Abstract
Objectives:
Anterior cruciate ligament (ACL) injuries are common among active patients and can be managed with primary repair or reconstruction. The most important predictor of good outcomes following primary repair is a more proximal tear location. Preoperative magnetic resonance imaging (MRI) guides surgical decision making, but its accuracy in identifying tear location is understudied. The purpose of this study was to evaluate the accuracy of preoperative MRI in identifying ACL tear location.
Methods:
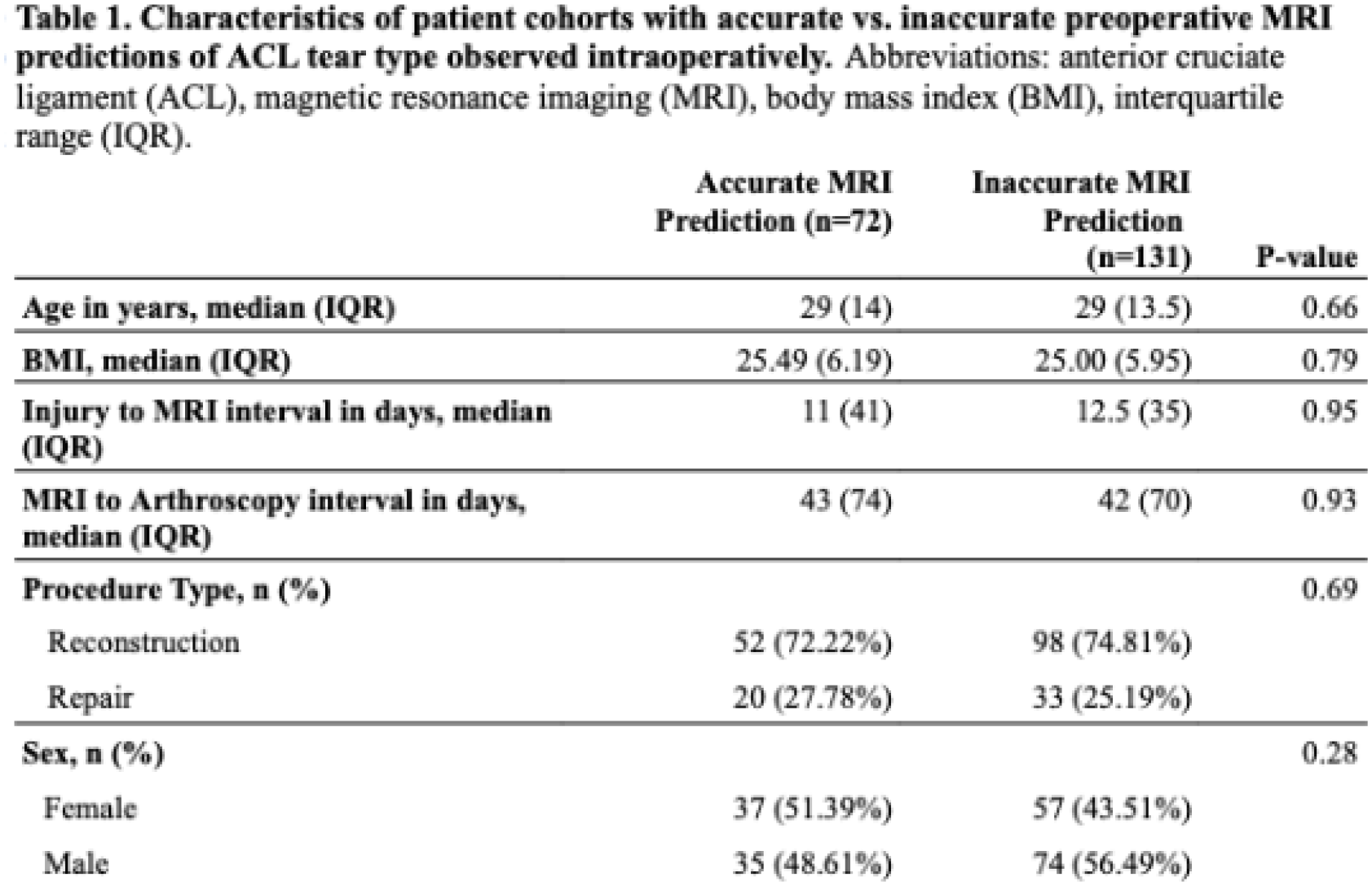
Patients who underwent ACL reconstruction or repair by two surgeons at a single, urban academic medical center from 2019-2024 were collected. Exclusion criteria included prior ACL surgery and inadequate imaging. The location of the ACL tear on preoperative MRI was retrospectively graded using the modified Sherman classification in a blinded manner by the two senior authors. Reference diagnosis was the tear location as noted in the surgeon’s operative note and confirmed with arthroscopic images. The primary endpoint was accuracy of MRI for predicting intraoperative tear type.
Results:
203 patients were included in this study. MRI accurately predicted the ACL tear type seen arthroscopically only 35.5% (72/203) of the time. When MRI did not match the arthroscopic diagnosis, the MRI was within 1 classification grade 74.8% (98/131) of the time. Of the incorrect gradings, 71.0% (93/131) of them were over-classifications (MRI tear classification more distal than found during arthroscopy). MRI was more sensitive for detecting type III (51.6%) and II (43.7%) tears than it was type I tears (2.5%).
Conclusions:
MRI is unreliable for determining the precise location of an ACL tear. MRI overestimates how distal a tear is compared to arthroscopic findings, which may influence surgical decision-making. ACL surgeons should discuss both ACL repair and reconstruction options with patients preoperatively and assess the remnant stump tissue arthroscopically prior to making a final determination.