Abstract
Objectives:
The remnant anterior cruciate ligament (ACL) ligament contains a wealth of vascular blood supply and proprioceptive nerve fibers. Previous literature has suggested that preservation of this remnant may promote graft healing and stability, as well as improved knee proprioception. The ACL-Hybrid Remnant Preservation Reconstruction (HRPR) technique involves preserving and tensioning the tibial remnant in combination with a traditional ACL reconstruction. The purpose of this study was to assess if ACL-HRPR leads to improved patient-reported outcomes and if the technique can be performed safely without increased complications compared to traditional ACLR.
Methods:
A prospective randomized controlled trial was performed to include patients undergoing primary ACL reconstruction +/- HRPR by a single surgeon from 2022-2023. Exclusion criteria included patients <14 years old, multi-ligamentous knee injury, date of injury >6 months prior to presentation, and revision ACLR. Preoperatively, patients were randomized to receive either ACL-HRPR or traditional ACLR with bone patellar tendon bone (BTB) or hamstring tendon autograft. If randomized for HRPR, the surgeon decided intraoperatively if the tibial remnant was amenable for preservation/repair. The primary outcome was Patient-Reported Outcome Measurement Information System (PROMIS)-Physical Function scores, which requires 50 patients per group to achieve 80% power. Secondary outcomes included range of motion (ROM), knee stability via KT-1000 measurements, timed hop testing, and complications. Patients who have completed 6-month follow-up were included for analysis.
Results:
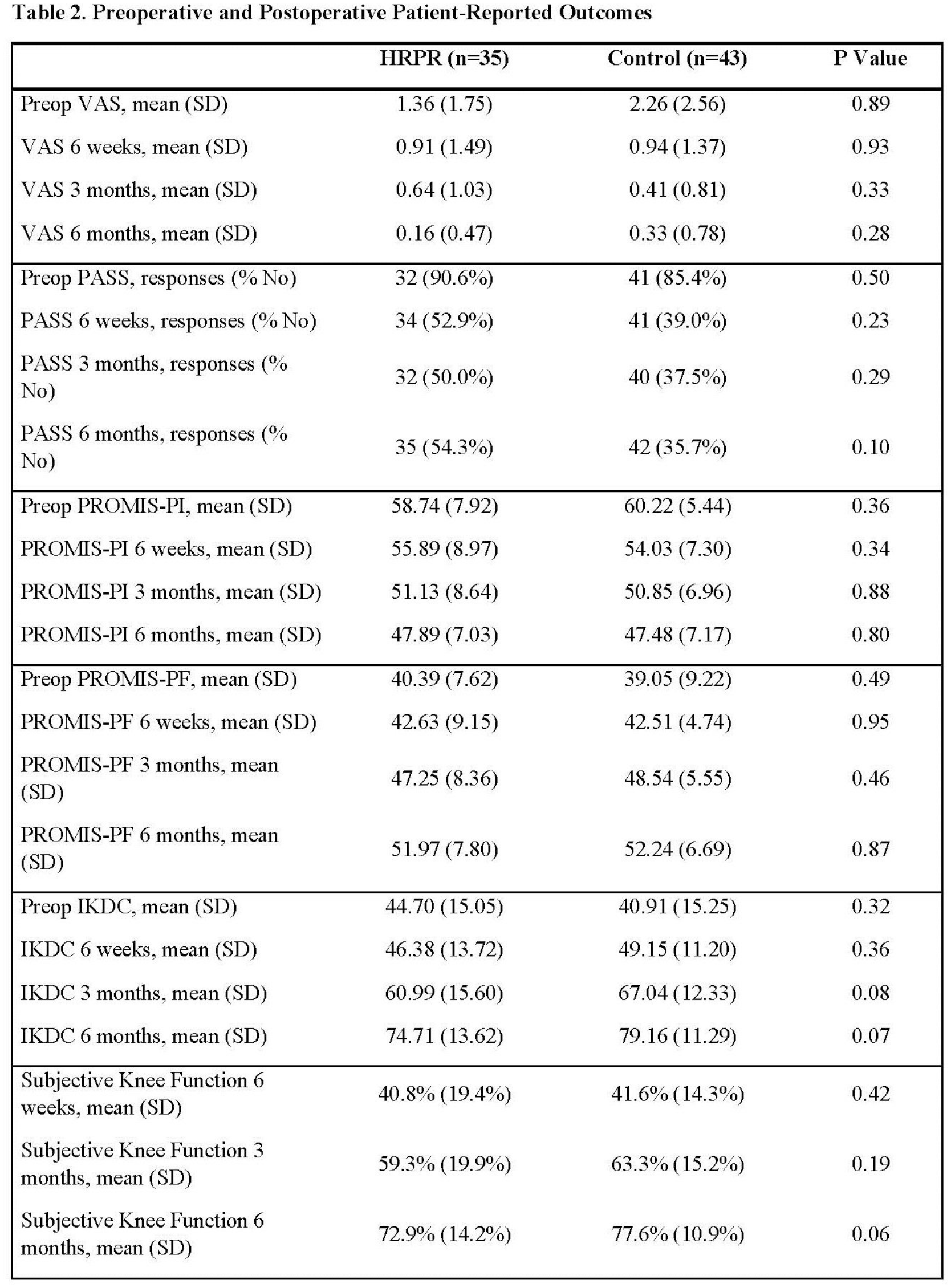
Seventy-eight patients were eligible for analysis, with 35 undergoing HRPR and 43 controls. No demographic differences were observed. After 6 months, patients demonstrated equivalent PROMIS-PF, -PI, International Knee Documentation Committee (IKDC), VAS pain scores, and percent achieving Patient Acceptable Symptom State (PASS). The HRPR group reported significantly increased ROM at 6 months compared to controls (138.7± 7.79 vs 134.52 ± 9.8, p=0.04), with no loss of terminal extension. No differences were observed in return to running time (HRPR 20.22 ± 12.25 vs. Control 19.81 ± 10.34 weeks, p-0.09) Complications rates were similar between groups, as well (5.7% HRPR vs 4.7% controls, p=0.83).
Conclusions:
After 6 months, ACL-HRPR achieves equivalent patient-reported outcomes, knee stability, and return to play testing parameters without increased complications compared to traditional ACL reconstruction.