Abstract
Objectives:
Bone patellar tendon bone (BTB) autograft is a popular graft choice for anterior cruciate ligament reconstruction (ACLR), with benefits including bone-to-bone healing, low rates of failure, and high rates of return to play. A drawback to BTB reconstruction relates to donor site morbidity, with a higher percentage of patients reporting anterior knee pain compared to hamstring and quadriceps tendon allografts.
Despite higher rates of anterior knee pain, there is little data on patellar defect size, how the patellar defect remodels over time, and how these dimensions relate to patient reported outcomes (PRO). We hypothesized that proportionally larger patella defects at the time of surgery and that patients with less robust patellar defect healing would be associated with worse PROs at 1 year follow up.
Methods:
This IRB-approved cohort study consisted of 23 participants (8 (35%) female; (mean ± std) age: 26 ± 7yrs, BMI 26 ± 4 kg/m^2) who underwent BTB ACLR by one of six surgeons from two large academic institutions. Surgeons harvested patellar grafts using their normal technique and replaced any excess bone following graft preparation. 3 Tesla knee MRIs performed according to standardized protocols were obtained for each participant at 6 weeks and 1 year post operatively. Two orthopaedic surgeons blinded to PRO agreed on measurements of each patella and defect. Knee injury and Osteoarthritis Outcome Score (KOOS) surveys were completed by 22 of the 23 participants at 1 year postoperatively.
Results:
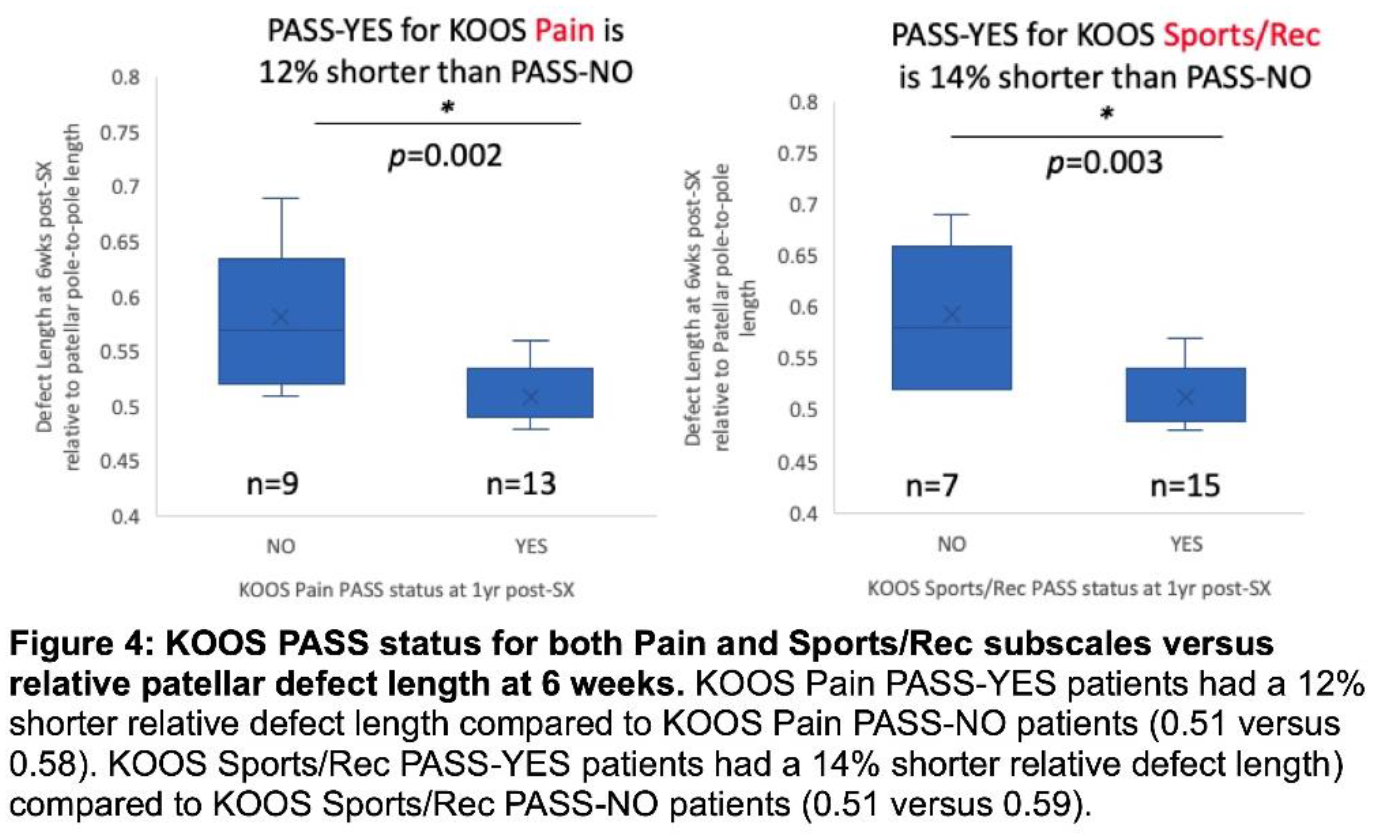
The average relative patellar defect width and depth substantially decreased from 6 weeks to 1 year (p < 0.0005) while relative patellar defect length was unchanged (Figure 1). A shorter relative defect length (Figure 2) at 6 weeks post-surgery was associated with better KOOS scores at 1 year postoperatively in KOOS subscales of Pain (p = 0.046), Activities of Daily Living (ADL) (p = 0.011), Function in Sports and Recreation (Sports/Rec) (p = 0.001), and knee related Quality of Life (QOL) (p = 0.023), and linear regression found no effects of age, sex, BMI or time from injury to ACLR on these relationships (Figure 3). Additionally, patients who achieved PASS thresholds (PASS-YES) for acceptable KOOS Pain and Sports & Recreation scores at 1yr post-ACLR had shorter relative patellar defect lengths at 6 weeks post-ACLR than those who did not (Figure 4). Those with longer relative defect lengths were also more likely to report difficulty with kneeling compared to those with shorter relative defects (p = 0.017). Of the participants with a relative defect length ≤ 0.5, 8/8 (100%) achieved PASS-YES for the Pain and Sports/Rec KOOS subscales, compared to the 14 participants with a relative defect length > 0.5, who only achieved PASS-YES in 5/14 (36%) for Pain and 7/14 (50%) for Sports/Rec. A similar higher proportion of PASS-YES was seen for participants with a relative defect length ≤ 0.5 compared to those with a relative defect length > 0.5 in the ADL subscale—6/8 (75%) versus 6/14 (43%), and the QOL subscale—7/8 (88%) versus 8/14 (57%), respectively. Changes in depths, widths, and lengths of defects between 6 weeks and 1-year post-surgery did not correlate with KOOS scores at 1 year.
Conclusions:
This study shows that shorter relative patellar defect lengths measured 6 weeks after ACLR are associated with better patient reported outcome measures at 1 year follow-up. Although patellar defect width and depth decreased between 6 weeks and 1 year after ACLR consistent with healing, these changes did not associate with patient reported outcomes. These data suggest that surgeons should consider patient size and relative patellar defect length at the time of BTB graft harvest and seek to minimize defect length while balancing the need for an adequate size bone block for the ACLR. Given that all participants with a relative defect length ≤ 0.5 achieved PASS-YES for KOOS Pain and Sports/Rec compared to 50% or less of those with a relative defect length > 0.5, a patellar bone harvest of less than half the pole-to-pole patellar length may serve as a surgically useful target.