Abstract
Objectives:
Lateral extra-articular tenodesis (LET) augmentation utilizing iliotibial band (ITB) autograft has been reported to reduce rotational laxity and reduce failure rates after both primary and revision anterior cruciate ligament reconstruction (ACL-R). Consequently, the utilization of lateral extra-articular tenodesis (LET) augmentation for anterior cruciate ligament reconstruction (ACL-R) has increased. Various fixation points have been recommended based on tactile and anatomic landmarks, however there is limited reporting of the accuracy or precision of these techniques in clinical practice. The purpose of this study was to evaluate whether LET fixation points identified using anatomic landmarks and tactile techniques would fall within a pre-defined radiographic zone. It was hypothesized that the majority of LET fixation points would be inside the radiographic zone.
Methods:
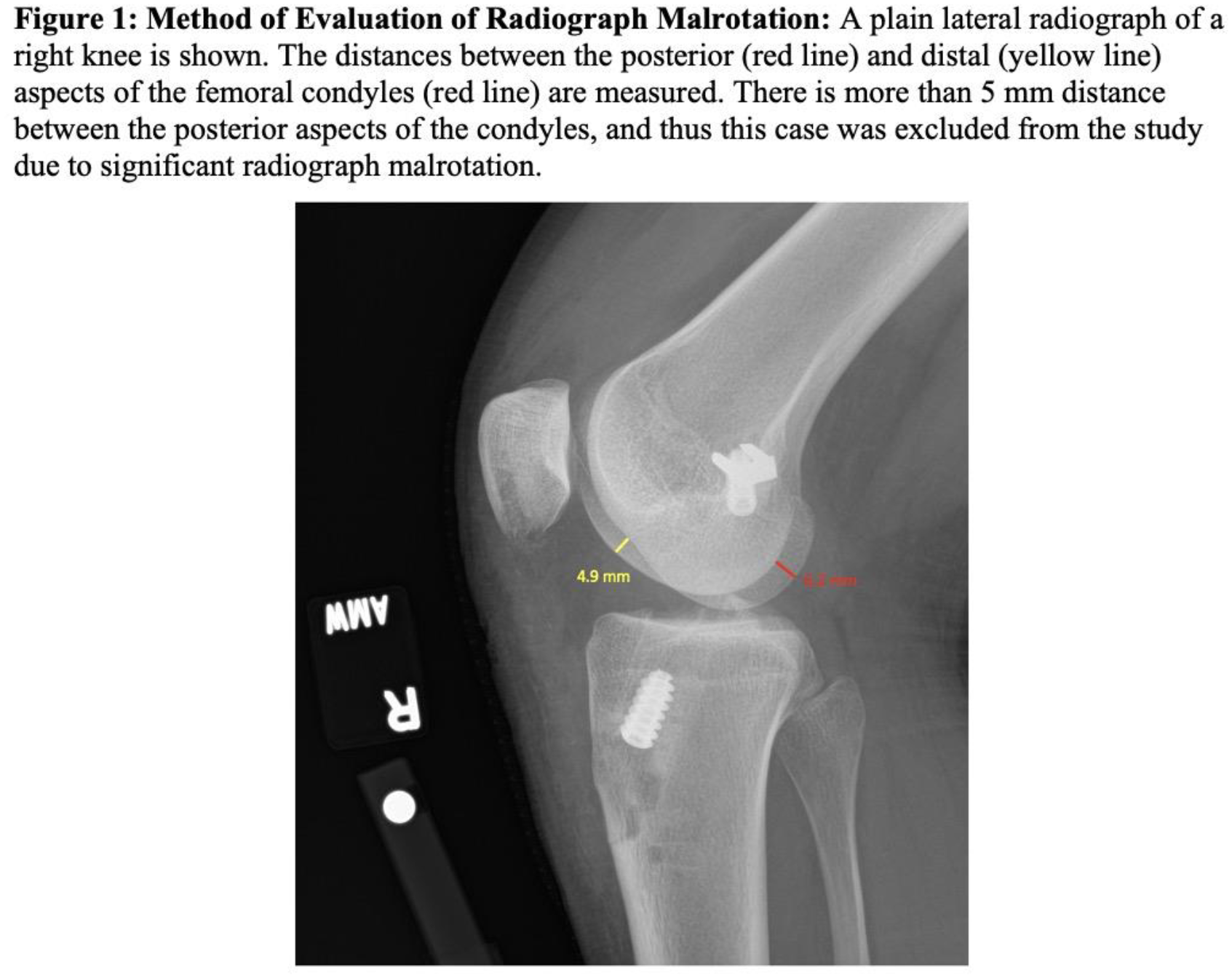
Post-operative plain lateral knee radiographs of patients who underwent ACL-R with concomitant LET from January 2018 to September 2023 by three sports medicine fellowship-trained senior orthopaedic surgeons at a single institution were reviewed. In all cases, the LET femoral fixation point was identified by palpation and identification of anatomic landmarks, and fluoroscopy was not used. Patients were excluded if they underwent additional posterior cruciate ligament, medial collateral ligament, or posterolateral corner reconstruction, if they were skeletally immature, if tunnel position could not be identified, and if there were no post-operative radiographs or no acceptable radiographs, defined as <5 mm distance between the posterior and distal aspects of the medial and lateral femoral condyles (
Results:
One hundred and three patients with 105 knees were identified as having undergone LET and ACL-R. After all inclusion and exclusion criteria were applied, 47 knees in 46 patients with mean age 29.3 +/- 12.9 years were included in the final analysis. Thirty-nine patients were excluded due to malrotated radiographs, fourteen were excluded due to the tunnel position being unable to be identified on radiographs, three were excluded due to lack of post-operative radiographs, and two were excluded due to skeletal immaturity. There were no differences in demographics or injury characteristics between included and excluded patients including age, sex, BMI, laterality, and incidence of meniscal pathology. Demographics for the cohort are shown in
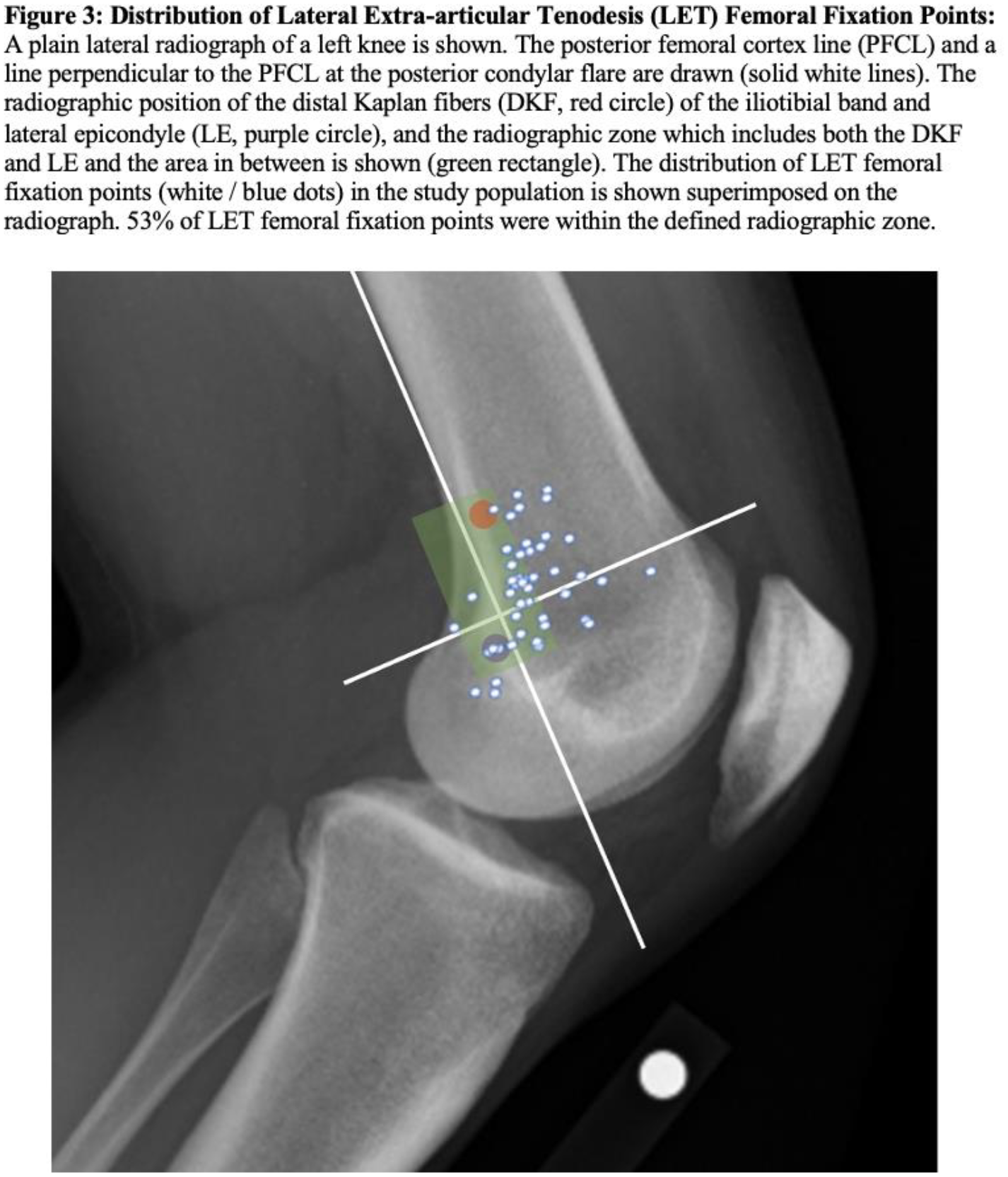
All data is reported as a mean +/- standard deviation (range) unless otherwise noted. The mean LET position was 6.4 ±7.1 mm (-9 to 27.3 mm) anterior to the PFCL and 1.8 ± 7.6 mm (-16.7 to 12.6 mm) proximal to the PCF. 53% of LET fixation points were within the pre-defined radiographic zone. Of the malpositioned tunnels (n=22), their location relative to the radiographic zone was: anterior (n=18), posterior (n=2), proximal (n=1), anterior and distal (n=1). The distribution of LET fixation points is shown in
Conclusions:
This study found high variation in the location of LET fixation points, and half of fixation points were outside the pre-defined radiographic zone. This study provides valuable insight into where LET femoral tunnels are being placed in clinical practice over a five-year period at a high-volume tertiary-referral sports medicine center. These findings suggest that surgeons should utilize intra-operative fluoroscopy during LET to ensure accuracy and precision. This is important to minimize the risk of lateral compartment over-constraint, ACL graft failure, and anisometry leading to LET graft loosening. It is important to note that the results of this study do not detract from the prior demonstrated benefits of LET, nor do they define the desired LET fixation point. Rather, these data should raise awareness for the wide variability in LET femoral fixation location and the need to refine LET techniques and define the ideal position to optimize the proven benefits of LET augmentation during ACL-R.