET compared with revision ACLR, but found no difference in the Tegner scores between groups postoperatively.
The reporting of other PROMs such as the KOOS, ACL-RSI, and SF-12 was limited to a single study. 2 Regardless, these PROMs followed the same trend of substantial improvement that was seen in Lysholm, Tegner, and IKDC-SKS scores across all studies. However, these findings should be interpreted with significant caution because of the small sample size (n = 12).
Overall complications were reported with relative frequency ranging from 15.8% 20 to 36.8% 8 ; however, objective failure rates were low, ranging from 0% 7 to 10.5%. 20 The most reported complications were relatively mild complications such as hematoma and painful hardware. Dangerous and serious complications such as severe infection, deep vein thrombosis, and nerve palsies were not reported in any studies. Only 1 patient reported a subjective experience of continuing instability following iLET, indicating that most patients were satisfied with the achieved reduction in laxity. Interestingly, this patient only reported instability during sport activities despite reporting increased stability during heavy work activities, indicating possible objective improvement despite the subjective feeling of residual instability. A total of 4 patients experienced ACL rerupture following iLET. However, 1 of those 4 patients was considered a poor candidate for iLET because of a complete medial meniscal deficiency prior to the operation yet the patient proceeded with the operation despite the senior surgeon's recommendation. 8 Interestingly, the studies that excluded patients with severe residual laxity2,8 did not have failure and complication rates that were appreciably different from the failure rates in studies that included patients with higher grade pivot shift,7,20 meaning that higher objective laxity may not be a risk factor for poorer outcomes following iLET, but more data are needed comparing low-grade and high-grade pivot-shift patients receiving iLET. These complication and failure rates are generally comparable with or lower than reported failure rates for revision ACLR.5, 29
Patients evaluated for residual laxity following ACLR with an uncompromised graft pose a difficult clinical decision. Residual laxity is associated with negative outcomes, but revision ACLR may be seen as an overly invasive and unnecessary procedure for patients with an intact graft. 16 This review demonstrates that iLET may be a valuable conservative procedure in this patient population that addresses instability and laxity without altering the primary graft.
Limitations
This systematic review has several limitations that should be acknowledged. First, the included studies were predominantly noncomparative and retrospective with varying levels of methodological rigor based on the MINORS criteria, introducing potential bias and limiting the strength of conclusions. Second, the included studies had small sample sizes, only 69 patients (70 knees), introducing potential bias or reducing generalizability. Third, inclusion criteria and outcome reporting were inconsistent, with different measurements of objective rotatory laxity being used and inconsistent reporting of AP laxity and PROMs. Nonetheless, to our knowledge this is the first systematic review to specifically investigate the outcomes of iLET, and it may provide clinicians with valuable evidence when managing a unique and challenging population of patients with residual ACL laxity.
Future research should focus on prospective, controlled studies with standardized reporting of surgical technique, laxity measures, and clinical assessment. Stratified analyses by patient-specific factors such as primary ACLR graft type, preoperative pivot-shift values, meniscal preservation, and baseline activity level are also needed to better define the indications, outcomes, and risks associated with iLET in the treatment of persistent rotatory laxity following ACLR.
Conclusion
This review demonstrated that iLET may serve as a viable procedure to treat residual rotatory laxity following ACLR with an intact or partially intact primary graft. While studies used differing definitions of laxity, improvement in subjective feelings of residual instability improved across all patient groups. iLET leads to improvement in rotatory and AP laxity, improves PROMs, and has acceptable complication and failure rates. However, several limitations, such as modest sample sizes and heterogeneity in methodological rigor require that these findings be interpreted with caution. High-quality, long-term prospective studies are needed to refine the indications for iLET following ACLR and to better characterize subjective and objective outcomes.
Footnotes
Appendix
Methodological Quality Assessment of Non-Randomized Studies Using the MINORS Instrument.

|
MINORS = Methodological Index for Non-randomized Studies
Final revision submitted November 30, 2025; accepted December 13, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.F.R.H. serves as a consultant for LifeNet, BodyCad, and Arthrex. He also receives royalties from BodyCad. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.