Abstract
Objectives:
Sagittal plane malalignment is increasingly recognized as a risk factor for patellofemoral (PF) cartilage wear. While lateral cartilage lesions may be unloaded with anteromedializing tibial tubercle osteotomies (TTOs), central and medial lesions may be better addressed with pure anteriorization TTOs (aTTOs), particularly when patients have normal patellar height and coronal plane alignment (i.e., normal tibial-tubercle trochlear groove distance). Traditional aTTO techniques were associated with unacceptable complication rates, however, and there is need for aTTO techniques that may be performed more safely. The purpose of this study was to assess the relative safety and efficacy of a contemporary aTTO technique for isolated PF chondral wear.
Methods:
Consecutive patients undergoing a modern aTTO technique for isolated PF chondral wear by a single surgeon from 2016-2024 with minimum 6-month follow-up were evaluated. In brief, this previously published technique consists of an anterior-posterior cut ~5° off the vertical line, a lateral-medial cut parallel to the posterior tibial cortex, straight anteriorization of the osteotomy shingle by 10-15 mm proximally with an anterior periosteal hinge distally, and fixation by two 4.5 mm lag screws. No proximal bone block is required. Patient demographic and surgical data were collected. The primary outcome was overall complication rate, including wound complications, non-union, and fracture, among others. Secondary outcomes included range-of-motion (ROM) at six- and twelve-weeks, and patient-reported outcome measures (PROMs) at two-years (among the 28 patients with minimum two-year follow-up). Removal of hardware (ROH) is offered to all patients in our practice and not considered a complication. Comparisons were made with Student t-tests.
Results:
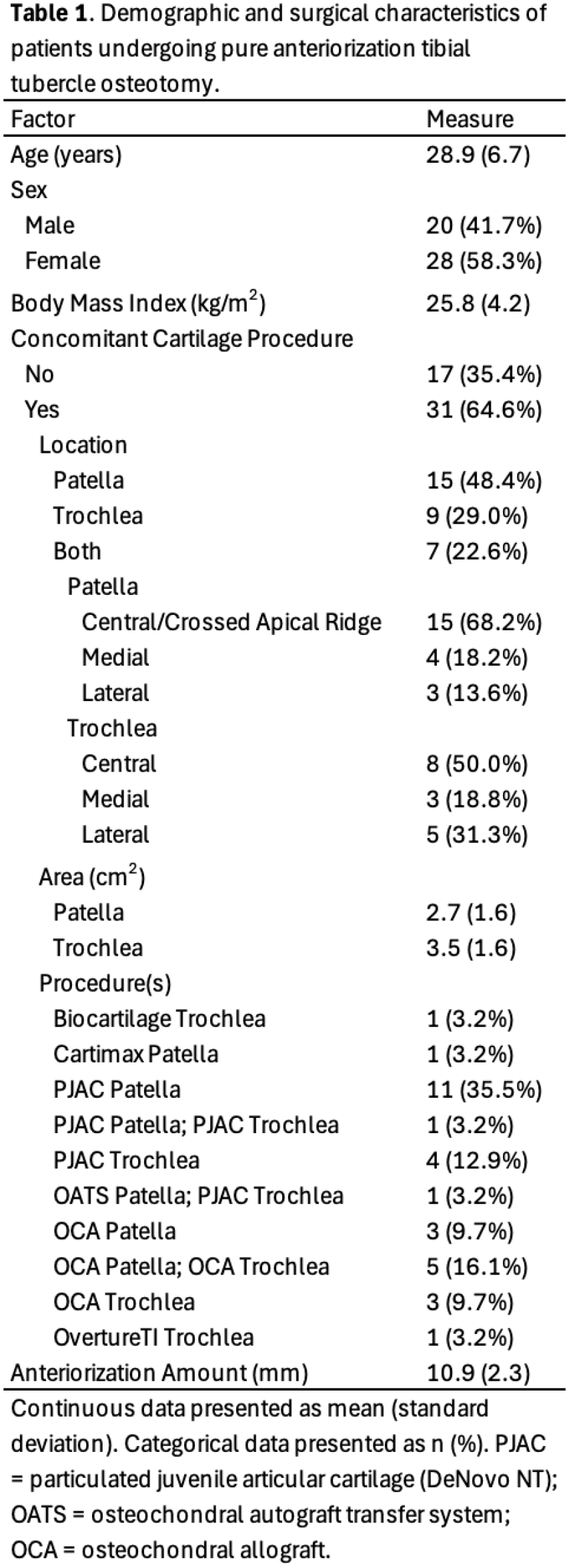
There were 48 patients with an average follow-up of 3.2 years (range 6 months-8.1 years). The mean (standard deviation) age was 28.9 (6.7) years and 58.3% of patients were women. Thirty-one (64.6%) patients underwent concomitant cartilage restoration procedures (15 [48.4%] isolated patellar, 9 [29.0%] isolated trochlear, and 7 [22.6%] to both), while 17 (35.4%) patients underwent aTTO alone. Additional patient and lesion details are presented in Table 1. The mean anteriorization amount with aTTO was 10.9 (2.3) mm. The overall complication rate was 4.2% (2 patients). This consisted of one (2.1%) manipulation under anesthesia for arthrofibrosis at 2.5 months postoperatively and one (2.1%) episode of superficial cellulitis managed with oral antibiotics alone. There were no episodes of wound dehiscence or deep surgical site infection (0%), non-union (0%), or fracture (0%). Average knee ROM was 0°-122° at 6-weeks and 0°-128° at 12-weeks postoperative. Fifteen (31.3%) patients underwent elective ROH. Among the 28 patients with minimum two-year follow-up, there were significant improvements in International Knee Documentation Committee scores from a mean 42.2 (14.0) preoperatively to 83.3 (15.7) at two-year follow-up (p<0.001). Similarly, visual analog pain scores significantly improved from a mean 4.4 (2.3) preoperatively to 1.5 (0.7) at two-year follow up (p<0.001).
Conclusions:
Anteriorizing TTO can be performed safely for isolated PF chondral lesions with low complication rates and significant improvements in PROMs. In contrast to historical results, in this cohort of 48 patients undergoing contemporary aTTO, there we no deep wound infections, fractures, or non-unions, and the overall complication rate (4.2%) was comparable or superior to other modern TTO types (e.g., anteromedializing, distalizing, etc.) as reported in the literature. Furthermore, patients experienced substantial improvement in PROMs from baseline to two-year follow-up. Moving forward, aTTO may be a safe and effective option in properly indicated patients with PF overload.