
Abstract
Background:
Depression and anxiety are prevalent among patients undergoing hip arthroscopy. The influence of preoperative depression and anxiety on 2-year patient-reported outcomes (PROs) after hip arthroscopy is not currently known.
Hypothesis/Purpose:
The purpose of this study was to investigate the association between depression and anxiety on PROs after hip arthroscopy. It was hypothesized that worse baseline levels of depression and anxiety, or a clinical history of depression and anxiety, would be associated with worse functional status, pain, and satisfaction 2 years after hip arthroscopy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients undergoing hip arthroscopy for femoroacetabular impingement and/or labral pathologies at a single institution from October 2015 to January 2020 were analyzed retrospectively. Levels of depression and anxiety were measured using the Patient-Reported Outcomes Measurement Information System (PROMIS) Depression and Anxiety domains. Functional status, pain, activity levels, and satisfaction were also measured using PROMIS domains and other PRO measures. Bivariate analysis was conducted to assess associations between preoperative levels of depression and anxiety, as well as 2-year PROs.
Results:
Of the 92 patients identified, 65 (71%) completed follow-up. The mean (SD) baseline PROMIS Depression and Anxiety score was 50.6 (8.3) and 55.4 (8.9), respectively. Worse baseline PROMIS Depression and Anxiety were associated with worse PROMIS Fatigue, Depression, and Anxiety at 2 years but not associated with worse PROMIS Physical Function, Pain Interference, or Social Satisfaction. Unlike the PROMIS measures, a clinical history of depression or anxiety was not associated with PROMIS Fatigue.
Conclusion:
Among patients undergoing hip arthroscopy, worse preoperative mental health is associated with worse mental health outcomes at 2 years. However, preoperative mental health may have no bearing on postoperative functional status or satisfaction.
The recent focus on the role of mental health in orthopaedic surgery patients has highlighted the impact of mental health morbidity on preoperative status and postoperative outcomes.3,34 For instance, the prevalence of psychiatric illness among patients undergoing hip arthroscopy has been reported to be as high as 52%, which is >3 times the prevalence in the general population and greater than the prevalence among other common elective orthopaedic procedures.11,20,35 Among all psychiatric illnesses, the 2 most common are depression and anxiety, accounting for >40% of psychiatric diagnoses in patients undergoing hip arthroscopy. 20 Depression and anxiety have been shown to be associated with an increased number of opioid prescriptions and increased cost of care, both before and after hip arthroscopy. 21 Prior studies have even found mental health to be more closely related to and predictive of preoperative symptoms and postoperative outcomes compared to radiographic or surgical findings.26,30,40 Therefore, understanding the impact of depression and anxiety on outcomes after hip arthroscopy is important in order to appropriately select patients, offer effective preoperative counseling, improve postoperative protocols, and ultimately improve outcomes.
The current evidence on hip arthroscopy and mental health disorders is limited to a small number of studies with a heterogeneity in defining both exposures and outcomes, and it largely focuses on patients with femoroacetabular impingement (FAI) syndrome.8,12,17 Methods for identifying patients with worse preoperative mental health status have included chart review to identify the use of psychotropic medications or a clinical history of depression or anxiety13,37,41 and validated measures of current depression and anxiety symptoms. 31 Few studies have evaluated a clinical mental health history alongside quantitative measurements of mental health, despite recent evidence demonstrating that quantitative measures of baseline depression and anxiety may be more predictive of functional status than clinical history. 26
The purpose of this study was to investigate the association between depression and anxiety on patient-reported outcomes (PROs) after hip arthroscopy at a 2-year follow-up. We analyzed baseline levels of depression and anxiety, as measured by the Patient-Reported Outcomes Measurement Information System (PROMIS), and clinical history of depression and anxiety to assess the impact of both acute and long-term symptom burden on outcomes. We hypothesized that worse baseline levels of depression and anxiety or a clinical history of depression and anxiety would be associated with worse functional status, pain, and satisfaction 2 years following hip arthroscopy.
Methods
We retrospectively analyzed prospectively acquired data from an orthopaedic registry at a single institution. 19 All patients undergoing hip arthroscopy for labral tears and/or FAI between October 2015 and January 2020 were screened in the preoperative areas and clinic for registry enrollment eligibility. Current Procedural Terminology codes included 29862, 29914, 29915, and 29916. Exclusion criteria included (1) age <12 years, (2) incarceration at the time of screening, (3) lack of English literacy, and (4) lack of a functioning email address. After obtaining informed consent and within 1 week of surgery, patients were administered an electronic baseline survey. Follow-up was obtained at 2 years postoperatively by an electronic survey link sent by email or text message. Data were housed in Research Electronic Data Capture at the host institution. 18 Patients were identified for inclusion in the study by procedure codes for FAI osteoplasty and labral repair or debridement. Patients who completed both the baseline and follow-up surveys were included in the final analysis. All study procedures were approved by the local institutional review board.
Sociodemographic variables were self-reported at baseline. The electronic medical record was used as needed to capture relevant demographic data, including the American Society of Anesthesiologists score, insurance, body mass index, and Charlson Comorbidity Index. 25 Arthritis and dysplasia were assessed using preoperative imaging.5,27 Arthritis was defined as Kellgren-Lawrence grade ≥2. Dysplasia was defined as a lateral center-edge angle measurement of <20° on a standardized anterior-posterior pelvis radiograph. PROs were assessed at baseline and 2 years postoperatively. Levels of depression and anxiety were measured using the PROMIS Computer Adaptive Testing (CAT) v1.0–Depression and PROMIS CAT v1.0–Anxiety, respectively. 10 A clinical diagnosis of depression or anxiety was also assessed from chart review. Functional status was measured using PROMIS Physical Function, PROMIS Fatigue, PROMIS Social Satisfaction, Tegner Activity Scale, and Marx Activity Rating Scale (MARS) for the lower extremity.7,33 Pain was measured using PROMIS Pain Interference and a numeric pain scale (NPS).2,24 Satisfaction was measured using the Musculoskeletal Outcomes and Data Evaluation Management System (MODEMS) Met Expectations domain and Surgical Satisfaction Questionnaire (SSQ-8).16,42
PROMIS is a computer-adaptive tool for self-reported health that is efficient to administer and reliable across subspecialties. All PROMIS measures are scored on a scale of 0 to 100, with the population mean set at 50. Higher scores represent increased levels of the variable being measured. Therefore, a higher PROMIS Depression or Anxiety score corresponds to higher levels of depression and anxiety. Since PROMIS measures current levels of depression and anxiety, a clinical history of depression or anxiety was also recorded based on chart review. Change in PROMIS scores was calculated as the difference between the 2-year follow-up and baseline scores.
Categorical variables were reported as frequency and proportion, while continuous variables were reported as means and standard deviation. A goodness-of-fit test was used to assess normality, and most variables failed to meet the normal distribution. Therefore, nonparametric testing was performed. A Wilcoxon rank-sum test and a Kruskal-Wallis test were used to analyze categorical variables with 2 or >2 categories, respectively. Correlations between continuous variables were analyzed using Spearman's coefficient. All tests were 2-tailed, with significance set at P < .05. Statistical analyses were performed with JMP Pro, version 17 software (SAS Institute).
Results
Of the 92 patients identified for the overall cohort, 65 (71%) completed a 2-year follow-up. The median time to follow-up was 25.3 months (IQR, 24-28). The mean (SD) baseline PROMIS Depression score was 50.6 (8.3), and the mean (SD) baseline PROMIS Anxiety score was 55.4 (8.9). Of the patients, 71% and 93% had a diagnosis of FAI or labral tear, respectively. Only 5% of patients had dysplasia, and 12% of patients had mild arthritis. Analysis of demographic variables showed an association between worse PROMIS Depression and greater Charlson Comorbidity Index (ρ = .26, P = .04) (Table 1). Female sex was associated with higher levels of baseline PROMIS Anxiety (female vs male: 56.9 ± 8.2 vs 49.2 ± 9.2, P = .005) (Table 1). Patients without a labral tear had a higher baseline PROMIS Depression score (58.6 ± 4.5 vs 50.1 ± 8.2, P = .03) (Table 1), but not a higher baseline PROMIS Anxiety score. There was no association between sex and baseline PROMIS Depression. A diagnosis of hip dysplasia was associated with higher levels of baseline PROMIS Anxiety (64.2 ± 2.3 vs 54.9 ± 8.4, P = .03) (Table 1) but not baseline PROMIS Depression.
Association Between Baseline Depression and Anxiety and Demographic Variables a

Bold values indicate statistical significance at P < .05. ASA, American Society of Anesthesiologists; BMI, body mass index; FAI, femoroacetabular impingement; KL, Kellgren-Lawrence osteoarthritis score; PROMIS, Patient-Reported Outcomes Measurement Information System.
Results of the bivariate analysis of the 65 patients who underwent hip arthroscopy and completed a 2-year follow-up are displayed in Tables 2 and 3. Higher baseline PROMIS Depression and Anxiety were both associated with higher PROMIS Fatigue, Depression, and Anxiety at 2 years postoperatively (Table 2). Higher baseline PROMIS Depression was associated with worse NPS score for the whole body (ρ = .37, P = .003), while higher baseline PROMIS Anxiety was associated with worse Tegner Activity Scale score (ρ = –.27, P = .04). There were no statistically significant correlations between preoperative PROMIS Depression or Anxiety and any other 2-year PRO measures for functional status, pain, or satisfaction (Table 2).
Association Between Baseline Depression and Anxiety and 2-Year PROs a

Bold values indicate statistical significance at P < .05. MARS, Marx Activity Rating Scale; MODEMS, Musculoskeletal Outcomes Data Evaluation and Management System; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; SSQ-8, Surgical Satisfaction Questionnaire.
Association Between Baseline Depression and Anxiety and Change in PROs a

PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System.
Indicates statistically significant change in PROMIS measure.
In evaluating the 2-year change in PROs, there was a statistically significant improvement in all PROMIS measures relative to baseline, except for PROMIS Depression (Table 3). There was no correlation between baseline PROMIS Depression and Anxiety with the change in any of the PROMIS measures, including the change in PROMIS Depression and Anxiety.
Further analysis investigated the association between a clinical history of depression or anxiety and 2-year outcomes. There were 12 patients (18%) with a clinical history of depression or anxiety. Patients with a clinical history of depression or anxiety did not have statistically significantly higher baseline levels of PROMIS Depression or Anxiety compared to those without (Table 1). At 2 years postoperatively, patients with a history of clinical depression or anxiety had higher PROMIS Depression (54.8 ± 10.7 vs 46.9 ± 9.1, P = .012) and PROMIS Anxiety (57.9 ± 9.3 vs 48.8 ± 9.1, P = .005). Additionally, patients with a history of clinical depression or anxiety had lower postoperative MARS Lower Extremity (18.0 ± 21.7 vs 40.9 ± 31.7, P = .027) (Table 4). Two-year change from baseline in all PROMIS measures was similar between patients with and without a mental health diagnosis (Table 5).
Association Between Clinical History of Depression and Anxiety and 2-Year PROs a
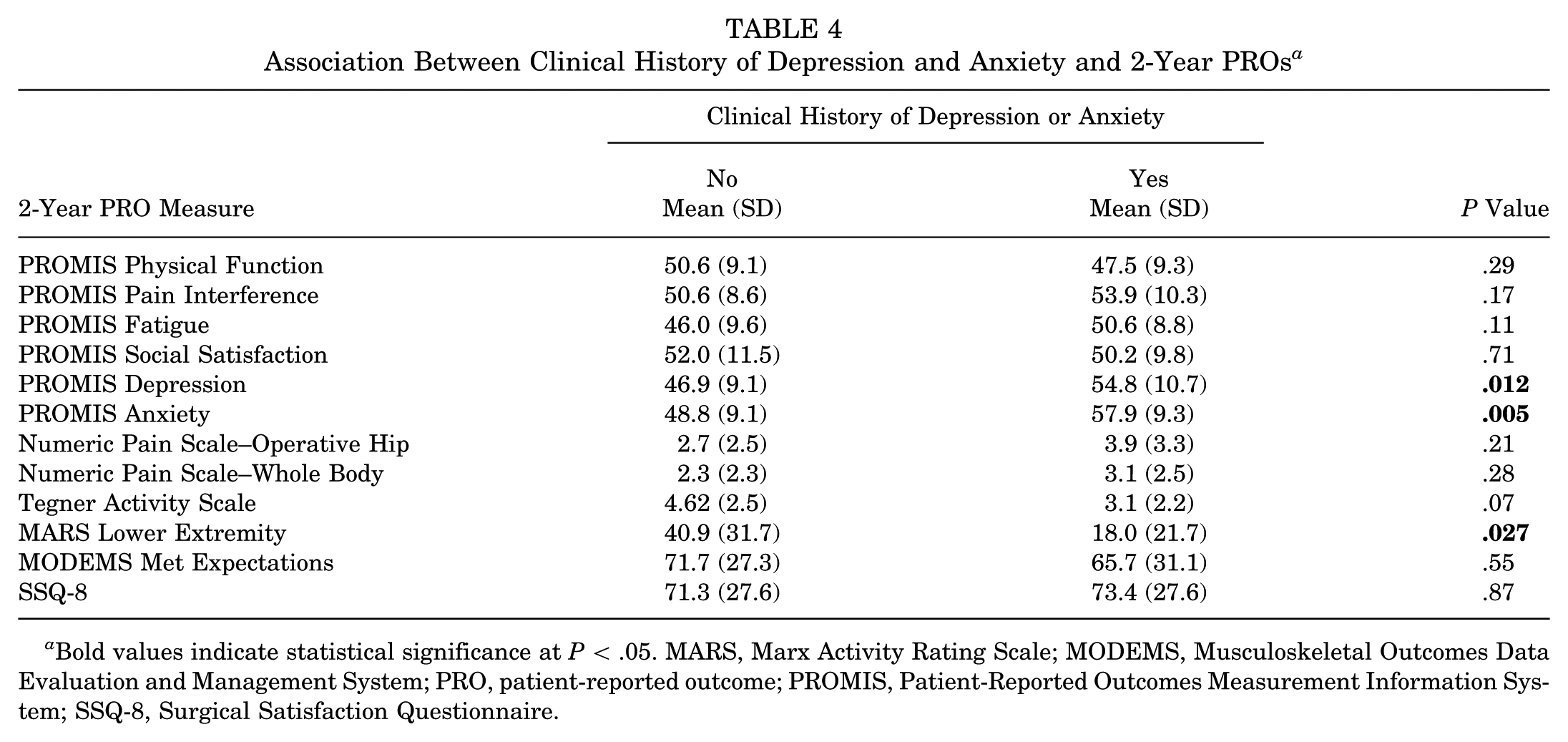
Bold values indicate statistical significance at P < .05. MARS, Marx Activity Rating Scale; MODEMS, Musculoskeletal Outcomes Data Evaluation and Management System; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; SSQ-8, Surgical Satisfaction Questionnaire.
Association Between Clinical History of Depression or Anxiety and Change in PROs a

PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System.
Discussion
The importance of understanding mental health in orthopaedic patients is paramount for improving postoperative outcomes. Patients undergoing hip arthroscopy have a reportedly higher incidence of mental health diagnoses than the average orthopaedic patient, which may have direct effects on postoperative outcomes and overall cost of care. 20 Greater understanding of the impact of depression and anxiety on outcomes in patients undergoing hip arthroscopy may help surgeons appropriately tailor treatment, counseling, and postoperative protocols. In this study, worse baseline PROMIS Depression and Anxiety were associated with worse PROMIS Fatigue, Depression, and Anxiety at 2 years postoperatively. A clinical diagnosis of depression or anxiety was associated with worse 2-year PROMIS Depression and Anxiety. These findings do not confirm our original hypothesis, as baseline PROMIS Depression and Anxiety or a diagnosis of depression and anxiety was not associated with function or satisfaction after hip arthroscopy.
The association between mental health measures and postoperative outcomes in patients undergoing hip arthroscopy has been studied in the literature. A meta-analysis of 9 studies found that patients with poor mental health had worse baseline modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sport-Specific Subscale (HOS-SS), and International Hip Outcome Tool (iHOT-12) scores, in addition to a lower likelihood of achieving a minimal clinically important difference (MCID) in these measures. 17 Similarly, Martin et al 31 found that patients with depression and severe depression, as defined by preoperative Short Form–12 Mental Component Summary (SF-12 MCS) <46.5 and ≤36, respectively, had significantly worse 2-year iHOT-12, visual analog scale, and surgical satisfaction scores after hip arthroscopy. Notably, postoperative SF-12 MCS was not analyzed in this study. Another study using baseline PROMIS Depression and Anxiety scores to assess mental health status observed that higher levels of depression and anxiety were significantly associated with worse iHOT-12, HOS-SS, and HOS-ADL scores at 2 years postoperatively. 36
The current study partially agrees with the literature that shows an association between worse baseline mental health metrics and worse postoperative PROs, as a negative correlation between baseline PROMIS Anxiety and 2-year Tegner Activity Scale was observed. However, there was no correlation or association observed between baseline depression or anxiety and PROMIS Physical Function (PF) or Pain Interference (PI). Although the present study did not include legacy hip-specific outcome measures, PROMIS PF and PI have been consistently validated within the hip preservation population and shown to correlate strongly with commonly used instruments, such as the HOS-ADL, HOS-SS, mHHS, nonarthritic hip score, and iHOT-12 preoperatively and up to 2 years postoperatively.4,6,9,14,22,28,32,39 PROMIS measures also reduce survey burden and demonstrate lower floor and ceiling effects than legacy measures.4,6,14,28,39 Bodendorfer et al 6 found that among 124 patients treated for FAI, PROMIS PF and PI showed good to very good correlations with HOS-ADL, mHHS, HOS-SS, and iHOT-12 one year after hip arthroscopy. Vogel et al 39 reported similar findings among a FAI cohort of 65 patients 2 years after hip arthroscopy. Martin et al 32 evaluated 163 patients treated for FAI, finding that PROMIS PF and PROMIS PI were as accurate as iHOT-12 in determining absolute substantial clinical benefit scores for patient satisfaction 1 year after hip arthroscopy. The absence of significant associations in the present study may reflect nuanced differences in construct measurement between PROMIS domains and legacy hip-specific metrics or demographic and clinical differences between study cohorts. Continued research is warranted to further clarify how baseline mental health influences recovery when measured across different PRO platforms.
Other studies have also investigated the impact of a clinical diagnosis of depression or anxiety on PROs after hip arthroscopy. Kunze et al 29 used a machine learning algorithm to identify predictors of iHOT-12 two years after hip arthroscopy and found that depression/anxiety predicted failing to achieve MCID, significant clinical benefit, and patient acceptable symptom state. Similarly, a recent study by Stone et al 38 identified a history of depression and anxiety as a significant predictor of persistent pain, as measured by the visual analog scale, at 2 years after arthroscopic treatment of FAI. Conversely, a recent study by Johnson et al 23 of 289 patients undergoing hip arthroscopy for FAI did not observe a significant difference in PROMIS PF or Hip Disability Osteoarthritis Outcome Score (HOOS)–Joint Replacement at baseline or 1 year postoperatively between groups with and without a mental health diagnosis. Findings from the current study expand on the 1-year findings reported by Johnson et al, 23 as we found no association between a diagnosis of depression and anxiety and PROMIS PF or PI at the 2-year follow-up. There was also no difference in 2-year change from baseline in all PROs between patients with and without a diagnosis of depression and anxiety. However, there was a correlation between baseline PROMIS Anxiety and 2-year NPS Body.
To our knowledge, this study is one of the few to investigate 2-year mental health outcomes based on baseline health status after hip arthroscopy. Gruskay et al 15 separated a cohort of 566 patients undergoing hip arthroscopy into low mental health (LMH) and high mental health (HMH) groups using an SF-12 MCS cutoff of 46.5. At a mean 4-year follow-up, the LMH group was associated with worse MCS, SF-12 Physical Component Summary, HOS-ADL, and HOS-Sports compared to the HMH group. The current study aligns with these findings, observing significant correlations between baseline PROMIS Depression and Anxiety and 2-year PROMIS Depression and Anxiety. Baseline PROMIS Depression and Anxiety also correlated with worse PROMIS Fatigue—another PROMIS domain that has been linked to psychosocial health in previous literature. 1 The current study also found that a clinical diagnosis of depression and anxiety was associated with worse 2-year PROMIS Depression and Anxiety, demonstrating a consistency between clinically diagnosed and PRO-derived depression and anxiety with regard to 2-year PROMIS mental health outcomes.
Notably, to our knowledge, this study is the first to investigate both baseline and 2-year PRO measures of mental health status and a clinical diagnosis of depression and anxiety in the same study. Lynch et al 30 used the Veterans RAND 12-Item Health Survey–Mental Component Score (VR-12 MCS) to assess mental health preoperatively in the FAI hip arthroscopy cohort. They found that VR-12 MCS was a strong predictor of HOOS-Pain, HOOS–Physical Function, and VR-12 MCS 1 year after surgery; however, clinical diagnoses of depression and anxiety were not included in their analysis. This study expands on these findings, not only observing associations between baseline and 2-year PROMIS Depression and Anxiety but also finding associations between a clinical diagnosis of depression and anxiety and 2-year PROMIS Depression and Anxiety after hip arthroscopy.
This study is not without limitations. First, selection and sample bias may be present, as this is a retrospective study. In this study, legacy hip-specific outcomes scores were not collected or analyzed; however, previous literature has demonstrated a strong correlation between hip-specific outcomes scores and PROMIS measures.9,14 Previous studies have also investigated the relationship between mental health and function at baseline using baseline PROMIS Depression and Anxiety in a cohort of patients undergoing hip arthroscopy. 26 Therefore, the data in this study would be relevant for orthopaedic surgeons in their counseling and discussion with patients. Another limitation is the relatively small sample size of patients who completed the 2-year follow-up; however, the 71% follow-up rate was appropriate and compares favorably to previously published cohort studies. Lastly, the patient population used in this study involves a single urban institution that is a tertiary referral center, and thus, these results may not be generalizable to all other patient populations.
Conclusion
The increased incidence of mental health comorbidities in the hip arthroscopy population when compared to other orthopaedic procedures places a heightened importance on understanding the impact of depression or anxiety on postoperative outcomes in these patients. This study found that preoperative depression and anxiety, whether derived from a clinical diagnosis or preoperative PRO scores, were associated with worse mental health outcomes but not physical function or satisfaction at 2 years postoperatively. Future research should evaluate the impact of preoperative depression and anxiety on postoperative outcomes in larger, prospective cohorts to better characterize this rapidly increasing patient population.
Footnotes
Acknowledgements
The authors thank J. Kathleen Tracy, PhD, Andrew G. Dubina, MD, Julio J. Jauregui, MD, Michael P. Smuda, Vidushan Nadarajah, MD, Ali Aneizi, MD, Patrick M.J. Sajak MD, Tina Zhang MD, Matheus B. Schneider, Evan L. Honig, Joshua M. Abzug, MD, Ngozi M. Akabudike, MD, Farshad Adib, MD, Craig H. Bennett, MD, W. Andrew Eglseder, MD, Mohit N. Gilotra, MD, S. Ashfaq Hasan, MD, Natalie Leong, MD, Christopher G. Langhammer, MD, Vincent Ng, MD, Jonathan D. Packer, MD, Ebrahim Paryavi, MD, Raymond A. Pensy, MD, Cameran I. Burt, Zachary Clark, Shaun H. Medina, Daniel Rivkin, Keyan Shasti, and Alexander J. Wahl for their assistance with data collection.
Final revision submitted December 3, 2025; accepted December 27, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from The James Lawrence Kernan Hospital Endowment Fund, Incorporated (BL1941007WS). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Maryland Institutional Review Board.