
Abstract
Background:
Latarjet is a reliable surgery for shoulder instability, particularly in cases of glenoid bone loss. However, there is a paucity of literature regarding the utility of shoulder arthroscopy with open Latarjet. Prior to Latarjet, shoulder arthroscopy can evaluate the joint and assess for the need for concomitant procedures.
Purpose/Hypothesis:
The purpose of this study was to determine if arthroscopy performed in conjunction with open Latarjet identifies pathology that alters surgical procedures performed. It was hypothesized that arthroscopy would effectively identify additional pathology not seen on magnetic resonance imaging (MRI) requiring surgical management.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review of open Latarjet procedures between 2010 and 2022 was performed. Patients who had a shoulder arthroscopy in conjunction with open Latarjet were identified. Electronic records were reviewed to gather patient and surgical data to determine what pathology was identified and what procedures were performed as part of arthroscopy.
Results:
In total, 307 Latarjet procedures were performed in 293 patients. Arthroscopy in conjunction with Latarjet was performed in 174 cases. Of these, 19 patients (10.9%) underwent diagnostic arthroscopy alone, 155 patients (89.1%) had at least an extensive debridement, and 16 patients (9.2%) had an additional arthroscopic procedure, including loose body removal, superior labrum anterior and posterior (SLAP) repair, biceps tenotomy, SLAP debridement, rotator cuff repair, and remplissage. Arthroscopic evaluation identified anterior glenoid bone loss (100%), torn or diminished anterior labrum (100%), Hill-Sachs lesion (87%), type I SLAP tear/fraying (11.5%), low-grade partial-thickness supraspinatus tear/fraying (9.2%), type II to IV SLAP tear (6.3%), biceps tendon tear (5.2%), and full-thickness supraspinatus tear (1.1%). Of the 16 cases with significant pathology identified that required additional treatment, there were 11 type II to IV SLAP tears requiring debridement, debridement and biceps tenodesis, or SLAP repair; 3 biceps tendon tears requiring biceps tenodesis; and 2 full-thickness supraspinatus tears requiring rotator cuff repair. For patients with a type II to IV SLAP or biceps tendon tear identified arthroscopically, preoperative MRI identified a tear in 10 cases, while 1 patient had a type III SLAP tear not identified on MRI. Both patients requiring a rotator cuff repair had a preoperative MRI that identified the tear.
Conclusion:
Arthroscopy performed with open Latarjet effectively identifies additional pathology and may alter management. Ultimately, 89.1% of this population underwent arthroscopic debridement, while 9.2% had significant pathology identified that required additional procedures.
Shoulder instability is commonly seen in orthopaedic sports medicine, and recurrent anterior instability is typically managed operatively. Operative treatment ranges from arthroscopic labral repair with or without remplissage to bone augmentation procedures such as the Latarjet. Surgical approach is selected based on factors including patient age, activity level, and the extent of glenoid and humeral bone loss. Latarjet is indicated for recurrent anterior shoulder instability with significant glenoid bone loss, off-track Hill-Sachs lesions, or failed prior soft tissue stabilization. 7
The threshold for glenoid bone loss prompting bony augmentation has decreased over time, with recent studies suggesting that a “subcritical” bone loss of 13.5% may warrant consideration for Latarjet. 14 Latarjet has demonstrated excellent long-term outcomes, with lower rates of recurrent instability and superior restoration of stability compared to isolated arthroscopic Bankart repair.3,5,16 A recent study by Rossi et al 12 found Latarjet to be successful in treating anterior glenohumeral instability regardless of the severity of preoperative glenoid bone loss. Despite reliable outcomes, Latarjet remains technically demanding, with complication rates of 15% to 30%, including neurovascular injury, hardware failure, nonunion, and graft osteolysis.1,10,11
Concomitant pathology during the Latarjet procedure most commonly includes associated injuries such as rotator cuff tears, labral pathology, capsular laxity, or sequelae of prior failed stabilization procedures.2,15 While the Latarjet addresses recurrent anterior instability with glenoid bone loss, these additional findings are not uncommon and may influence operative planning. Concomitant procedures performed at the time of Latarjet may involve capsulolabral repair, subscapularis management (split vs takedown), and, less commonly, biceps tenodesis or rotator cuff repair if indicated by intraoperative findings.2,6,9,13 For example, a biceps tenodesis has been described in patients with severe bicipital pain, and modifications such as pectoralis minor repair have been proposed to reduce postoperative scapular dyskinesis without compromising stability. 13 Additionally, intra-articular loose bodies may be difficult to identify or remove through a subscapular split, further underscoring the potential utility of arthroscopy for complete joint evaluation alongside Latarjet. 2
Despite recognition of these associated pathologies, there remains limited high-level evidence regarding their optimal management or long-term impact on outcomes. The incidence of concomitant intra-articular pathology and the extent to which addressing it alters postoperative results are not systematically reported in most Latarjet series. Missing such pathology may contribute to persistent pain or mechanical symptoms. Arthroscopy concurrent with open Latarjet offers the opportunity to identify and treat these lesions as well as provide confirmatory diagnostic visualization that may be valuable for both patient counseling and medical legal documentation.
Although preoperative advanced imaging, such as magnetic resonance imaging (MRI), can identify most pathologies, shoulder arthroscopy performed prior to open Latarjet can provide the gold standard evaluation of the joint and glenoid bone loss prior to proceeding with open Latarjet. In addition, arthroscopy allows evaluation of any concomitant pathology. Despite this, however, arthroscopy is not always performed prior to open Latarjet. While most Latarjet procedures are performed open, surgeons who use arthroscopy at the time of Latarjet will evaluate the joint to debride and treat any unexpected findings. Patients who undergo open Latarjet without arthroscopy, therefore, may have fewer treatment options than those who undergo arthroscopy.
Despite abundant literature on open Latarjet, there is a paucity of studies on the utility of performing shoulder arthroscopy prior to open Latarjet to identify other pathologies that may require concomitant procedures. Ernat et al 8 demonstrated that diagnostic arthroscopy performed immediately prior to open Latarjet identified additional intra-articular pathology not detected by preoperative MRI in 39% of cases and led to additional procedures in 19% of patients. Similarly, Arrigoni et al 2 found that arthroscopy prior to open modified Latarjet revealed associated pathologic lesions in 73% of cases, many of which would not have been optimally discovered or treated during the operative approach alone. Both studies underscore that while open Latarjet is well studied, there is a scarcity of data on arthroscopic evaluation before Latarjet and its impact on surgical management.
The purpose of this study is to determine whether diagnostic shoulder arthroscopy performed in conjunction with an open Latarjet procedure identifies intra-articular pathology that alters the surgical procedures performed. The primary aim is to quantify the number of patients requiring any additional procedures (including debridement) among those undergoing arthroscopy in conjunction with open Latarjet. The secondary aims are to quantify the number of patients requiring additional procedures (not including debridement) and to assess the concordance between preoperative MRI and arthroscopic findings among patients who undergo arthroscopy in conjunction with open Latarjet. It is hypothesized that shoulder arthroscopy will identify pathology not detected on preoperative MRI, potentially altering intraoperative management and improving patient outcomes of surgical treatment.
Methods
Institutional review board approval was obtained before initiation of this study.
A retrospective review of all patients who underwent open Latarjet for recurrent shoulder instability was performed between January 1, 2010, and May 1, 2022, at a large tertiary care institution. The age range of the cohort was 14 to 51 years, with the mean age being 24.1 years. Patients who had a shoulder arthroscopy in conjunction with an open Latarjet were identified, including both primary and revision procedures (61% primary and 39% revision). Bureau of Workers’ Compensation patients were excluded. These data include procedures from 4 surgeons who performed Latarjet. The decision to perform Latarjet and arthroscopy was the surgeon's choice based on bone loss, level of contact sport, and perceived risk of recurrence. Both the operating surgeons as well as radiologists reviewed the MRIs, and results were reported from these reads. Data, which were collected through the institution's electronic medical record system and stored in a secure database, included patient demographics and surgical data to identify the pathology and procedures performed during arthroscopy. Standard operating procedure was to perform a diagnostic shoulder arthroscopy prior to open Latarjet to attempt to identify additional pathology and evaluate the degree of bone loss of the glenoid. The Current Procedural Terminology code 29823 describes “arthroscopic shoulder debridement, extensive,” which involves the removal of devitalized or pathologic tissue from multiple intra-articular structures. Anatomic structures that may be debrided under this code include the rotator cuff, labrum (including superior labrum anterior and posterior [SLAP] tears), synovium, subacromial bursa, and articular cartilage (chondral lesions or flaps). Clinically significant pathology involves rotator cuff tears, labral tears, or chondral lesions with large, unstable chondral flaps. Less significant debridement may include minor synovial fraying or small, stable chondral lesions or minor labral fraying. This study defines significant pathology requiring additional arthroscopic procedures to be type II to IV SLAP tears, biceps tendon tears requiring tenodesis, and full-thickness rotator cuff tears requiring repair. Descriptive statistical analysis was performed to summarize findings.
Results
A total of 307 Latarjet procedures were performed on 293 patients (Figure 1). Of the 293 patients, 249 were male (85.0%) and 44 were female (15.0%). Average age at the time of surgery was 24.1 years. A total of 121 patients had prior surgery: 107 with prior shoulder arthroscopy and 14 with prior open shoulder surgery.
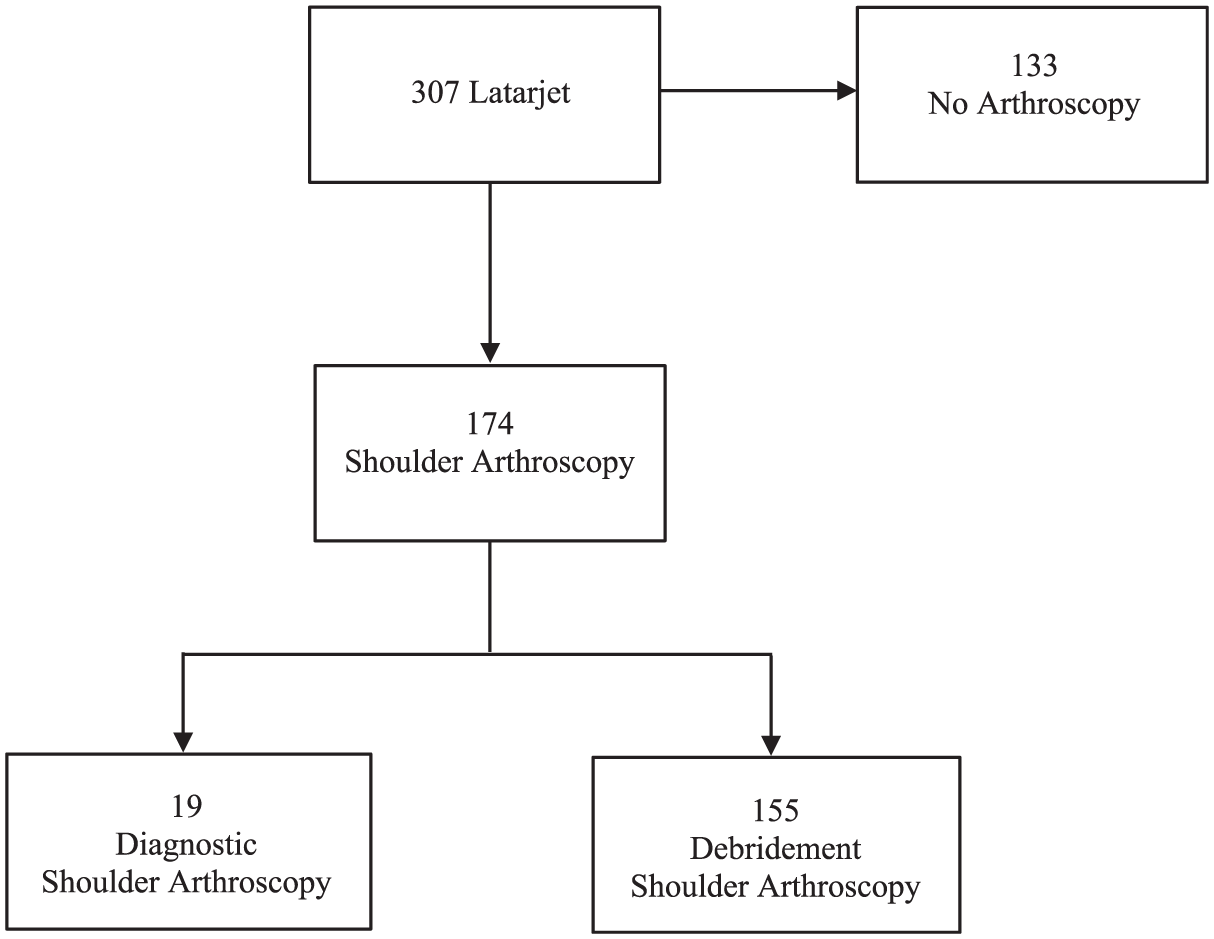
CONSORT (Consolidated Standards of Reporting Trials) diagram. Flowchart showing the patients identified as having open Latarjet during the study period and the breakdown of shoulder arthroscopies performed, further divided by whether the arthroscopy was diagnostic alone or included debridement.
Of the 307 cases, shoulder arthroscopy was performed in 174 cases (56.7%). Of these, 19 (10.9%) cases had a diagnostic shoulder arthroscopy alone performed before proceeding to open Latarjet. In the remaining 155 cases (89.1%), arthroscopic shoulder extensive debridement was performed. Arthroscopic evaluation identified the following pathology: anterior glenoid bone loss (100%), torn or diminished anterior labrum (100%), Hill-Sachs lesion (87%), type I SLAP tear/fraying (11.5%), low-grade partial-thickness supraspinatus tear/fraying (9.2%), type II to IV SLAP tear (6.3%), biceps tendon tear (5.2%), and full-thickness supraspinatus tear (1.1%). Not including debridement, a total of 16 cases (9.2%) at the time of shoulder arthroscopy identified significant pathology that required additional arthroscopic treatment, as defined in the Methods (Figure 2). Eleven of these 16 cases identified type II to IV SLAP tears, of which 4 required debridement alone, 6 required debridement and biceps tenodesis, and 1 required SLAP repair. Three cases had a biceps tendon tear without a SLAP tear requiring biceps tenodesis. In 2 cases, there was a full-thickness supraspinatus tear requiring rotator cuff repair. All additional pathology that was identified was addressed in the same setting and not at a later date.

Flow diagram of patients with significant pathology at the time of arthroscopy. Flowchart showing the breakdown of the cases that had significant pathology at the time of shoulder arthroscopy prior to open Latarjet and the subsequent additional arthroscopic procedures required. SLAP, superior labrum anterior and posterior.
For the 14 cases in which a type II to IV SLAP or biceps tendon tear was identified during shoulder arthroscopy, preoperative MRI was performed in 8 cases. In 7 of those 8 cases (87.5%), the MRI successfully identified the tear. In the 1 case in which the MRI did not identify a tear, the patient had a type III SLAP tear. In the 2 cases of full-thickness supraspinatus tear requiring rotator cuff repair, a preoperative MRI was obtained, which identified the full-thickness tear.
Discussion
This study demonstrated that among patients undergoing arthroscopy at the time of open Latarjet, most required an additional procedure, including extensive debridement (89.1%) that would not have otherwise been performed with a Latarjet alone. Additionally, excluding extensive debridements, an additional arthroscopic procedure was required in 9.2% of cases. Among patients requiring additional arthroscopic procedures who had a preoperative MRI, the MRI identified pathology in only 1 case (0.5%).
Ernat et al 8 found that 19% of patients who underwent arthroscopy prior to Latarjet had additional “critical” procedures performed as a result of findings not identified on MRI. The study by Ernat et al 8 did not include extensive debridement as an additional “critical” procedure, and as such, these data are in stark contrast to this study, which demonstrates an additional, nonextensive debridement procedure not identified on preoperative MRI in 0.5%. However, this study expands on the study by Ernat et al 8 with more cases (307 vs 154) and differs with a younger patient population (24 years vs 28 years), a greater proportion of male patients (85% vs 75%), and a greater percentage of primary Latarjet (61% vs 38%) compared to revision Latarjet (39% vs 62%).
The Current Procedural Terminology code 29823 was developed to reflect that intra-articular structures in the shoulder often require debridement to relieve pain or mechanical symptoms. As such, extensive debridement during arthroscopy represents a therapeutic intervention that provides clinical benefit, rather than a routine or incidental finding. In this context, the high rate of debridement observed in this study (89.1%) underscores the potential value of concomitant arthroscopy, as many of these debridements would not have been performed with an open Latarjet alone.
This study adds to the literature by quantifying the number of patients who underwent additional arthroscopic procedures at the time of open Latarjet. While MRI appears effective at identifying significant intra-articular pathology, this is not always performed preoperatively. Shoulder arthroscopy may also provide additional detail if a patient has had further instability episodes between the time of preoperative MRI and surgery or for soft tissue and bony structural evaluation for patients undergoing Latarjet without a preoperative MRI. Many patients have a preoperative computed tomography scan with 3-dimensional reconstructions to meet the gold standard for bone loss evaluation. 4 The diagnostic arthroscopy then provides complementary evaluation of the soft tissue structures without requiring 2 separate preoperative advanced imaging studies. In our opinion, diagnostic shoulder arthroscopy prior to open Latarjet can add benefit in a variety of ways, including identifying additional pathology that was not identified on a preoperative MRI, treating pathology that was identified on a preoperative MRI, and allowing for the evaluation of soft tissue structures for patients who did not obtain a preoperative MRI.
There are limitations to this study. First, as this study is a retrospective review, results are limited by review and the accuracy of the documentation from the operative reports. Second, not all patients underwent an MRI scan prior to surgery, which may have affected the ratio at which concomitant pathology was identified preoperatively in comparison to that seen during arthroscopy. Additionally, this study lacks objective and subjective patient outcomes; thus, while this study has identified that additional arthroscopic procedures may be required at the time of Latarjet, the ultimate clinical significance and benefit to the patient are not clearly defined. Ultimately, most findings are likely incidental, and addressing them may or may not have any long-term impact on outcomes. This study does not suggest that arthroscopy is a necessity or a standard of care but rather emphasizes that proceeding with it should be left up to the surgeon. Another limitation of this study is that there is no determination of the exact time interval between preoperative MRI and surgery. In clinical practice, there is often a substantial delay between imaging and preoperative intervention, during which additional instability episodes may occur that could alter intra-articular pathology. Perhaps this temporal gap could explain discrepancies between MRI findings and arthroscopic observations at the time of surgery. Consequently, a longer interval between MRI and surgery may increase the likelihood of unrecognized pathology, which further supports the consideration of arthroscopy at the time of Latarjet to ensure evolving pathology is not missed. Future studies should collect outcome variables and compare the cohort that received arthroscopy with a cohort that did not undergo arthroscopy.
In conclusion, arthroscopy performed in conjunction with open Latarjet is an effective tool in identifying intra-articular pathology and may alter surgical management. Ultimately, 89% of this population underwent arthroscopic debridement, while 9% had additional critical pathology identified requiring additional procedures. Although this study did not find arthroscopy to make a significant difference in a high number of patients, improving the outcome of 1 patient makes the use of arthroscopy worthwhile to consider. As such, the authors recommend strong consideration of performing arthroscopy prior to open Latarjet if a preoperative MRI is not obtained or if a preoperative MRI identifies additional intra-articular pathology.
Footnotes
Acknowledgements
The authors acknowledge The Ohio State Sports Medicine Research Institute.
Final revision submitted October 14, 2025; accepted October 23, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The Ohio State University Institutional Review Board (IRB).