Abstract
Objectives:
Lateral extra-articular tenodesis (LET) typically involves surgical fixation of a portion of the iliotibial band to improve rotational stability of anterior cruciate ligament reconstruction (ACLR). LET procedures can reduce strain on the ACL autograft by decreasing excessive tibial translation and rotation and have been shown to reduce re-rupture rates in high level athletes. Altered loading to the ACL autograft could, in turn, influence autograft collagen organization and vascularization, a process known as ligamentization. Currently, there exists a gap in knowledge regarding the potential effects of LET procedures on ACL autograft ligamentization. Therefore, the purpose of this study was to determine the effect of LET on autograft maturation during the process of ligamentization based on signal intensity (SI) ratio derived from magnetic resonance imaging (MRI) at timepoints throughout the first post-operative year. We hypothesized that LET would not alter SI ratio relative to non-LET indicating no change in autograft maturation following isolated ACLR.
Methods:
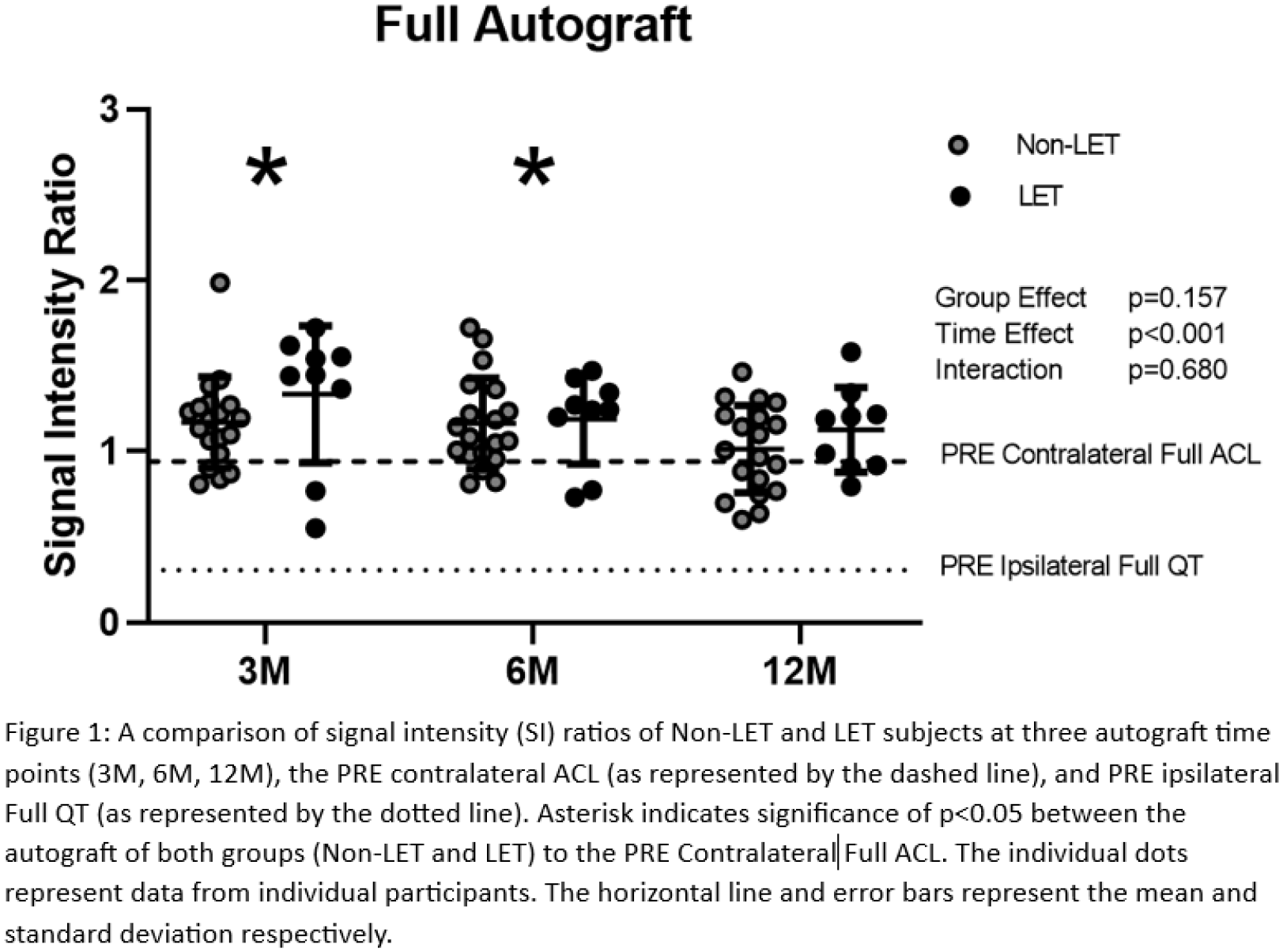
From a prospective longitudinal cohort, 28 young athletes were identified who underwent isolated quadriceps tendon (QT) ACLR (Non-LET; N=19) or QT ACL with LET (LET; n=9) with knee MRI at four timepoints: Pre-surgery (PRE), 3 months post-operative (3M), 6 months post-operative (6M), and 12 months post-operative (12M). From the MRI-derived data, SI ratio was calculated from the following regions: PRE contralateral ACL; PRE ipsilateral QT; 3M, 6M, and 12M autograft. SI ratio was calculated by normalizing to the PCL using the following equation at the full autograft level as well as segmented into 4 sub-segments for analysis: SI ratio = Sregion/SPCL. Separate 2 (group; QT ACLR, QT ACLR with LET) x 5 (time; PRE (contralateral ACL, ipsilateral QT), 3M, 6M, 12M) mixed ANOVAs with repeated measures on the last factor were employed to differentiate post-operative ligamentization metrics across timepoints and LET status at the full autograft level as well as at the segment level. Greenhouse-Geisser adjustments were made to adjust for violations to sphericity and post-hoc t-tests with Bonferroni corrections were used, as appropriate, to evaluate significant group main effects, time, as well as any group by time interactions. Cohen’s d calculations were also used to determine effect size for SI ratio of the full and four segments of the QT autograft as compared to the PRE contralateral ACL.
Results:
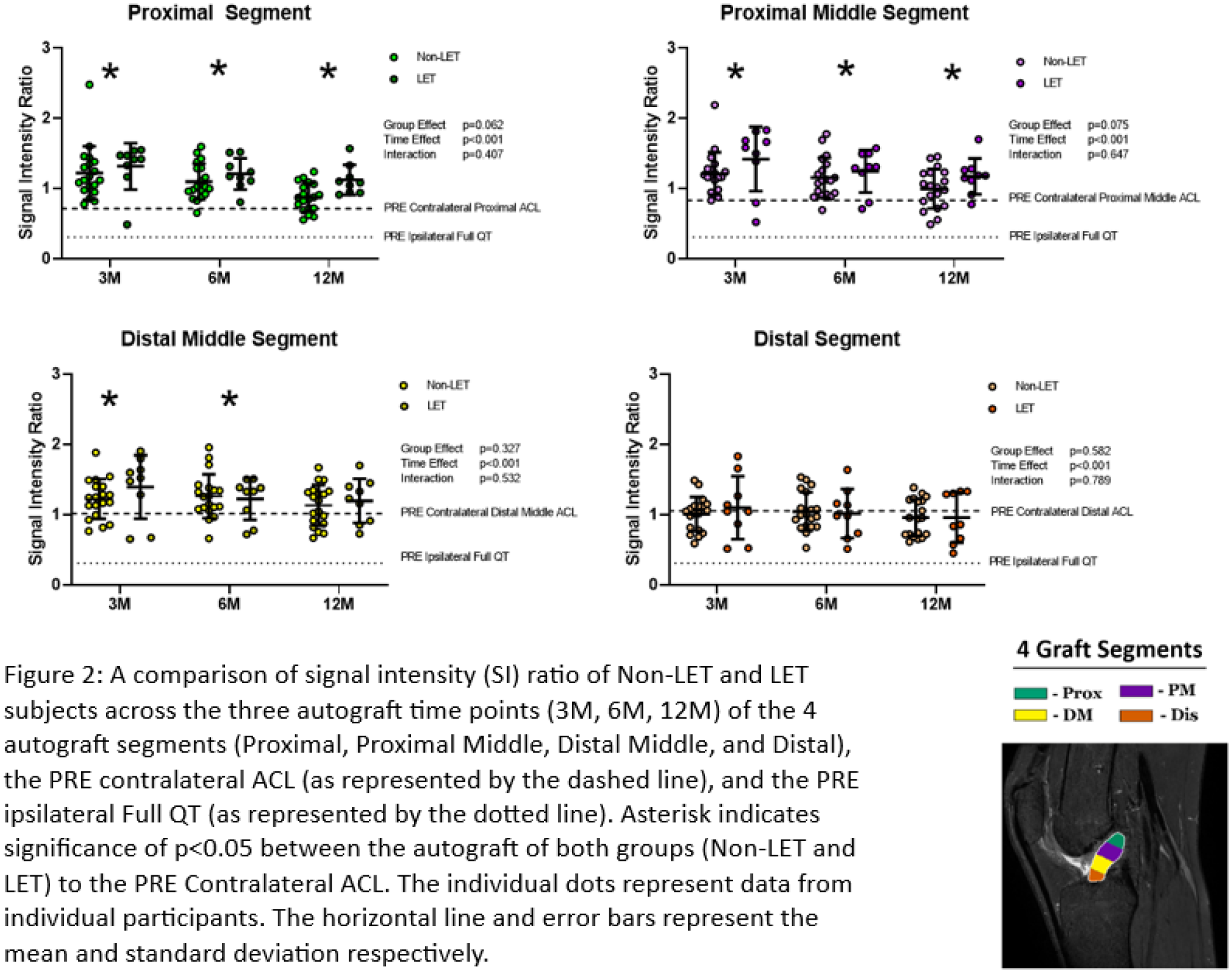
At the full autograft level, there was a significant main effect for time [(2.51, 65.27)=85.59, p<0.001, η2=0.767], but not for a group effect p=0.157 or for a group by time effect (p=0.68). Post hoc t tests indicated significant differences between the full autograft of both groups as compared to the PRE contralateral ACL at 3M and 6M (p<0.001, d=0.759; p=0.001, d=0.697 respectively) but was not different at 12M (p=0.072). At the segment level, there was again a significant main effect for time in the proximal segment [(2.01,54.58)=67.78, p<0.001, η2=0.723)], proximal middle segment [(2.329, 60.56)=74.62, p<0.001, η2=0.742], distal middle segment [(2.66, 69.27)=78.09, p<0.001, η2=0.750], and distal segment [(2.86, 74.53)=55.00, p<0.001, η2=0.679]. Post doc t-tests indicated significant differences between autograft of both groups in the proximal and proximal middle segments at all post-operative time points (proximal 3M p<0.001, d=1.079; proximal 6M p<0.001, d=1.187; proximal 12M p<0.001, d=0.816; proximal middle 3M p<0.001, d=1.009; proximal middle 6M p<0.001, d=0.896; proximal middle 12M p<0.002, d=0.653). The distal middle was also different from the PRE contralateral ACL at 3M and 6M (p=0.001, d=0.669; p=0.003, d=0.624 respectively) but not at 12M (p=0.052) and the distal segment was not different at any time point (p=0.934, p=0.893, p=0.193). Again, there was no significant group effect (proximal p=0.062, proximal middle p=0.075, distal middle p=0.327, distal p=0.582) or group by time effect for any segment (proximal p=0.407, proximal middle p=0.647, distal middle p=0.532, and distal p=0.789).
Conclusions:
The hypothesis that LET would not alter SI ratio indicating no change to autograft maturation was supported as there was no group or group by time interaction on SI ratio for either the full autograft or the four segments. However, there were significant time effects with the autograft SI ratio tending to decrease over time both of the full autograft and four segments approaching the SI ratio of the PRE contralateral ACL. The proximal most segments of the autograft have the most pronounced differences as they remain elevated throughout the post-operative timepoints while the distal most segments achieve a SI ratio that of the native contralateral ACL by 12M. These data suggest that the autograft have a maturation phase extending to 12M or beyond, especially considering the proximal aspect of autograft. Future investigations should consider larger cohorts extending past the one-year time-point to further investigate associations between SI ratio and autograft maturation, clinical failure, and revision surgery.