Abstract
Objectives:
Posterolateral tibial plateau impaction fractures commonly occur in the setting of ACL injury and have been shown to affect clinical outcomes after ACLR, but their biomechanical significance is not well understood. A recent large cohort study showed posterolateral tibial plateau fractures to occur in nearly 50% of all patients with complete ACL tears, with 8.6% of patients in the cohort having > 10% loss of lateral tibial plateau depth in the sagittal plane. Given this, the purpose of our study is to a) evaluate the biomechanical effect of increasing size of antero-posterior tibial plateau depth bone loss on knee kinematics and b) evaluate the effect of ACLR with and without a LET on knee kinematics in the setting of posterolateral tibial plateau bone loss.
Methods:
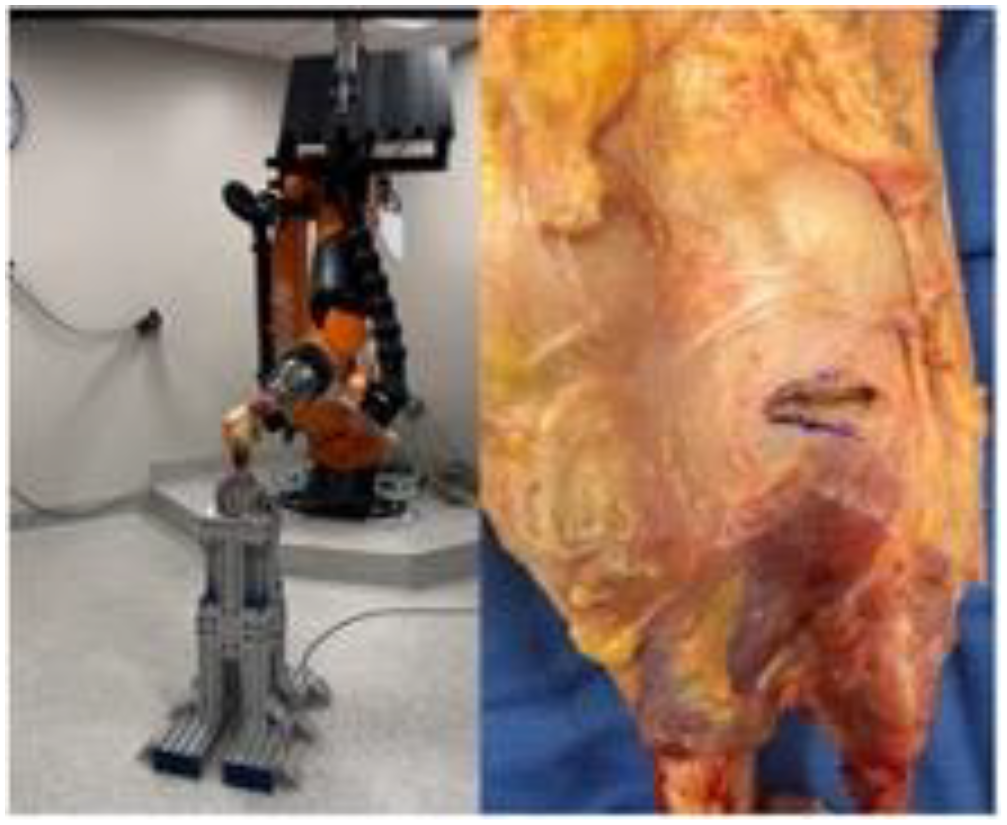
This study is a cadaveric biomechanical study using ten knee specimens. Inclusion criteria was age below 50 and no evidence of prior injury, surgical history, or gross anatomic abnormality. Femoral and tibial diaphyses were sectioned 20 cm from the joint line and potted in polymethyl methacrylate. Specimens were mounted in a custom fixture to a universal force-torque sensor (Delta F/T Transducer; ATI Industrial Automation) attached to the robotic end effector of a 6 degrees of freedom robotic system (KUKA KR 60-3; KUKA Robotics). A simulated pivot shift was conducted using the KUKA robot. An internal rotation torque of 5 Nm was applied at 15° increments from 0° to 90° of knee flexion to evaluate tibial internal rotation. The pivot-shift test was simulated by a combined 5-Nm internal rotation torque and a 10-Nm valgus torque and performed at 15° and 30° of knee flexion, and anterior tibial translation (ATT), tibial internal (IR) rotation, and valgus were measured. ATT was evaluated at 30° and 90° of knee flexion under an 88-N anterior tibial load.
The following states were tested for each specimen: 1) Intact ACL, 2) ACL deficient with no bone loss, 3) ACL deficient and 10% bone loss, 4) ACL deficient and 20% bone loss, 5) ACL deficient and 30% bone loss, 6) ACL or ACL/LET and 30% bone loss. Posterolateral tibial bone loss was created through a small horizontal posterior capsulotomy at the level of the joint line. After the final 30% lateral tibial plateau bone defect had been created, specimens either underwent an anatomic single-bundle ACLR with BTB autograft or ACLR with the addition of a modified Lemaire LET.
Statistical Analysis was performed using a one-factor, random-intercepts, mixed-effects models to compare rotation and translation during simulated pivot shift tests. Pairwise comparisons among estimated marginal means for each state were made using Tukey’s method. For all models, residual diagnostics were inspected to ensure model fit and that model assumptions were reasonably met. P-values less that 0.05 were considered statistically significant. Statistical power was considered for this experimental design, assuming a fixed feasible sample size of 10 specimens. Assuming an alpha level of 0.05, two-tailed testing, and parametric dependent groups comparisons of means, 10 specimens is sufficient to detect a between-state effect size of d=1.0 with 80% statistical power. The statistical software R version 4.4.0 was used for all plots and analyses (access date September 2, 2024; R Core Team, Vienna Austria).
Results:
A trend toward increasing ATT, IR, and valgus was observed during simulated pivot shift with increasing posterolateral tibial plateau bone loss in the ACL deficient state. There were no differences between directly sequential states (eg: ACL deficient to 10% bone loss); however, there was both increased ATT and valgus with a simulated pivot shift in the 30% bone loss group compared to the ACL deficient group without bone loss (p = .02 and p = .004) (Table 1).
As opposed to when measured during a simulated pivot shift, ATT was not different between the ACL deficient state and the 30% bone loss group (p = .52) when this was tested directly with an anterior force rather than a pivot shift force applied. With a simulated pivot-shift applied, there was no difference between the combined ACLR/LET with 30% bone loss and the intact ACL state for all biomechanical parameters, while these differences remained when comparing an isolated ACLR with 30% bone loss to the intact ACL state. Furthermore, an isolated ACLR had increased ATT, IR, and valgus with a simulated pivot-shift (p = .005, p = .05, p = .02) when compared to the ACL/LET, whereas there was no difference between the two groups in terms of ATT occurring with an anterior force rather than a pivot shift ( p = .99).
Conclusions:
With increasing amounts of posterolateral tibial bone loss, there was increased ATT, IR, and valgus that occurred with a simulated pivot shift in the presence of ACL insufficiency. These biomechanical abnormalities can be normalized with a combined ACLR and LET and are incompletely addressed with an ACLR alone.